
Abstract
Objective:
To conduct an interim analysis of data collected from an ongoing multisite randomized controlled trial (RCT) assessing the effectiveness of Trauma Center Trauma-Sensitive Yoga (TCTSY) for post-traumatic stress disorder (PTSD) among women veterans with PTSD related to military sexual trauma (MST). The purpose of the interim analysis was to assess outcomes from the primary site, which is geographically, demographically, culturally, and procedurally distinct from the second site.
Design:
RCT was conducted within a Veterans Administration Health Care System. Data collection included preintervention through 3 months postintervention.
Participants:
Enrollment for the main site was 152 women. The sample size for the intent-to-treat analysis was 104. The majority were African American (91.3%) with a mean age of 48.46 years.
Intervention:
The TCTSY intervention (n = 58) was conducted by TCTSY-certified yoga facilitators and consisted of 10 weekly 60-min group sessions. The control intervention, cognitive processing therapy (CPT; n = 46), consisted of 12 90-min weekly group sessions conducted per Veterans Administration protocol by clinicians in the PTSD Clinic.
Outcome measures:
The Clinician Administered PTSD Scale for DSM-5 (CAPS-5) was used to assess current PTSD diagnosis and symptom severity, including overall PTSD and four symptom clusters. The PTSD checklist for DSM-5 (PCL-5) was used to obtain self-report of PTSD symptom severity, including total score and four symptom clusters.
Results:
The findings reported here are interim results from one clinical site. For both the CAPS-5 and PCL-5, total scores and all four criterion scores decreased significantly (p < 0.01) over time in all five multilevel linear models within both TCTSY and CPT groups, without significant differences between groups. There were clinically meaningful improvements seen for both TCTSY and CPT with 51.1%–64.3% of TCTSY subjects and 43.5%–73.7% of CPT decreasing their CAPS-5 scores by 10 points or more. Effect sizes for total symptom severity were large for TCTSY (Cohen's d = 1.10–1.18) and CPT (Cohen's d = 0.90–1.40). Intervention completion was higher in TCTSY (60.3%) than in CPT (34.8%). Symptom improvement occurred earlier for TCTSY (midintervention) than for CPT (2 weeks postintervention).
Safety:
There were no unanticipated adverse events in this study.
Conclusion:
The results of this study demonstrate that TCTSY may be an effective treatment for PTSD that yields symptom improvement more quickly, has higher retention than CPT, and has a sustained effect. TCTSY may be an effective alternative to trauma-focused therapy for women veterans with PTSD related to MST.
The study is registered in
Introduction
Post-traumatic stress disorder (PTSD) affects ∼20% of veterans across populations and settings. Among women veterans, the most common cause of PTSD is military sexual trauma (MST), a pervasive problem in the military for both women and men. 1 Current first-line treatments for PTSD in the Veterans Health Administration (VHA) are trauma-focused psychotherapies, that is, prolonged exposure (PE) and cognitive processing therapy (CPT). While these therapies are evidence based, dropout rates in clinical practice and research are high 2 and more than half of those who complete treatment continue to meet the criteria for PTSD. 3,4 Women veterans with PTSD related to MST often have experienced complex trauma in addition to MST, which may be less amenable to trauma-focused therapies than PTSD related to noninterpersonal trauma. 3 Women veterans have expressed a desire for alternatives to standard PTSD treatment approaches. 5 New treatment options are needed, particularly for this population. Thus, the purpose of this study is to examine the effectiveness of Trauma Center Trauma-Sensitive Yoga (TCTSY) for PTSD among women veterans with PTSD related to MST. The purpose of this article is to present results from an interim analyses from this 5-year multisite randomized controlled trial (RCT), using complete data from the primary study site.
Women veterans and MST
MST is defined broadly by the Veterans Administration (VA) as the experience of sexual assault or repeated threatening sexual harassment during military service. 6 A recent meta-analysis reported that nearly one in four women were sexually assaulted and half of women were sexually harassed while serving in the military. 1 The VHA serves ∼ 22% of all women veterans in the United States. MST prevalence rates among women veterans who use VHA services are consistently at least 20% and as high as 49% among deployed Operation Iraq Freedom or Operation Enduring Freedom (OIF/OEF) women veterans. 7,8 These rates of sexual trauma during military service are similar to rates of lifetime sexual trauma in the general U.S. population, in which nearly one in three women (36.3%) have experienced some form of sexual violence during their lifetime. 9
Post-traumatic stress disorder
PTSD is a psychiatric disorder resulting from exposure to a traumatic or stressful event with deleterious health effects and significant distress and functional impairment. Symptoms include hyperarousal, hypervigilance, avoidance, and cognitive and mood impairment. PTSD symptoms are associated with mental and physical conditions such as depression, anxiety, chronic pain, insomnia, obesity, and cardiovascular conditions. 10 The rate of PTSD among veterans is higher than that of the general population (6.8%), 11 with a recent study reporting a rate of 23% for veterans seeking services at the VHA. 12 For both combat- and MST-related PTSD, the unique military milieu and isolation from friends and family experienced by service members contribute to higher PTSD risk and symptom severity. 13,14
Trauma-focused therapies, specifically CPT and PE, are currently recommended as first-line treatment for PTSD by the Department of Defense and the VHA. 15 A recent meta-analysis found a mean CPT effect size of 1.69 (range 1.27–2.11), with higher effect sizes among women and lower effect sizes among veterans. 16 Additionally, psychotherapy studies using wait-list controls had larger effect sizes than the studies using active control conditions. Steenkamp and colleagues reported that studies of CPT for military-related PTSD had an effect size range of 0.78–1.10, with 49%–67% of participants showing meaningful clinical change; however, roughly two-thirds of participants retained their PTSD diagnosis based on symptom severity, even after treatment. 4 In a scoping review of dropout from gold standard PTSD therapies, Najavits reported that dropout rates before completing treatment for CPT in “real world” clinical trials in civilian and military and VA settings are roughly 80%–90%, 17 rates higher than those found in RCTs with military populations (roughly 60%). 18 The implications are that the vast majority of PTSD treatment-seeking veterans and civilians are left without effective treatment. The goal of this study was to determine whether yoga could provide similar outcomes to the current gold standard, which currently consists of trauma-focused psychotherapies such as CPT. If TCTSY is as or more effective than standard treatments, it may be possible to treat more veterans with PTSD at lower costs and with greater accessibility and ease for both veterans and the VHA.
Yoga as a therapeutic intervention for PTSD
The use of yoga to treat PTSD has grown dramatically in health care settings, including the VA. 19,20 In a recent study, nearly one-fourth of VA patients responding to a survey reported using yoga in the past year. 21 However, the evidence for yoga as a clinical intervention for PTSD is inconclusive and is limited by methodological problems, for example, inadequate power, lack of randomization, and lack of control groups. 22 –24 A recent meta-analysis reported low-quality evidence for yoga yielding clinically significant improvements in PTSD symptoms; yoga had a large effect size when compared with no treatment, and a small effect size (standardized mean difference = 0.31) when compared with attention control. 25 No studies have been published comparing yoga with evidence-based treatment for PTSD. TCTSY, the experimental intervention in this RCT, was developed for civilian women survivors of complex trauma, specifically childhood sexual trauma, with chronic PTSD. 26,27 Studies of TCTSY with civilian women and veterans have effect sizes of 0.20–1.07, compared with no control, 28 wait list control, 29 and women's health education. 30
This 5-year study addresses the current gaps in knowledge of the effectiveness of yoga for PTSD and associated symptoms. The theoretical framework of the study is psychoneuroimmulogic. Yoga is theorized to have the opposite effects on the autonomic nervous system and stress response than the dysregulating effects associated with PTSD. 31,32
Study objectives
The overall study includes specific aims related to the effectiveness of TCTSY on PTSD diagnosis and symptom severity, associated symptoms, and the mechanisms of action of these effects. This article provides a report on interim analyses of the data for the primary outcomes of PTSD symptom severity and diagnosis in the main study site. Additional study enrollment (n = 49), data collection and interventions were conducted at a second site; follow-up data collection at this site will be completed in 2021. The two study sites differ geographically, demographically, culturally, and procedurally. This interim analysis of the completed sample from the first site will enable comparisons in the final analysis that will include data from the second site.
Design and Interventions
Trial design
This randomized controlled trial of the effectiveness of TCTSY for PTSD symptoms included equal allocation to the experimental condition (TCTSY) and the control condition (CPT), a current gold standard treatment for PTSD. The study is ongoing; interim findings are presented here.
Participants
Women veterans with PTSD related to MST who were users of a VAHCS were enrolled in this study. Participants were recruited primarily from the out-patient PTSD clinic and enrolled during 2016–2020. Additional recruitment was conducted in Women's Wellness Clinics and Primary Care Clinics within the VAHCS. Inclusion criteria were PTSD related to MST diagnosed in the PTSD clinic or in the first study assessment. Exclusion criteria included (1) severe psychosis; (2) current, active suicidal intent, or plan; (3) current moderate/severe alcohol/substance use disorder; (4) moderate/severe cognitive impairment; and (5) current engagement in trauma-focused treatment or yoga practice or other activity at odds with the study interventions. The study was approved by the Emory University Institutional Review Board and the appropriate VA committees.
Interventions
The TCTSY intervention was conducted by TCTSY-certified yoga facilitators and consisted of 10 weekly 60-min group sessions using the TCTSY protocol. David Emerson, the developer of TCTSY, trained the yoga facilitators and provided weekly consultation to them during the nine intervention cohorts. TCTSY focuses on interception, that is, the sense of the physiological condition of the body, in Hatha style yoga, and addresses themes related to establishing safety, individual choice, being in the present moment, and taking effective action. 27
The CPT intervention was conducted by VA clinicians (psychologists and licensed clinical social workers) certified in CPT. The CPT manualized intervention consisted of 12 weekly 90-min group sessions. 33 The sessions focused on identifying how thoughts change as a result of trauma exposure and ways in which to evaluate maladaptive thoughts and create alternative thoughts. Intervention completion was defined as attendance of at least 7 of 10 TCTSY sessions and 9 of 12 CPT sessions.
The interventions were provided in group format for nine cohorts of TCTSY and CPT groups.
Outcome meaures: PTSD
The MINI International Neuropsychiatric Interview-Version (MINI) 7.0.0 was administered to assess participants' mental health symptoms/diagnoses according to Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria and to establish a PTSD diagnosis for inclusion in the study as well as to assess for comorbid disorders. 34
The Clinician Administered PTSD Scale for DSM-5 (CAPS-5), a gold standard diagnostic instrument, was used to assess current PTSD diagnosis and symptom severity. 35,36 The CAPS-5 yields a continuous measure of overall PTSD symptom severity and the severity of the four PTSD symptom clusters: criteria B (re-experiencing), C (avoidance), D (negative alterations in cognitions and mood), and E (hyperarousal), as well as a diagnosis (yes/no) of PTSD. Symptom severity is rated on a 5-point scale (0 = absent to 4 = extreme/incapacitating), yielding a total score on 20 items of 0 to 80.
CAPS-5 interviews were conducted by trained assessors and audiorecorded; data quality was maintained via review of at least 10% of recordings by a coinvestigator and ongoing CAPS-5 supervision and consultation. CAPS-5 was assessed at baseline and at three follow-up points.
The PTSD Checklist for DSM-5 (PCL-5) is a 20-item self-report instrument that parallels diagnostic criteria for PTSD, as delineated in the DSM-5 and includes symptom cluster (Criteria B–E) subscores. 37 –39 A 5-point Likert scale is used to indicate the extent to which the respondent is bothered by each symptom (0 = not at all to 4 = extremely). Total scores range from 0 to 80 with higher scores representing greater PTSD symptom severity. The Cronbach alpha for the PCL-5 in this study was 0.870. The PCL-5 was assessed at baseline and at three follow-up points.
Data collection
Participants underwent a full assessment after enrollment to determine eligibility, and then were assessed at four time points for outcomes: (1) baseline data before the start of the intervention, (2) midtreatment, (3) 2 weeks post-treatment, and (4) 3 months post-treatment. Each study visit lasted 2–3 h and included self-report measures, interview-based assessments, psychophysiological assessment, and immunologic measures. Participants were compensated for time and travel. Only the primary outcomes of PTSD symptom severity and PTSD diagnosis are presented here.
Sample size and randomization
Of the enrolled participants (n = 152) at the main site of this multisite RCT, 104 completed baseline data collection and were randomized. One of the 104 participants had missing CAPS-5 and PCL-5 data, but is included in the sample description following intent-to-treat analysis principles. Participants within each of nine cohorts were randomized to the two groups by the block randomization algorithm “random sorting using maximum allowable percent deviation” using the PASS v.15 power analysis software package. 40 Randomization sequences were generated for each cohort, initially in blocks of 24, then in 20 based on enrollment numbers. Using the randomization sequences, the study coordinator set up sequentially numbered sealed envelopes containing randomization assignment for use at each baseline data collection. Once participants completed baseline data collection, the data collector opened the envelope to determine randomization allocation and informed the participant and study coordinator.
Initial targets for cohort enrollment were n = 20–24 (10–12 in each intervention group). However, to avoid delays in treatment and study attrition, intervention sessions were started no later than 3 months after the first enrollee for that cohort, resulting in several cohorts that were smaller than planned. Cohort sizes ranged from 6 to 16, excluding crossover participants (n = 18)—participants who opted to participate in the intervention to which they were not allocated once they completed their assigned intervention and follow-up data collection.
Given the completed sample size from the main clinical site for this interim report, the study was powered at 80% with a 5% level of significance to detect large effect sizes for group (f = 0.42), time (f = 0.49), and group-by-time (f = 0.49) effects from the longitudinal multilevel linear models (MLM). 40
Data analysis/statistical methods
Before analysis, all data were reviewed for completeness and distributional assumptions. Descriptive statistics were computed and reported for all demographics and outcome measures.
Chi-square tests were performed to compare completion rates between the two treatment groups. Multilevel linear models (MLMs) were used to compare changes over time between the two groups on the continuous outcome variables and a generalized MLM was used for the binary PTSD diagnosis outcome. For significant main effects and interaction effects, post hoc tests were performed to compare changes from baseline to the three follow-up time points: midpoint of intervention, 2 weeks post- and 3 months postintervention as well as differences between the two groups at each time point using Sidak pairwise error rate adjustment. 41 In addition, for descriptive purposes, point estimates (mean, standard deviation [SD]), 95% confidence intervals, and effect sizes (Cohen's d) were computed based on the change scores from baseline to each follow-up time point to help evaluate clinically meaningful improvements. 42 The percentage of participants who achieved a clinically meaningful change (an improvement of 10 or more points on the CAPS-5 and PCL-5 total scores) at each time point from baseline is also reported. All computations were performed using SPSS version 26.0. 43
Results
Participants were randomized to TCTSY (n = 58) and CPT (n = 46) after completion of baseline assessment of outcome measures. Randomization was conducted by cohort, yielding slightly unequal intervention group sizes over the course of nine cohorts. The age of the participants ranged from 22 to 71 years averaging 48.46 (SD 11.2) years old. The majority were African American (91.3%), were not married or in a committed relationship (71.8%), and had monthly incomes of $2000 or more (54.8%). The median years of education was 16. Table 1 presents all demographic data. Figure 1 shows participant flow through the study using a CONSORT flow diagram.
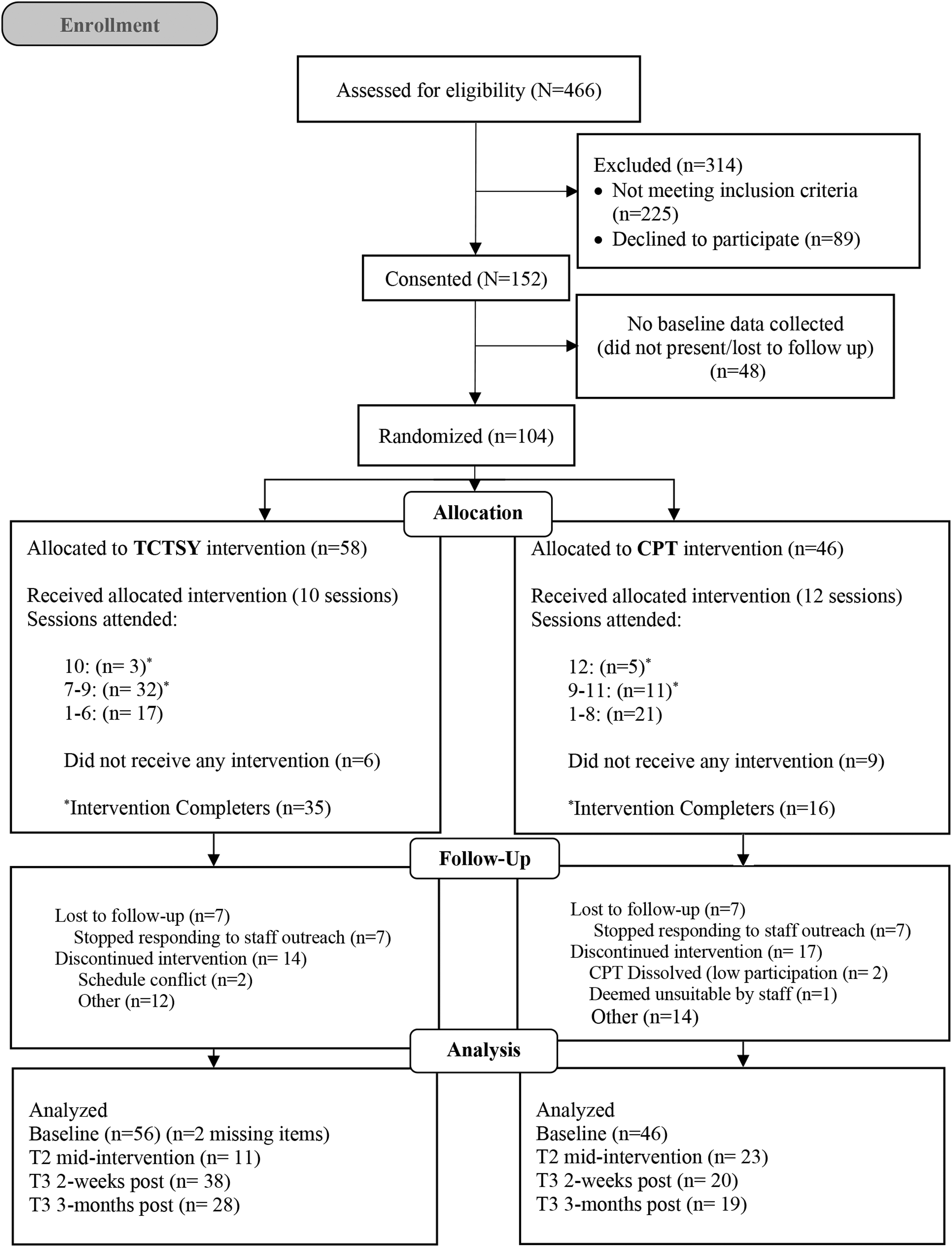
CONSORT flow diagram. CPT, cognitive processing therapy; TCTSY, Trauma Center Trauma-Sensitive Yoga.
Demographics and Baseline Characteristics
AA, African American; IQR, interquartile range; SD, standard deviation.
Intervention attendance and completion
TCTSY intervention completion was significantly higher (60.3% attended ≥7/10 sessions) than CPT (34.8% attended ≥9/12 sessions) (χ2 (1) = 6.71, p = 0.010). TCTSY session attendance dropped to about 65% after the second session and then stabilized with close to 60% or better for all the remaining sessions, while CPT session attendance persistently declined through the half-way point to 40% and lower for their remaining sessions (Fig. 2).

Percentage of participants who attended each session by group. Dashed vertical line marks the midpoint of the sessions. CPT, cognitive processing therapy; TCTSY, Trauma Center Trauma-Sensitive Yoga.
For this interim analysis of data from the main clinical site, 49 (47.1%) of the 104 participants completed the 3-month follow-up: 29 (50.0%) of the 58 TCTSY participants and 20 (43.5%) of the CPT participants.
PTSD outcomes
For both the CAPS-5 and PCL-5, total scores and all four criterion scores decreased significantly (p < 0.01) over time in all five models across both groups (CAPS-5 Table 2 and Fig. 3; PCL-5 Table 3 and Fig. 4). Both groups improved significantly and to an equal degree by the final time point. No significant group-by-time effects were found for these models, except for PCL-5 Criterion B. That is to say, there were no differences in outcomes between the two intervention groups, indicating that one treatment was not more effective than the other.
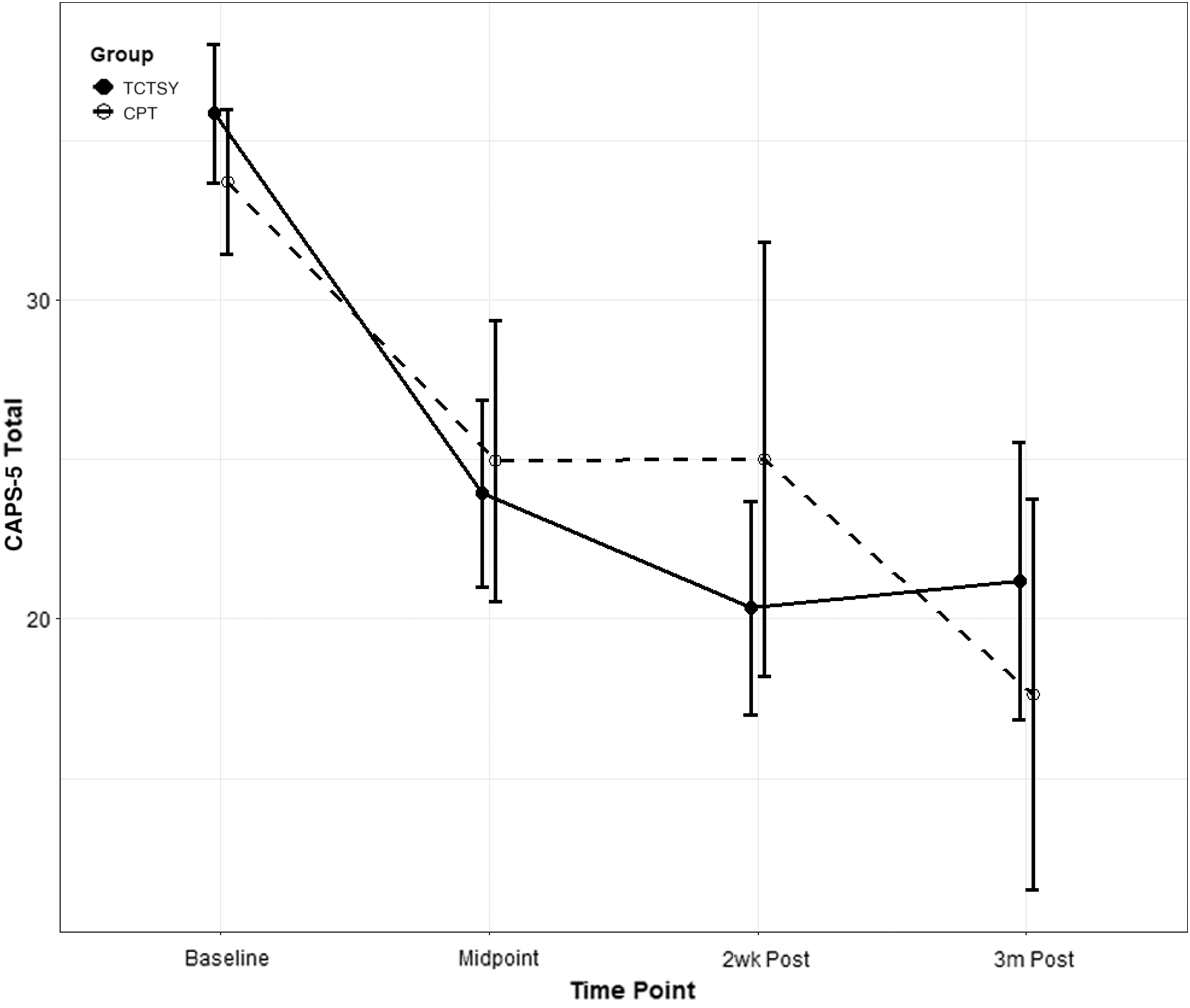
CAPS-5, total symptoms. CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CPT, cognitive processing therapy; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.
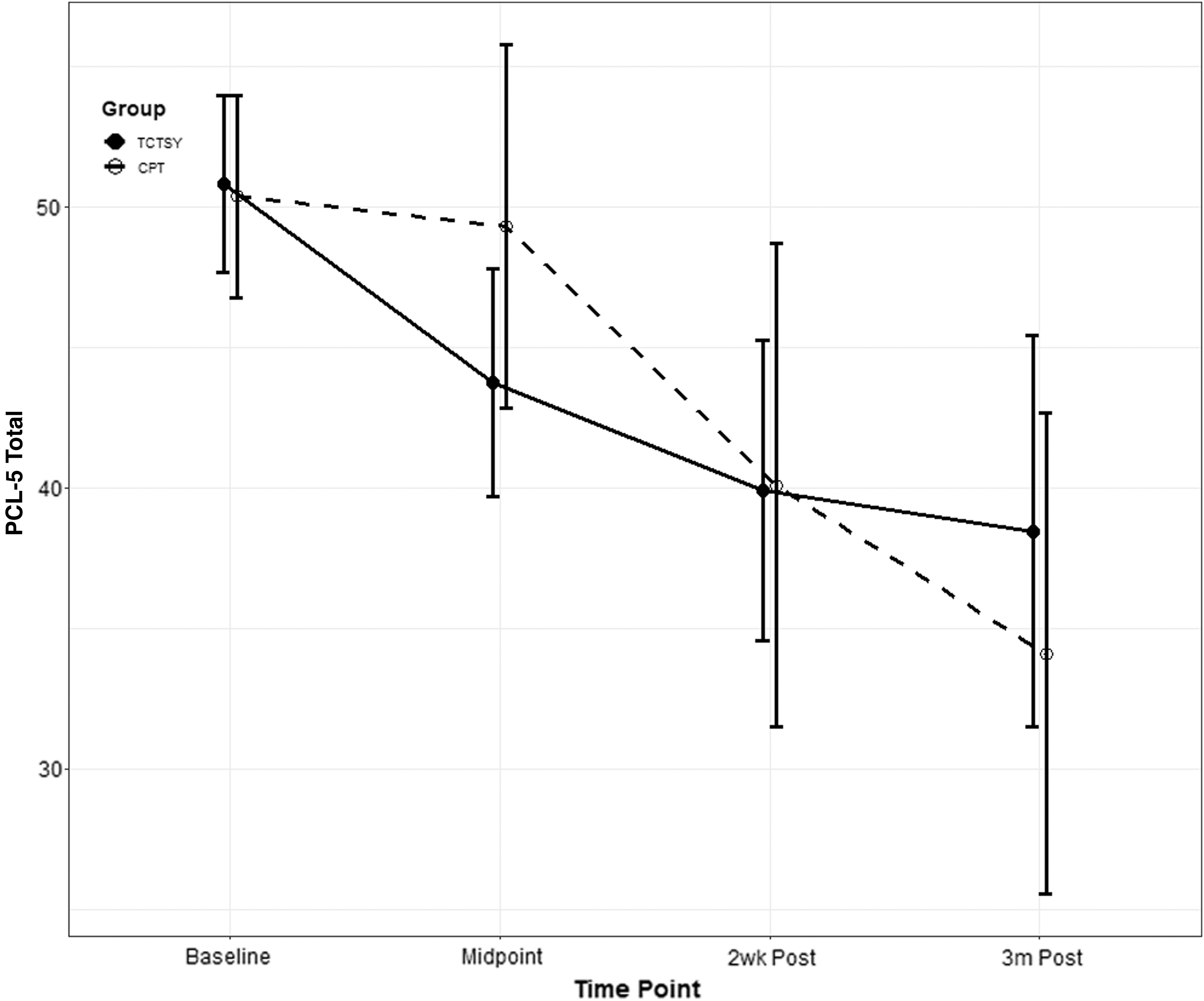
PTSD scores according to PCL-5 at the given time points according to TCTSY or CPT intervention groups. CPT, cognitive processing therapy; PCL-5, PTSD Checklist for DSM-5; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.
PTSD Checklist for DSM-5 Total and Subscales Scores Over Time by Group and Model Effects
CPT, cognitive processing therapy; CI, confidence interval; LB, lower bound; PCL-5, PTSD Checklist for DSM-5; SD, standard deviation; TCTSY, Trauma Center Trauma-Sensitive Yoga; UB, upper bound.
Clinician Administered PTSD Scale for DSM-5 Total and Subscale Scores Over Time by Group and Model Effects
CAPS-5, Clinician Administered PTSD Scale for DSM-5; CI, confidence interval; CPT, cognitive processing therapy; LB, lower bound; PTSD, post-traumatic stress disorder; SD, standard deviation; TCTSY, Trauma Center Trauma-Sensitive Yoga; UB, upper bound.
CAPS-5 clinically meaningful improvements
The trajectories of change were different for the two groups. More TCTSY participants (51.5%) showed a clinically meaningful difference (CMD, a decrease of 10 points or more) by midintervention on the CAPS-5 total score than CPT participants (43.5%). At 2 weeks postintervention, 61.1% of TCTSY participants had achieved a CMD, compared with 55.6% of the CPT group. Effects were sustained for those who completed the study. By 3 months post-treatment, 64.3% of the TCTSY and 73.7% of CPT participants achieved clinically meaningful improvements for CAPS-5 total scores. Nearly all improvements for the CAPS-5 total and four criterion scores showed moderate to large effect sizes (Table 2: most Cohen's d > 0.9, d = mean change scores divided by SD). For example, the effect size of the TCTSY group changes from baseline to midpoint for CAPS-5 total scores was 1.11 (9.98/9.03), that is large (Table 2). 42
CAPS-5 criterion scores
The reductions in CAPS-5 criteria B, D, and E scores were clinically significant and had similar trajectories in both groups (Figs. 5, 7, and 8). Of note, for CAPS-5 Criterion C (avoidance), the TCTSY group showed reductions from baseline to midintervention, with sustained effects after the midpoint to 3 months postintervention, whereas for the CPT group, there was only a noticeable reduction from baseline to 3-month postintervention (Fig. 6). For PTSD diagnosis criteria met (yes/no), both groups also showed comparable significant declines across time (p < 0.001), with different patterns (Fig. 9).

CAPS-5, Criterion B (re-experiencing symptoms). CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CPT, cognitive processing therapy; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.

CAPS-5, Criterion C (avoidance symptoms). CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CPT, cognitive processing therapy; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.

CAPS-5, Criterion D (negative alterations in cognitions and mood symptoms). CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CPT, cognitive processing therapy; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.
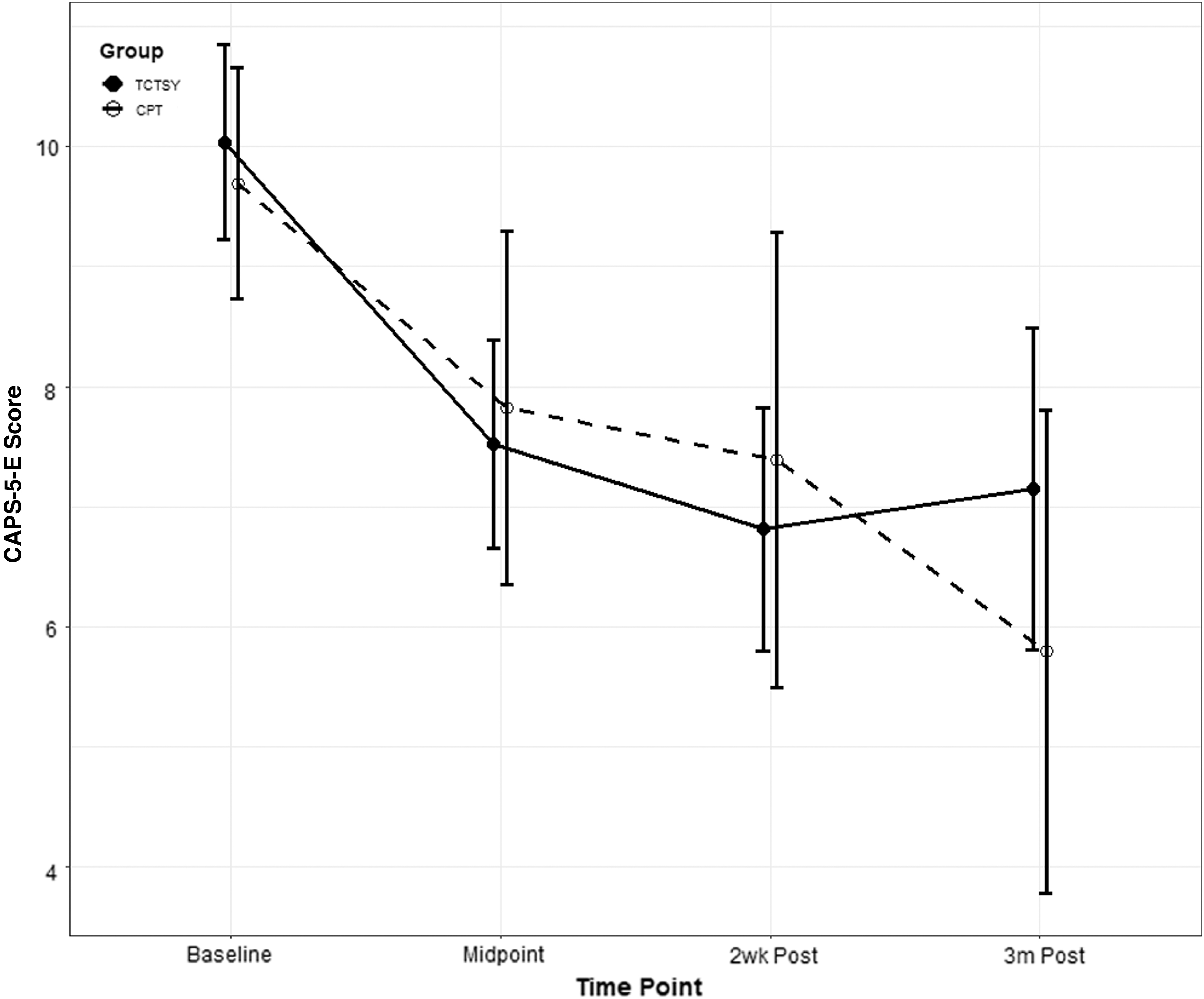
CAPS-5, Criterion E (hyperarousal symptoms). CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CPT, cognitive processing therapy; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.

CAPS-5, percent of subjects with PTSD at the given time points according to TCTSY or CPT intervention groups. CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CPT, cognitive processing therapy; PTSD, post-traumatic stress disorder; TCTSY, Trauma Center Trauma-Sensitive Yoga.
PTSD Checklist
On the PCL-5 total score, there were significant and similar reductions for both groups (p < 0.001; Table 3) from baseline to each follow-up time point. None of the tests for differences between groups were significant, indicating no significant differences between the two treatments. On the PCL-5 symptom cluster (criterion) scores, the general pattern was that the TCTSY group showed significant improvement by midintervention with sustained effects to 3 months postintervention, while the CPT group did not show significant improvement until 2 weeks postintervention, with sustained effects to 3 months postintervention. Of note, the TCTSY group showed a quicker improvement from baseline to midpoint than CPT group on the PCL-5 Criterion B score (re-experiencing; p = 0.039). However, the CPT group improved by 3 months follow-up, and there were no statistically significant differences between the two treatment groups.
PCL-5 clinically meaningful improvements
The PCL-5 total and all four criterion scores showed moderate to moderate-to-large effect sizes (most Cohen's d > 0.4, Table 3). Effects were sustained for study completers. The effect sizes for the CPT treatment group were slightly larger than for the TCTSY group. The final improvements from baseline to 3 months postintervention were larger for the CPT group. However, for the TCTSY group, the immediate improvements from baseline to midpoint were typically larger than those seen for the CPT group (most 95% confidence intervals for the change scores did not contain 0) (Table 3). For the PCL-5 total, approximately a third of the participants in both TCTSY (32.6%) and CPT (34.8%) showed a CMD (a decrease of 10 points or more) from baseline to the midpoint. By 3 months post-intervention, approximately half of the participants achieved a CMD improvement (50.0% of TCTSY and 47.4% of CPT participants).
Safety information
There were no safety problems or unanticipated adverse events reported during this study. There were no study-related physical injuries. Two participants in the CPT group withdrew due to increased psychological distress and were referred for individual therapy. The study included a Data Safety Monitoring Board (DSMB) in the final year with the addition of the second site. The DSMB met with the study Principal Investigator and had no concerns regarding safety of participants or data.
Discussion
In this interim analysis, both groups had clinically meaningful decreases in PTSD symptom severity and PTSD diagnosis. No significant differences in outcomes between the groups were found, leading us to interpret that TCTSY performed similarly to the current gold standard treatment, specifically CPT. These findings are consistent with the literature that supports yoga as an effective clinical intervention for PTSD, 25,44 as well as the literature that established CPT as an effective PTSD treatment. 4,16 The final analysis of this study should provide more definitive results. Given the design of this study as an RCT, a comparison of one intervention with another, the findings of comparable outcomes between the two groups can be interpreted to indicate that one treatment was not more effective than the other, rather than establish the effectiveness of TCTSY.
This study is the first RCT to use yoga as a comparator to a gold standard treatment for PTSD, rather than using an attention or wait list control. The use of a first-line treatment as the control condition in this RCT provides stronger and potentially more clinically relevant implications. Other studies have examined the efficacy of yoga for PTSD compared with wait list control, 45 health education, 30 wellness programs, 44 or other alternative modalities but not with evidence-based therapies. The authors wanted to compare TCTSY with the best evidence gold standard, with the goal of establishing a viable PTSD treatment alternative, given the significant limitations of the current best practices, namely engagement, retention, and initial symptom exacerbation before improvement. The finding that one treatment was not more effective than the other supports TCTSY as a viable alternative to current evidence-based psychotherapeutic treatment options, which suffer from 80% to 90% attrition and incomplete symptom resolution for many in clinical practice. 17 In this study, retention in TCTSY exceeded that of CPT by more than 25%. In addition, yoga delivered in a group setting is less costly than CPT provided in group or individual formats, the latter being more common in VA clinical settings.
This study has several strengths. First, the sample size for this interim analyses (n = 104) is larger than most yoga for PTSD studies, second only to Davis et al.'s recently published study of yoga for PTSD in veterans and civilians, in which they compared yoga with a health education control condition. 44 The predominantly African American study sample is novel in the field of yoga research in the United States and broadens the generalizability of studies of yoga for PTSD. Furthermore, the focus on MST and women with complex trauma expands the scope of yoga for PTSD among veterans beyond the more common research and clinical use of yoga for combat-related PTSD. Finally, unlike many RCTs for PTSD, the exclusion criteria were minimal; populations often excluded were included, for example, participants with suicidal ideation, comorbid serious psychiatric and medical problems, and pregnancy. 17 Furthermore, although this study was not designed as a pragmatic trial, it was conducted in a real-life clinical setting, with real-life practical considerations.
The calculation of point estimates and 95% confidence intervals for improvements from baseline along with reported clinically meaningful improvements in addition to statistical significance tests adds depth to and strengthens the evidence for TCTSY in this population. The effect sizes on the CAPS-5 total score for TCTSY (Cohen's d = 1.10–1.18) and CPT (Cohen's d = 0.90–1.40) were larger than the standard for large effects sizes (d = 0.80). Especially encouraging was the finding that more than half (51.5%) of TCTSY participants achieved clinically meaningful improvements by the midpoint of the intervention. The moderate-to-large effect sizes in the TCTSY group are double those reported in other studies of trauma-sensitive yoga (TSY) with civilians 30 and veterans. 28 The effect sizes and CMDs in this study reflect within-group improvement. Davis et al. recently reported on their large RCT of yoga for PTSD; however, while their control condition was active, it was not evidence based, and their effect size (0.46) was between yoga and a wellness intervention, rather than change within groups. 44 The selection of an evidence-based control condition to TCTSY provides a more clinically useful comparison.
The most notable differences between the TCTSY and CPT groups were timing of symptom improvement, session attendance, intervention completion, and data collection completion, all of which were higher for TCTSY. It is further noted that for TCTSY, higher percentages of participants achieved clinically meaningful improvements for their CAPS-5 total scores earlier (at the midpoint of treatment sessions) than were seen for CPT. The timing of the improvements is interesting to note. TCTSY improved symptoms significantly by the midpoint of the intervention, whereas significant improvements in the CPT group were not seen until 2 weeks postintervention. The substantially higher rate of retention and completion in the TCTSY group (60.5%) versus CPT group (34.8%) is a critical finding, as a significant limitation in CPT in the clinical setting is the relatively high dropout rate.
Study limitations
This report is limited in that it is an interim report of an ongoing study that is not yet completed. The enrolled sample (n = 152) and the intent-to-treat analytic sample (n = 104) do not reflect the final sample size. Additional limitations of this study include high attrition before randomization (n = 48; 32.6%). Half (n = 24) of this attrition was due to disparate findings on postenrollment assessment for inclusion/exclusion criteria before randomization. Other limitations include the possibility that participants may have engaged in yoga or therapy outside of the VA during the study. Finally, the CAPS-5 assessors were not blinded to group assignment due to study logistics.
Changes from clinical trials registration
There are clerical errors in the clinical trials registration that warrant clarification here. The time frame for follow-up on the outcomes is 3 months postintervention, not 3 years. The primary outcomes of interest in this study are PTSD symptoms and diagnosis, as measured by the CAPS-5 and PCL-5. As this is an interim report, only PTSD outcomes were included, as it is the main outcome of interest.
Conclusions
To the authors' knowledge, this is the first RCT comparing yoga with CPT, the latter being a trauma-focused psychotherapy and gold standard treatment, as interventions for PTSD. The results suggest that TCTSY was no better or worse than the current gold standard and, therefore, may be a viable and acceptable alternative for PTSD treatment, especially for women veterans with MST and complex trauma-related PTSD. This potential has great relevance to clinical and policy decisions, because yoga is much less costly, easier to deliver, and more feasible for veterans to access, and is scalable. These characteristics of TCTSY likely support earlier and sustained engagement in and adherence to PTSD treatment among this population of women veterans. Additional research is needed to evaluate larger scale TCTSY implementation in the VA, with the goal of establishing TCTSY as an additional first-line treatment option for women veterans with MST-related PTSD. Studies are also needed to investigate TCTSY as a treatment for men with MST-related PTSD and to investigate the effectiveness of TCTSY not only as a standalone treatment but also as a precursor and adjunctive treatment to psychotherapy for PTSD related to MST.
Footnotes
Author Contribution Statement
U.K. is the principal investigator of the study. She is responsible for the study design and oversaw implementation. She contributed to interpretation of the data and wrote portions of the article and revised the final version. T.H. contributed significantly to implementation of the study and was responsible for acquisition and interpretation of the data. She contributed significantly to drafting and revising the article. E.S. contributed significantly to data acquisition and contributed significantly to drafting and revising the article. M.H. conducted all data analysis and was responsible for drafting the ![]() section of the article. Dr. Kelly attests that coauthors have reviewed and approved of the article before submission.
section of the article. Dr. Kelly attests that coauthors have reviewed and approved of the article before submission.
Acknowledgments
The authors acknowledge the consultation and training provided by David Emerson and the dedicated interventionists in this study, TCTSY facilitators, and the VA clinicians who provided the CPT intervention. The authors also thank the women veterans who participated in this study.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the U.S. government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This material is based upon work supported by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Health Services Research and Development, Grant No. 5I01HX001087-02.