
Abstract
Objectives:
To evaluate the effect of Yugengtongyu granules on reducing the incidence of adverse cardiovascular events and improving quality of life (QOL) in patients with stable coronary artery disease (SCAD).
Methods:
A double-blind randomized controlled trial was conducted among SCAD population. One hundred fourteen patients were randomly assigned to experimental group (n = 57) and control group (n = 57) following randomized block design. Combined with the basis of standard treatment of SCAD, the experimental group and control group received Yugengtongyu granules or placebo, respectively, twice daily for 6 months and were followed for another 1 year (18 months in total from enrollment). Major outcomes (any occurrence of cardiovascular death, nonfatal myocardial infarction, or coronary revascularization), minor outcomes (any occurrence of all-cause death, ischemic stroke, readmission due to unstable angina, heart failure, or malignant arrhythmia), and composite outcomes (union of major and minor outcomes) were used to evaluate prognosis; Seattle Angina Questionnaire (SAQ) was applied to evaluate QOL, and levels of low density lipoprotein-cholesterol (LDL-C) and high sensitive C reacting protein (HS-CRP) in serum were tested.
Results:
The incidence of composite outcomes in the experimental group was significantly lower than that in the control group (3 [5.2%] vs. 11 [19.2%], hazard ratio: 0.273, 95% confidence interval: 0.080–0.926, p = 0.022); major outcomes, minor outcomes, and independent events such as nonfatal myocardial infarction showed lowering trend in experimental group. Experimental group scored significantly higher than control group in four dimensions of SAQ: physical limitation, angina frequency, treatment satisfaction, and disease perception at the third- and sixth-month follow-up; there was no significant difference in serum level of LDL or HS-CRP at all scheduled timepoints.
Conclusion:
The addition of Yugengtongyu granules based on current standard treatment reduced the incidence of composite outcomes and improved QOL in patients with SCAD.
The trial was registered in the Chinese Clinical Trial Registry (ChiCTR-TRC-13004370).
Introduction
Although established secondary prevention treatment of stable coronary artery disease (SCAD) has been proved to benefit patients, 1 residual risks of adverse cardiovascular events (ACE) still exist, 2 –5 affecting patients' prognosis and quality of life (QOL). To reduce ACE, multiple attempts have been conducted during these years. These attempts focused on anticoagulation, enhancement of low-density lipoprotein (LDL) lowering, and anti-inflammation.
In terms of anticoagulation treatment, PEGASUS-TIMI 54 Trial 6 showed benefit of prolonged double antiplatelet treatment of ticagrelor combined with acetylsalicylic acid (ASA). After a median follow-up of 33 months, the primary combined endpoint of myocardial infarction (MI), stroke, or cardiovascular death (or major adverse cardiovascular events [MACE]) was significantly reduced in ticagrelor groups compared to placebo groups (hazard ratio [HR] 0.85; 95% confidence interval [CI]: 0.75–0.96; p = 0.008). In COMPASS trial, 7 low-dose anticoagulation Rivaroxaban was added on the basis of ASA. During a mean follow-up of only 23 months, the primary endpoint MACE was significantly reduced in the ASA + rivaroxaban group (HR: 0.76; 95% CI: 0.66–0.86; p < 0.0001). However, both trials showed higher risk of bleeding (HR: 2.45 and 1.7).
On reducing residual cholesterol risk, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor, a new cholesterol lowering agent, has been proved to benefit patients. In ODYSSEY trial, 8 alirocumab was tested in SCAD patients. Result indicated that for every 39 mg/dL decrease achieved in LDL-cholesterol (LDL-C), the risk of MACE was reduced by 24% (adjusted HR: 0.76; 95% CI: 0.63–0.91; p = 0.0025). In FOURIER trial, 9 compared to placebo, evolocumab treatment significantly reduced the risk of the primary endpoint and secondary endpoint by 1.5%. However, long-term application of PCSK9 inhibitor will bring huge financial burden to patients, which hinders its popularization in the short term.
In terms of reducing residual inflammation risk, a fully human monoclonal antibody against interleukin-1β named canakinumab was tested in CANTOS trial. 10 During a median follow-up period of 3.7 years, canakinumab reduced the rate of MACE by 15%, but also led to higher incidence of fatal infection. In COLCOT trial, 11 low-dose colchicine was proved to benefit patients after acute MI reflected by reducing primary endpoints (HR, 0.77; 95% CI: 0.61–0.96; p < 0.02). However, similar conclusion was not acquired among SCAD patients. 12 Moreover, none of the strategies above provided a perfect balance of efficacy, risk, and costs. Therefore, a safe and effective method to reduce residual risk in SCAD patients is urgently needed.
In China, Traditional Chinese Medicine (TCM) has been applied to treat CAD for more than 2000 years. TCM emphasizes individualized treatment and mainly focuses on relieving symptoms. As research principles of evidence-based medicine (EBM) were introduced to TCM study, TCM practitioners began to put more attention on improvement of prognosis. 13 –15 TCM is widely applied in China, however, still lacks evidence which conforms to requirement of EBM.
Yugengtongyu (means healing infarction and clearing stasis) decoction was created based on the “Deficiency-Stasis-Toxin-Phlegm” TCM pathogenesis theory (DSTP theory) of CAD. It is composed of 11 kinds of herbs. According to previous clinical observation, Yugengtongyu decoction improved angina symptoms in patients with SCAD 16 and reduced the serum cholesterol level. Besides, the authors have noticed that Yugengtongyu decoction reduced the incidence of hospitalization attributed to ACE, but there's no published evidence.
To popularize the use of Yugengtongyu decoction, a new version, Yugengtongyu granules, was created. The dosage form was transferred into granules, and the composition was minimized to five kinds of herbs: Astragalus membranaceus (Huangqi), Salvia miltiorrhiza Bunge (Danshen), Ligusticum chuanxiong Hort (Chuanxiong), Agastache rugosus (Huoxiang), and Coptis chinensis (Huanglian). This double-blind randomized controlled trial was conducted to verify Yugengtongyu granules' efficacy on improving prognosis and QOL in CAD patients.
Design
This double-blind randomized controlled clinical trial was conducted in China-Japan Friendship Hospital (Beijing, China) from 2014 to 2018. This study was designed according to guidelines of the Declaration of Helsinki for human research, and study protocol was approved by the Ethics Committee of China-Japan Friendship Hospital. Informed consent was obtained from all individual participants included in the study. Supplementary Data show the flow chart of this trial.
Participants
Patients who met following criterion were enrolled: (1) The diagnosis of SCAD was made according to 2013 ESC guidelines on the management of stable coronary artery disease 17 ; (2) aged 18–75 years; (3) had two or more of the following four conditions: serum high sensitive C reacting protein (HS-CRP) level >3 mg/L, history of hypertension (HT), hyperlipidemia, and diabetes mellitus (DM). Patients with congenital heart disease, rheumatic heart disease, severe heart failure (HF), an uncontrolled severe arrhythmia, uncontrolled HT, severe hepatic/renal/hematologic disease, severe mental disorders, or participating in other studies were excluded.
Assignments, randomization, masking, and blinding
Through a computer-generated, block randomization schedule, serial numbers were randomized in a 1:1 ratio and assigned to experimental group or control group. From the lowest to highest number, every 6 sequentive numbers composed 1 block, in which the amount of numbers assigned to experimental group or control group were equally 3. The order within each block was determined by random number table method, forming random sequence. (Detailed randomization schedule is shown in Supplementary Data). The package of drug or placebo was labeled by the serial numbers. On recruiting, each patient will be assigned the lowest available number. The random sequence was kept by database administrator and hidden from others, so that patients, physicians, and statisticians were blind to treatment assignment until the database was unlocked.
Intervention treatment and control treatment
Patients assigned to experimental groups received Yugengtongyu granules, including Astragalus membranaceus [Huangqi] 7.5 g, Salvia miltiorrhiza Bunge [Danshen] 7.5 g, Ligusticum chuanxiong Hort [Chuanxiong] 5 g, Agastache rugosus [Huoxiang] 5 g, and Coptis chinensis [Huanglian] 2.5 g. Each of the five herbs was produced and packed in a single batch by China Resources Sanjiu Medical and Pharmaceutical Co., Ltd., Shenzhen, China. On taking, mix five herbs with hot water orally twice daily for 6 months. Patients assigned to control group received placebo (composed of 90% starch and 10% of crude drug of Yugengtongyu granules, identical in color, smell, and appearance to Yugengtongyu granules) for 6 months. Besides, all patients received standard fundamental treatment based on SCAD clinical guidelines. 17
Follow-up and clinical evaluation
All the participants were followed at 3rd, 6th, 12th, and 18th month after enrollment. During each follow-up, primary endpoints (ACE), including major outcomes, minor outcomes, and composite outcomes, were assessed. The major outcomes comprised cardiovascular death, nonfatal myocardial infarction, and coronary revascularization. The minor outcomes were all-cause death, ischemic stroke, and readmission due to unstable angina (UA), HF, or malignant arrhythmia. Composite outcomes were defined as the union of major outcomes and minor outcomes (all the ACE mentioned above).
To quantify the QOL, the secondary endpoint Seattle Angina Questionnaires (SAQs) were introduced, in which five independent dimensions of angina (physical limitation [PL]; anginal stability; anginal frequency [AF]; treatment satisfaction [TS]; and disease perception [DS]) were evaluated quantitatively. 18 Serum levels of HS-CRP and LDL-C were compared between the experimental group and the control group at 3rd, 6th, and 12th month, respectively. Safety variables, including major bleeding, reduction of white blood cell or platelet, and liver and kidney function damage, were also assessed at scheduled timepoints.
Statistical analysis
PASS 11.0 software was applied in sample size estimating. Because incidence of ACE data is binary structure, the method of “Test for two proportions” was used. The authors defined the rate of composite outcomes (P1) as 34.5% according to epidemiology data from previous study, 4 as well as database of recruiting hospital. Based on previous single-arm observation study conducted by their team (unpublished), Yugengtongyu granules reduced the incidence rate of composite outcomes (P2) to 11.1%. A sample of 96 would be sufficient with α level of 0.05 and 1-β level of 0.8. Considering the maximum dropout rate of 20%, the authors decided to recruit 114 participants in this research.
Dropout participants were interviewed through telephone or online at scheduled timepoints to acquire information of ACE incidence until unblinded. Last observation carried forward method was applied to impute missing values. Following intention-to-treat (ITT) principle, data of all patients were analyzed according to the initial allocation, despite dropouts.
SPSS 20.0 software was applied for statistical analysis. Continuous variables were analyzed by two sample t test (mean ± SD) or Mann–Whitney U test (median [interquartile range]) according to whether they conformed to the normal distribution. Categorical variables were presented as frequency (percentage) and compared by Chi-square test. Kaplan–Meier curves were used to compare incidence of primary endpoints between groups. Following statistical principles, 19 because the estimated amount of ACE was no larger than 10-folds of covariate amount, adjusted baseline was not suitable for analyzing ACE incidence. For all analyses, two-sided p-values were used, and p < 0.05 was defined to be statistically significant.
Results
Participant process
Figure 1 shows the participant process.

Flow chart of participant process, including numbers of participants that received randomization, intervention/control treatment, finishing follow-up and included in analysis of primary endpoints.
Recruitment and baseline
From December 2014 to April 2016, 114 participants were enrolled and randomly assigned to experimental group (n = 57) and control group (n = 57). By the end of last follow-up, 43 patients in experimental group and 48 patients in control group cooperated well with follow-up. The total dropout rate was 20.1%, and there was no significant difference between groups (p = 0.24). Detailed dropout reasons are introduced in Supplementary Data.
Between groups, baseline characteristics were similar (Table 1). Among all the participants, 78.1% were male, and the average age was 61.56 ± 8.37. In terms of risk factors, 56.1% of participants had a history of MI, 64.9% with a history of HT, 91.2% with dyslipidemia, 35.1% with DM, 13.2% with stroke, and 15.8% with peripheral artery diseases; 30.7% of participants were current smokers. As for baseline of inflammation and serum cholesterol markers, median HS-CRP level was 1.18 (0.55, 1.92) mg/L, and average LDL-C level was 2.24 ± 0.62 mmol/L. In terms of drug intake, none of CAD medications, including antiplatelet agents, lipid-lowering agents, inhibitor of the renin–angiotensin system, beta-blocker, or nitrates, showed difference between groups, indicating that there's no relation between the use of different “standard fundamental treatment” and different clinical outcomes.
Baseline Characteristics of Experimental Group and Control Group
Categorical variables are expressed as the number of cases (percentage); numerical variables are expressed as mean ± standard deviation or median (interquartile range).
ACEI, angiotensin-converting enzyme inhibitor; ADP, adenosine diphosphate; AMI, acute myocardial infarction; ARB, angiotensin receptor blocker; CABG, coronary artery bypass graft; DAPT, double antiplatelet treatment; LDL-C, low density lipoprotein-cholesterol; PAD, peripheral artery disease; PCI, percutaneous coronary intervention.
Effect on reducing ACE
The authors managed to get in contact with all dropout participants and acquire their information of ACE incidence. The incidence of composite outcomes was significantly lower in experimental group than control group. The major outcomes occurred in two and five patients in experimental and control group, respectively. For minor outcomes, the occurrence was one and six. Despite lack of statistical significance, both major and minor outcomes showed decreasing trend in experimental group. Figure 2A–C shows Kaplan–Meier curves of cumulative event incidence of composite, major, and minor outcomes.
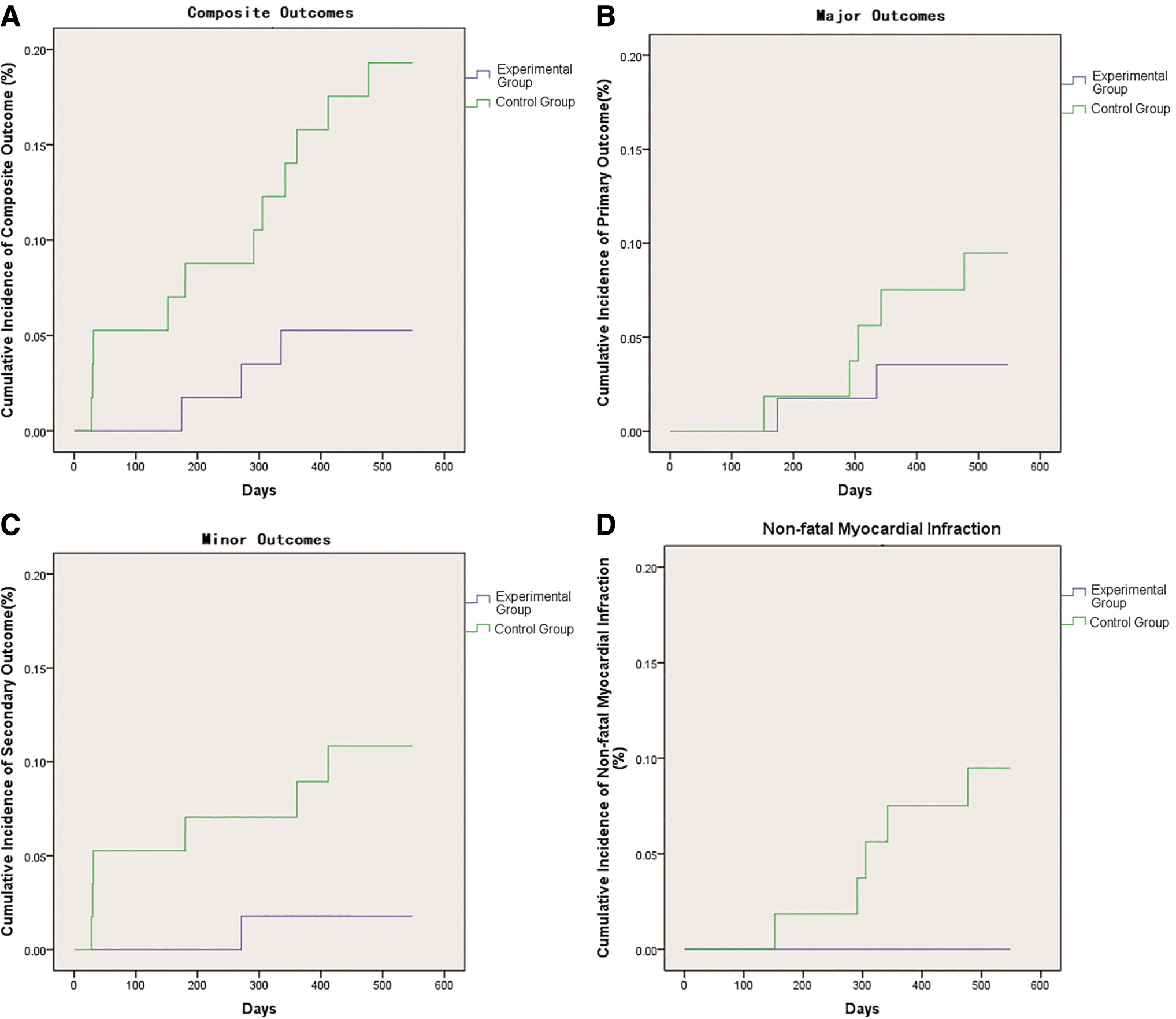
Kaplan–Meier curves of cumulative event incidence of endpoints;
Table 2 shows classification and specific type of outcome. Nonfatal MI incidence in experimental group was lower than that in control group (0 vs. 5 [8.77%], p = 0.067), where Kaplan–Meier curve also reflects the result in Figure 2D. Other independent outcome events showed no statistical difference between groups.
Comparison of Outcome Events Between Groups
CI, confidence interval; HF, heart failure; MA, malignant arrhythmia; MI, myocardial infarction; UA, unstable angina.
Effect on improving QOL
Multiple dimensions of SAQ showed improvement of QOL in experimental group compared to control group (Table 3). At the third month time point, score of AF and TS dimensions was significantly higher in experimental group than control group. At the sixth month time point, scores in PL, AF, and DS dimensions manifested statistical difference between groups. However, none of dimension score showed statistical difference at 12-month follow-up.
Seattle Angina Questionnaire Scores of Five Dimensions
p-Value refers to comparison between groups at the timepoint and dimension; * p < 0.05; ** p < 0.01.
Effect on level of LDL-C and HS-CRP
Between experimental and control groups, the difference of HS-CRP showed an increasing-decreasing trend, but there was no significant difference at all scheduled timepoints. The same trend also occurred in serum LDL level (Fig. 3).
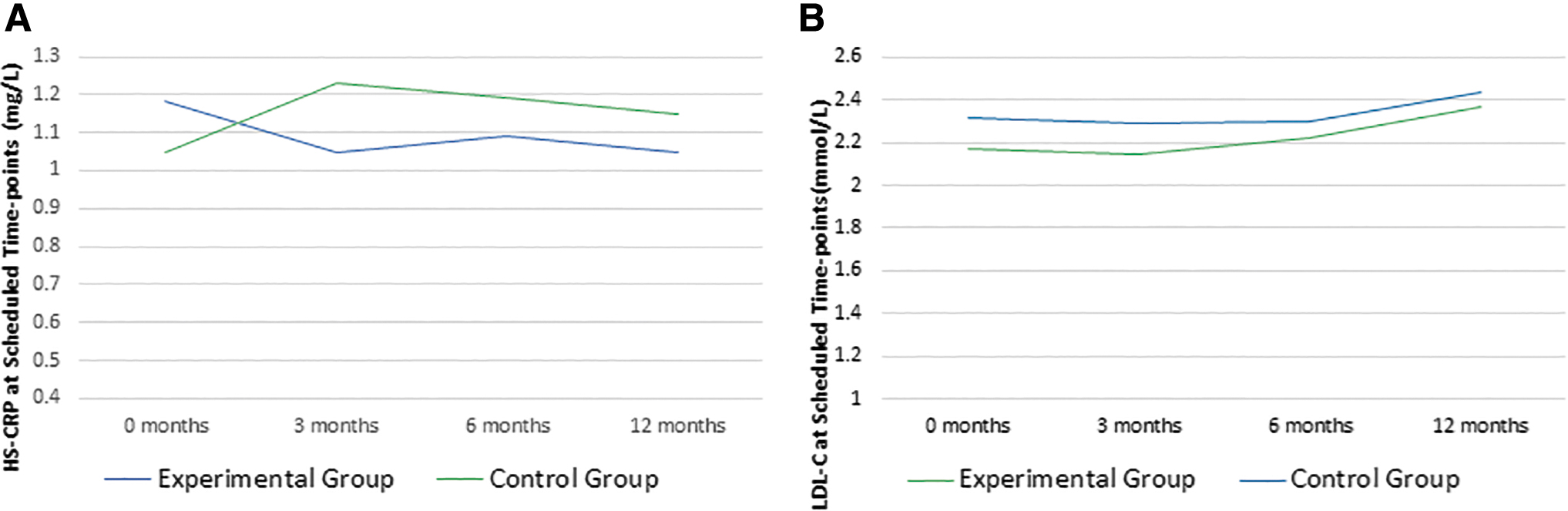
Serum level of
Safety
During the follow-up of 1 year, a total of 11 safety events occurred (4 vs. 7 in experimental group and control group, HR: 0.57, 95% CI: 0.17–1.84; p = 0.34). The most frequent event was constipation (two events), and other events were considered not related to Yugengtongyu treatment. No major bleeding occurred, and no increasing risk of liver injury, kidney injury, reduction of platelet, inflammation, and coagulopathy was observed in this trial (detailed safety information is listed in Supplementary Data).
Discussion
Efficacy on improving prognosis
From the results showed above, the authors primarily achieved the purpose of this trial, to prove the effect and safety of Yugengtongyu granules on improving the prognosis of SCAD patients, reducing ACE rate of composite outcomes. Although major outcomes, minor outcomes, and nonfatal MI were not statistically different, the overall results were gratifying. In this trial, all the patients were treated on the basis of standard and adequate secondary prevention. Based on this, Yugengtongyu granules reduced composite outcomes to some extent, providing a promising treating method for reducing the residual risk of SCAD.
The difference of total ACE incidence between groups (5.26% vs. 19.29%) indicated success. However, this result should also be treated rationally. First, according to statistical principles, the actual value of HR might be any value within the 95% CI, instead of the fixed value of 0.273. Obviously, the range of 95% CI was relatively wide in this result (0.080–0.926). Second, it is composite outcomes that manifested difference, in which minor outcomes constituted a large proportion of the total incidence. However, statistical significance was not found in major outcomes, which were believed to be better reflecting the effect of experimental drugs.
Although the incidence of events was significantly lower in experimental group, there were varied factors that may affect the result.
First, on evaluating sample size, the values of P1 (estimated incidence rate in control group) and P2 (estimated incidence rate in experimental group) were higher than other studies. The authors defined P1 and P2 as the incidence of composite outcomes (minor outcomes were included) instead of pure major outcome incidence; therefore, the sample size could be minimized. Under this condition, the impact generated from random errors might be magnified. Fortunately, the results turned out to meet their expectation on P1 and P2 and showed that only composite outcome incidence manifested statistical significance. If the sample size was calculated based on the P1/P2 value of pure major outcomes, which might help to enlarge the sample size and narrowing the 95% CI, the efficacy of Yugengtongyu granules might be better proved.
Second, due to the fact that ITT principle was used in statistical analysis, 20 compliance factors were not fully considered. For example, participant No.309 was one of those patients with a minor outcome. She refused to continue experimental treatment 30 days after enrollment because of personal reason, but she was hospitalized due to UA on the 361st day. Obviously, she was not under the protection of Yugengtongyu treatment, but still she was included in the analysis as experimental group. In terms of this, the efficacy of Yugengtongyu granules might be underestimated.
Efficacy on improving QOL
Yugengtongyu granules also manifested great effect on improving QOL. Difference between groups in PL, AF, TS, and DS dimensions of SAQ appeared in third and sixth month and disappeared in 12th month. Among all five dimensions, the improvement of PL (reflecting PL due to angina) and AF (reflecting the frequency of angina) is most meaningful, because they directly reflect severity of angina symptoms. At the same time, the authors found that these two dimensions improved during treatment and returned to baseline after treatment, which was in accordance with therapeutic phase. This strongly proved the efficacy of Yugengtongyu granules on improving angina symptom.
Although a variety of complementary and alternative medicine treatments are believed to be able to alleviate SCAD symptoms, most of them are considered to be placebo effects 21 due to the inability to provide evidence. In this study, a placebo double-blind design was used to eliminate the influence of the placebo effect, thereby providing evidence for Yugengtongyu granules to improve QOL.
The improvement of QOL also contributed to the decreasing incidence of secondary outcomes. The improvement of angina symptom led to the decline of readmission due to UA (a subset of composite outcomes), and in this trial, respectively, zero and six patients in experimental group and control group was hospitalized due to UA. This might be able to explain why there's such a huge difference in composite outcome incidence between groups.
Exploration of mechanism
Initially, the authors hoped to figure out the specific mechanism of Yugengtongyu granules on improving patients' prognosis. By analyzing the composition of Yugengtongyu granules, the authors found that multiple pharmaceutical ingredients have anti-inflammatory effect. 22 –25 Therefore, the authors assumed that Yugengtongyu granules could inhibit inflammation, reflected by reduction of HS-CRP level. Unfortunately, despite an expectant trend, HS-CRP showed no significant difference between groups. The result of LDL level didn't give us surprise either.
These results may be related to the setting of inclusion criteria. For example, in CANTOS trial, a HS-CRP level of 2 mg/L or more was mandatory item. Therefore, a trend that canakinumab caused a dose-dependent decrease in HS-CRP levels was observed. In this trial, high level of LDL and HS-CRP is not mandatory on recruiting. Therefore, even if Yugengtongyu granules can reduce the level of the two, it is difficult to make a difference on a low baseline value.
Another possible explanation is that Yugengtongyu granules may have multiple coordination mechanisms, for example, improving endothelial function. Maintaining normal endothelial function is essential for plaque stability and inhibiting plaque progression. Among the five herbs of Yugengtongyu granules, active ingredients of four herbs: Astragalus, Salvia, Ligusticum, and Coptis have been proved to be effective on maintaining endothelial function. To examine endothelial function, flow-mediated dilation (FMD), a noninvasive method, has been widely used. The authors tested FMD in some patients taking Yugengtongyu granules and got preliminary results showing that Yugengtongyu granules increased FMD value, indicating the improvement of endothelial function. This mechanism will be further confirmed in subsequent studies.
Limitations
There are some limitations in this trail. Considering that the occurrence of outcomes reflects the protection efficacy of medications in a former period of time, design of 6 months of treatment followed by 12 months of observation was introduced in this trial. Unfortunately, the authors didn't get a time point that the protection efficacy was completely eliminated. Limited observation time might be the reason. Besides, the dropout rate was relatively high and may affect multiple results except ACE incidence. Finally, the authors didn't explore deeply into the mechanism of Yugengtongyu granules' efficacy.
Conclusion
The addition of Yugengtongyu granules based on current standard treatment reduced the composite outcomes and remarkably improved QOL in patients with SCAD.
Footnotes
Authors' Contribution
Authors contributed to research protocol design (D.W., C.L., X.X., H.X., L.H.), enrollment and investigation (D.W., H.X., C.G., J.W., J.G.), data acquisition, analysis (D.W., X.X.), or interpretation (D.W., C.L., and L.H.), drafting the article (D.W., C.L.), funding acquisition (L.H.), and critically revising the article (D.W., C.L., X.X., H.X., and L.H.). All authors read and gave final approval for the final article.
Acknowledgments
The authors appreciate Dr. Lin Li who works in China-Japan friendship hospital and Wenhua Peng who works in Beijing University of Chinese Medicine Affiliated Dongzhimen Hospital for their help in enrollment. The authors also thank National Science and Technology Support Program and National Key Research & Development Program for the funding.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
National Science and Technology Support Program of China (Grant Number: 2013BAI02B01); National Key Research & Development Program of China (Grant Number: 2017YFC1700103).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.