
Abstract
Objectives:
Implementation science is key to translating complementary and integrative health intervention research into practice as it can increase accessibility and affordability while maximizing patient health outcomes. The authors describe using implementation mapping to (1) identify barriers and facilitators impacting the implementation of an Integrative Medical Group Visit (IMGV) intervention in an outpatient setting with a high burden of patients with chronic pain and (2) select and develop implementation strategies utilizing theory and stakeholder input to address those barriers and facilitators.
Design:
The authors selected a packaged, evidence-based, integrative pain management intervention, the IMGV, to implement in an outpatient clinic with a high burden of patients with chronic pain. The authors used implementation mapping to identify implementation strategies for IMGV, considering theory and stakeholder input. Stakeholder interviews with clinic staff, faculty, and administrators (n = 15) were guided by the Consolidated Framework for Implementation Research.
Results:
Based on interview data, the authors identified administrators, physicians, nursing staff, and scheduling staff as key stakeholders involved in implementation. Barriers and facilitators focused on knowledge, buy-in, and operational procedures needed to successfully implement IMGV. The implementation team identified three cognitive influences on behavior that would impact performance: knowledge, outcome expectations, and self-efficacy; and three theoretical change methods: cue to participate, communication, and mobilization. Implementation strategies identified included identifying and preparing champions, participation in ongoing training, developing and distributing educational materials, and organizing clinician implementation team meetings.
Conclusions:
This study provides an example of the application of implementation mapping to identify theory-driven implementation strategies for IMGV. Implementation mapping is a feasible method that may be useful in providing a guiding structure for implementation teams as they employ implementation frameworks and select implementation strategies for integrative health interventions.
Introduction/Background
Implementation science in complementary and integrative health interventions
The National Center for Complementary and Integrative Health has invested heavily into rigorously evaluating health interventions, many of which target chronic pain. 1 While growth of the evidence base has prompted widespread implementation of complementary and integrative health interventions within the Veteran's Health Administration, 2 civilian health care settings have not seen the same therapeutic shifts, leaving many efficacious treatments inaccessible to populations at risk for chronic pain. 3 Implementation science methods are ideally suited to translating complementary and integrative health intervention research into more widespread practice. 4 Implementation science has been defined as the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice and, hence, to improve the quality and effectiveness of health services and care. 5 Increasingly, the National Center for Complementary and Integrative Health is expressing interest in growing their implementation science portfolio. 6
Integrative pain management (IPM) interventions include a range of complementary and integrative health therapies such as mindfulness, yoga, Tai Chi, qigong, and other noninvasive techniques. 7 –10 Many of these approaches are proven to be just as effective, if not more so, in managing chronic pain symptoms compared with other self-care therapies. 11 Several IPM interventions are now recommended as first-line treatments in clinical guidelines for chronic pain conditions, and the Joint Commission has required that accredited health care facilities provide IPM therapies. 12,13 Yet, biomedical health care systems' provision of IPM therapies is limited by the absence of staff with expertise in IPM and lack of remuneration for the delivery of many IPM services. 14 For instance, in most cases, neither public nor private insurance fully covers therapies such as mindfulness-based stress reduction, yoga, Tai Chi, and massage. 15 The current challenge is how to best overcome these challenges to promote and support the implementation of IPM interventions into widespread practice.
The production of evidence alone does not directly lead to the uptake of new interventions, and there is a significant gap (up to 17 years) between generation of research findings and their translation to patient care. 16 Implementation science offers methods, theories, and frameworks to help close the gap between research and practice. This gap is addressed by developing and testing implementation strategies that specifically target the educational, financial, logistical, organizational, and structural barriers to a new intervention. Implementation science methods marry rigorously researched interventions with the development of strategies needed to incorporate interventions into health care settings. When effective, implementation strategies improve access to evidence-based interventions.
Implementation mapping
Implementation science distinguishes between interventions (also referred to as evidence-based interventions or the “thing” being implemented) and implementation strategies (which are used to facilitate the uptake of the intervention). 17 Implementation strategies describe how interventions are applied in a clinical setting, 18 detailing logistical measures such as how to recruit participants into an intervention, who should be responsible for running the intervention, and how the intervention should be maintained. Implementation strategies facilitate optimal incorporation by targeting barriers such as provider attitudes, patient knowledge, community norms, organizational policies, and finances. 19 Implementation scientists have developed frameworks aimed at characterizing barriers and facilitators to implementation (e.g., the Consolidated Framework for Implementation Research [CFIR]) 20 and compilations of implementation strategies for use in targeting those barriers and facilitators (e.g., Expert Recommendations for Implementing Change compilation [ERIC]). 21 However, the field has not achieved consensus on which implementation strategies should be used to address specific barriers or facilitators. 22 Implementation mapping offers a systematic process for selecting the implementation strategies needed to overcome barriers to implementation by considering relevant behavioral theories and stakeholder input. 23 Utilizing a systematic process enhances replicability, while utilizing relevant theory enhances the potential to identify mechanisms of action of implementation strategies. Both replication and identifying mechanisms are key to enhancing the rigor of implementation science. 22
Implementation mapping is based upon and closely mirrors intervention mapping, a process for designing health behavior interventions. This method typically involves five tasks: (1) construct a needs assessment that identifies barriers and facilitators as well as actors who will address those barriers and facilitators; (2) state steps to implementation; (3) select and design implementation strategies; (4) produce implementation strategy materials; and (5) assess implementation outcomes. 19 Using implementation mapping, researchers first engage with stakeholders (such as clinicians, health care employees, or community members) to identify implementation barriers and recognize facilitators at multiple levels. Following stakeholder engagement, steps to implementation are developed that clearly specify who needs to do what to address the identified barriers and facilitators. Relevant behavioral theories are then identified and the implementation team (engaging both research and practice stakeholders) begins to select and design implementation strategies to build on the selected theories to overcome barriers and identify the steps to implementation. Finally, implementation strategies are executed and evaluated. The implementation mapping process is iterative and allows the implementation team to construct and review implementation strategies based on literature, behavioral theories, and stakeholder input.
Implementation science can support the adoption of IPM therapies in diverse settings; however, it has not been extensively described within the scope of complementary and integrative health. 24 Prior research suggests that multiple factors impede the implementation of IPM interventions, 25 yet little work has been done to systematically identify implementation strategies for IPM. In this article, the authors provide a model of how implementation science techniques can be applied to the study of IPM interventions. The authors describe using implementation mapping tasks 1–4 to (1) identify factors impacting the implementation of an IPM intervention—the Integrative Medical Group Visit (IMGV)—in an outpatient setting and (2) select and develop implementation strategies to address those factors. In the fifth task of implementation mapping, the implementation strategies developed here will be evaluated for feasibility and acceptability in a pilot study.
Materials and Methods
The authors selected a packaged, evidence-based IPM intervention, the IMGV, to implement in an outpatient clinic with a high burden of patients with chronic pain. Patients at the clinic had previously expressed the desire for increased access to complementary and integrative health services, and leadership at the clinical site was interested in developing IPM services that could be billed to patients' insurance. 26 IMGV is one of few IPM interventions that is widely reimbursable and was therefore selected as part of a larger effort to develop a financially sustainable Integrative Medicine Clinic. 27 In this study, the authors describe the IMGV intervention and implementation mapping process used to identify relevant implementation strategies. This project was reviewed by the Institutional Review Board of the University of North Carolina at Chapel Hill, protocol number 20-0147. The Institutional Review Board determined that these activities did not meet criteria for human subject research under federal regulations and therefore did not require approval.
Integrative Medical Group Visits
The IMGV is an innovative approach to IPM combining a medical group visit format, mindfulness-based stress reduction, pain education, acupressure, self-massage, and other evidence-based, integrative medicine therapies for patients with chronic pain in a billable model. 28 –31 IMGVs usually consist of 8 to 12 patients meeting as a group in the same room and are run by a billing clinician (MD, DO, NP, or PA) and a mind–body instructor (mindfulness-based stress reduction teacher or yoga instructor). During the visits, the clinician provides program participants with individualized medical attention, education, self-management, self-monitoring, and support, while the mind–body instructor guides experiential activities.
IMGVs significantly reduce emergency department visits among patients with chronic pain, decrease pain medication usage, and increase patient mental and emotional well-being. 32 IMGV participants may experience a greater amount of social and emotional support than they would in individualized medical appointments and often report a greater quality of life. 33 Clinicians consistently report that group medical visit programs allow them to participate in a community of support, develop more personal relationships with their patients, and gain insight from patients with chronic conditions. 34
IMGV allows a diverse group of patients to access integrative therapies in a format covered by insurance. The IMGV for chronic pain is one of few efficacious IPM interventions to address the lack of access to complementary and integrative health therapies due to financial barriers; however, it has been only minimally implemented. 27,35
Implementation mapping
The authors used implementation mapping tasks 1–4 to identify implementation strategies for IMGV while considering theory and stakeholder input (Fig. 1). The principal investigator (I.J.R.) led the implementation mapping process in partnership with an engaged team of both research and practice-based stakeholders. The team included a physician trained in qualitative methods, a senior implementation scientist, a physician/researcher who developed the IMGV, a physician trained in IPM, three IPM researchers, and a research assistant.
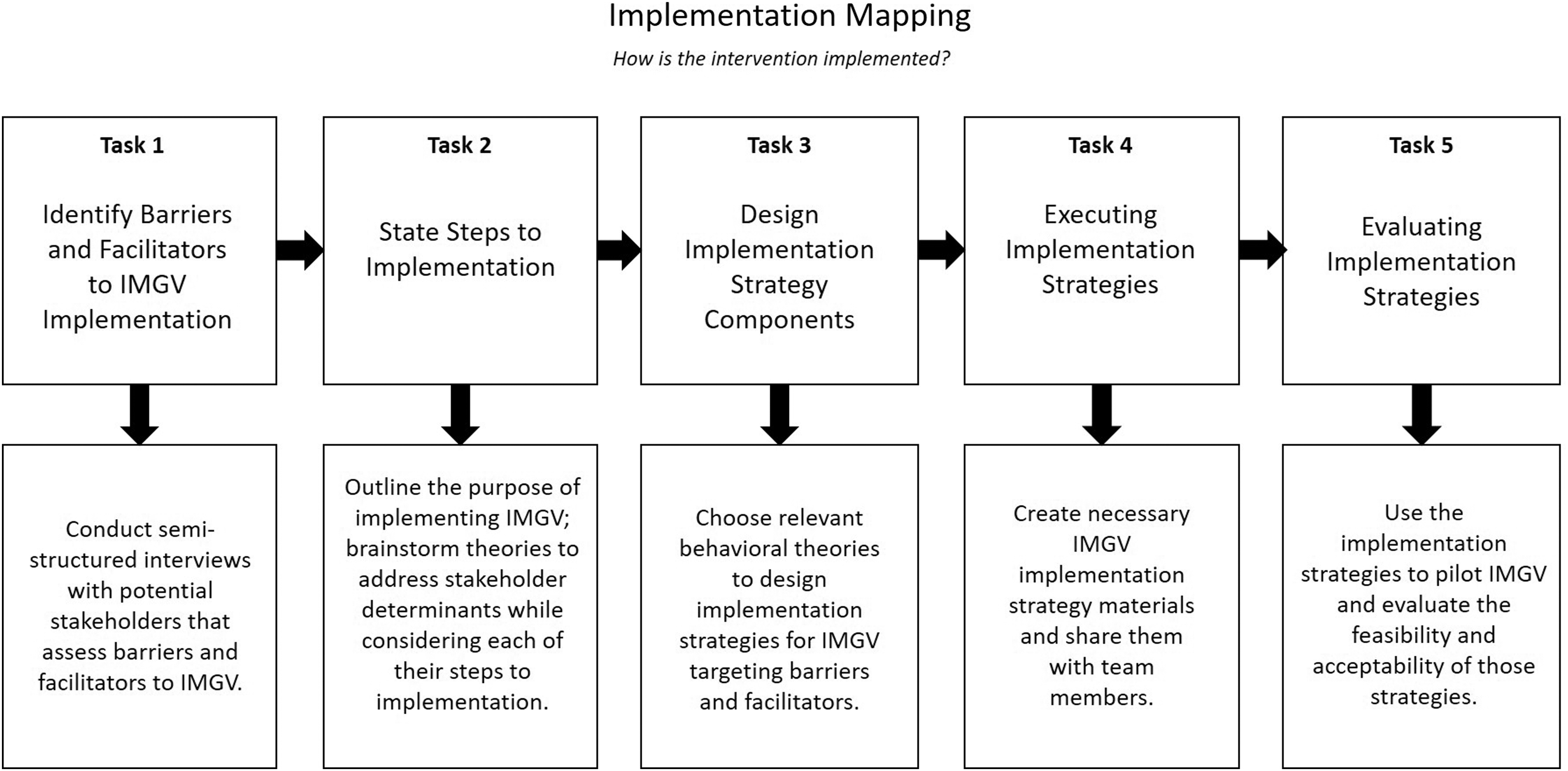
Implementation mapping for IMGV. Implementation mapping consists of five tasks aimed at selecting and evaluating relevant implementation strategies using relevant theory and stakeholder input. IMGV, Integrative Medical Group Visit.
Task 1. Identify barriers and facilitators to IMGV implementation
In the first task, the authors assessed the needs of the clinical context, identified program adopters and implementers, and identified potential barriers and facilitators to IMGV implementation. The planning team held a brainstorming session to identify the following: 1) Who will be involved in making the decision to adopt IMGV? 2) Who will implement the program? Who will be involved in implementation? Who will the implementation impact? While originally planned to be informal and conducted in person, due to the COVID-19 pandemic, all interviews were scheduled in advance and conducted through Zoom teleconference. After identifying a list of potential stakeholders, the authors sent e-mail invitations for virtual interviews to 22 stakeholders. Semistructured interviews with clinicians, staff, and administrators (n = 15) were conducted. Nonrespondents included six clinicians and one staff member. Participants included eight clinicians, three staff members, and four administrators. All interviews were conducted in English, recorded, and no compensation was provided to participants for their participation. All interviews were conducted at one clinical site.
The authors developed an interview guide informed by the CFIR, an implementation framework used to identify multilevel factors (i.e., determinants) that may influence successful implementation. 36 The CFIR organizes determinants within five domains or levels: characteristics of intervention, the individuals who will implement the intervention, the setting where those individuals work (inner setting), the wider community and regulatory context (outer setting), and the process of implementation. 37 Understanding the practice context informs the development and selection of implementation strategies and can lead to more effective implementation efforts. 38
The interview guide focused on the CFIR domains of the outer setting, inner setting, and process. Questions were related to the following CFIR constructs: Patient Needs and Resources (outer setting), Culture, Networks and Communication, Goals and Feedback, Learning Climate, Relative Priority, Tension for Change, Structural Characteristics, and Compatibility (inner setting), as well as Engaging Opinion Leaders (process). Additional questions addressed current treatments for chronic pain patients, prescription drug reliance, and demographic information about the interviewee (Supplementary Appendix SA1). The implementation team reviewed interview questions and the recruitment e-mail before sending them out to potential participants. Interviews were then conducted through online video conferences or phone calls. Snowball sampling based on interviewee responses was used to identify additional key stakeholders to be interviewed. The responses were transcribed, uploaded into ATLAS.ti Cloud, a qualitative data management software, 39 and double-coded by two experienced qualitative researchers. Both deductive codes from the CFIR codebook and inductive codes were used. Specific barriers, facilitators, and suggestions for implementation were extracted by the qualitative researchers and presented to the rest of the implementation team for discussion.
Task 2. State steps to implementation
In the second task, the implementation team reviewed the barriers and facilitators identified in task 1 and prioritized those most critical to successful implementation. All implementation team members were involved in this discussion. The team then matched barriers and facilitators identified through stakeholder interviews to steps to implementation, specifying who would need to do what to implement the IMGV into routine practice.
Task 3. Design implementation strategy components
The third task consisted of selecting and designing implementation strategies to achieve the steps to implementation and address the prioritized barriers and facilitators. The team selected two theories as most relevant to the identified barriers and facilitators: social cognitive theory and diffusion of innovations theory. 40 The authors drew on these theories to identify broad methods that target identified barriers/facilitators. For example, education can be used to target a gap in knowledge. They then drew on existing taxonomies of implementation strategies to operationalize broad methods into more specific strategies such as educational meetings and materials from the ERIC taxonomy of implementation strategies. 21
Task 4. Executing implementation strategies
In task 4, the protocols and materials needed to execute the identified implementation strategies were created through open collaboration with the implementation team and then distributed to stakeholders responsible for successful implementation. Tasks specified by the implementation strategies were delegated and executed. Evaluation of the implementation strategies occurs in task 5 of implementation mapping and includes interviews with patients and the implementation team. These activities are underway and will be reported on in future articles.
Results
The authors present results by implementation mapping task, explaining how the qualitative findings informed by the CFIR guided the process of identifying implementation strategies for IMGV.
Task 1. Identify barriers and facilitators to IMGV implementation
The authors began by identifying key stakeholders for adoption and implementation of the IMGV within the clinical setting. One of the implementation team members is a physician who agreed to lead clinical implementation of the IMGV. Based on their planning meetings, the authors determined that clinic administrators would be key actors making decisions about adoption. Clinic administrators include the clinic's Medical Director and Financial Administrator. In the qualitative analysis, CFIR codes included Key Stakeholders, Opinion Leaders, and Champions. Administrators, physicians, nursing staff, and scheduling staff were identified as key stakeholders involved in implementation.
Qualitative findings from semistructured interviews related to implementation included the following CFIR codes: Needs and Resources of Patients, Culture, Implementation Climate, Relative Priority, Networks and Communication, and Knowledge and Beliefs about the Intervention. The authors utilized these data to develop a prioritized list of barriers and facilitators to implementation, specifying the actors involved (Table 1). Barriers and facilitators focused on clinician and staff familiarity with the IMGV, including knowledge, buy-in, and operational processes needed to deliver IMGV.
Prioritized Barriers and Facilitators to Implementation
Data from qualitative interviews with key stakeholders were used to identify barriers and facilitators to IMGV implementation in the clinical site. Actors needed to address barriers and facilitators are specified, as well as stakeholders who suggested each barrier or facilitator.
IMGV, Integrative Medical Group Visit.
Knowledge or familiarity with the IMGV was noted as key to obtaining buy-in. All participants involved in direct clinical care were supportive of the purpose of the intervention and expressed that the stated goals of the IMGV aligned with their clinical goals for patients with chronic pain. Clinicians and staff expressed a lack of familiarity with details of IMGV and lack of confidence to explain the program to potential participants, noting that educational activities for clinicians and staff would be key to implementation efforts.
All stakeholders interviewed noted that leadership buy-in, from both the Medical Director and Financial Administrator, would be key to successful implementation. Other opinion leaders included the clinic's Nurse Manager and the Scheduling Staff Manager. Stakeholders noted that for IMGV implementation to be successful, clinicians would need to steadily refer patients with chronic pain to the IMGV, and this would require clinician buy-in as well.
Operational processes were also prioritized for successful implementation of IMGV. Clinicians noted that a simple electronic referral process would facilitate patient referrals to IMGV and that determining a clinical workflow would also be essential. The clinic had no prior experience running group medical visits, therefore stakeholders anticipated that new scheduling and check-in procedures would need to be determined. Finally, stakeholders emphasized the need for frequent communication and input as new procedures were being developed.
Task 2. State steps to implementation
The authors' prioritized list of barriers and facilitators was used to inform the development of steps to implementation and behavioral determinants for implementation. Steps to implementation specified outcomes needed to be achieved to address prioritized barriers and facilitators (Table 2). These include actions to be performed by both the clinical facilitator of the IMGV (in this case, a physician) and the mind–body facilitator (referred to as cofacilitators), including agreeing to implement IMGV and attend training, determining IMGV participant eligibility criteria, reviewing the IMGV manual, preparing to lead IMGV, scheduling IMGV sessions, reserving space or a telehealth platform, and communicating regularly with stakeholders. For nursing staff and other clinical stakeholders, steps included developing an understanding of IMGV and willingness to refer participants. Both scheduling staff and information technology professionals are needed to secure an electronic referral process and scheduling template for IMGV.
Steps to Implementation and Supporting Qualitative Data
Steps to implementation are specified based on qualitative data from semistructured interviews with key stakeholders.
IMGV, Integrative Medical Group Visit.
After developing steps to implementation, the authors identified behavioral determinants and change methods from the social cognitive theory 41 and the diffusion of innovations theory. 42 They identified three cognitive influences on behavior (knowledge, outcome expectations, and self-efficacy) and three change methods (cue to participate, communication, and mobilization) that could be employed to shift behavior and performance. Change targets are described in Supplementary Appendix SA2.
Task 3. Design implementation strategy components
After specifying steps to implementation, determinants, and theory-derived change methods, the implementation team identified specific implementation strategies. Because interviews were conducted during the COVID-19 pandemic, implementation strategies were designed to be conducted either in person or virtually (with some activities specified as telehealth-only). The ERIC implementation strategy taxonomy 21 was used to help identify implementation strategies and included identifying and preparing champions, participating in ongoing training, developing and distributing educational materials, and organizing clinician implementation team meetings. Implementation strategies were organized by stage of implementation, actor, determinants, and theoretical change methods. The implementation strategies are outlined in Table 3.
Integrative Medical Group Visit Implementation Strategy Plan
Stage of implementation, actors needed to execute implementation strategies, behavioral determinants, theoretical change methods, and implementation strategies are specified to create an implementation strategy plan.
IMGV, Integrative Medical Group Visit.
Task 4. Executing implementation strategies
In task 4, materials to execute the implementation strategies designed by the team were produced and the strategies were executed. The implementation team designed the language and content for educational strategies based upon language that had previously been developed for recruitment of participants for a randomized controlled trial of IMGV. Marketing and communications staff from the clinical site designed flyers to distribute to patients and staff.
Limitations
The current study assessed the feasibility of implementation mapping as a method to identify implementation strategies for IMGV in a single-site pilot study. These data are therefore limited by the single-site nature of the study and small sample size of stakeholders who were interviewed. Furthermore, implementation mapping was not compared with other methodologies for determining implementation strategies. However, given that few systematic processes for identifying implementation strategies have been developed, the current findings suggest that implementation mapping may be a feasible method for identifying implementation strategies that warrant further testing in a future fully powered trial.
Discussion
This study provides an example of the application of implementation mapping to identify theory-driven implementation strategies for IMGV. Implementation mapping offers a roadmap for how implementation frameworks, methods, and theories can be applied to the study of integrative health interventions. The authors found implementation mapping to be a feasible method for consolidating data and producing an actionable plan of implementation strategies. Those implementation strategies are currently being evaluated for feasibility and acceptability in an ongoing pilot study. Implementation mapping can be done at a single site or in a multisite trial 43 and may be a useful method for future fully powered IPM studies. By including implementation frameworks and relevant theory, implementation mapping provides a method for teams to document the rationale for choosing specific implementation strategies and to identify mechanisms of action of those implementation strategies. 22
The field of implementation science has developed many frameworks, models, and theories to make sense of the complex phenomena observed during implementation. It would be ideal to arrive at a consensus on which strategies should be used to address particular barriers, but this consensus does not yet exist in the field. Efforts are underway to synthesize and systematize the process of assessing contextual barriers and facilitators to implementation and identifying relevant implementation strategies. 44 Implementation mapping can be combined with these other tools and offers the advantage of creating a detailed description of the rationale and evidence used to choose particular implementation strategies.
While implementation research within integrative health is just emerging, the authors' findings are similar to previous studies of integrative health implementation. A large-scale evaluation of barriers and facilitators to implementation of integrative health within the Veteran's Administration noted the importance of leadership, program champions, strategic planning, and effective marketing. 45 The authors similarly found that stakeholders highlighted the importance of engaging leadership, program champions, providing clear plans to staff, and marketing effectively to ensure robust recruitment.
A review of implementation challenges and recommendations for group visits found that difficulty recruiting participants was among the most common implementation challenges and recommended the use of high-quality marketing materials. 46 The authors similarly found that recruitment was a common concern among stakeholders regarding the sustainability of IMGV within the clinical site.
Several suggestions regarding start-up procedures are described in detail in the IMGV manual for facilitators, originally developed for a randomized controlled trial. 34 While many of these procedures are specific to the execution of a clinical trial, the authors found that procedures and most language measures were directly applicable to clinical implementation of IMGV. While these components (recruitment strategies and training processes) may not be considered core intervention components, they have a strong impact on real-world effectiveness and are of principle concern to stakeholders looking to adopt evidence-based interventions.
Conclusions
Implementation mapping is a feasible method, utilizing relevant implementation theories and frameworks, to identify implementation strategies for IMGV. Implementation mapping may be useful in providing a guiding structure to employ implementation frameworks and select implementation strategies for IPM interventions. Systematic application of implementation science methods, theories, and frameworks will be increasingly important in integrative health as researchers and clinicians seek to disseminate and implement evidence-based interventions.
Footnotes
Authorship Confirmation Statement
I.J.R., J.L.B., K.R.F., S.G., K.R.K., P.G., V.E.M., and J.L. contributed to the design of the work, and I.J.R., M.K.T., and J.L.B. contributed to the acquisition and analysis of data. All authors contributed to interpretation of data. All authors contributed to drafting the work and revising it critically, gave final approval for the version to be published, and agreed to be accountable for all aspects of the work, ensuring accuracy and integrity of the work.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
The project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489. Contributions of I.J.R., J.L.B., and V.E.M. were supported by the National Center for Complementary and Integrative Health, through Grant Award Number 5T32AT00378-12. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.