
Abstract
Introduction:
Within family medicine it is generally accepted that the more we know about patients' lives, the better the care we provide. Few studies have sought to quantify this historical assumption. We wondered if knowing their chronic pain, patients' life stories would improve the physician–patient relationship in a family medicine residency training program clinic.
Methods:
We selected patients in chronic pain with depression and/or anxiety who were considered difficult. After a lead in period to establish stability of ratings, we obtained a life story interview for 125 such patients after administering the doctor–patient relationship questionnaire to them and their physicians. Patients completed the McGill Pain Inventory (MPQ), the Zung Anxiety Inventory, and the Center for Epidemiological Studies Depression Scale. Physicians completed the Jefferson Physicians Empathy Scale. Questionnaires were repeated every 4 months.
Results:
The quality of the physician–patient relationship increased significantly over the course of the year for patients (increase of 0.60, standard deviation [SD] = 0.13, 95% confidence interval [CI] = 0.57 to 0.63, p < 0.001) and for doctors (increase of 0.77, SD = 0.20, 95% CI = 0.72 to 0.81, p < 0.001). The perceived level of pain on the MPQ decreased significantly on the sensory component (71.2 ± 7.6 to 11.7 + 9.4, 95% CI = 0.589 to 9.411, p = 0.0270 and the affective component (4.2 + 3.4 to 2.1 + 4.3, 95% CI = 0.131 to 4.069, p = 0.037). Anxiety and depression ratings did not change. Physicians' empathy ratings increased significantly over the course of the year from a mean of 117.2 (SD = 10.2) to 125.1 (SD = 16.1) for a difference of 7.90, which was significant at p = 0.0273 with a 95% CI of −14.85 to −0.915.
Discussion:
Knowing the patient's life story improves the physician–patient relationship for both patients and physicians. When the physician–patient relationship improves, the perceived level of pain decreases. Physicians' empathy ratings increase. While the interview requires 90–120 min, it is billable, and can be done by medical students, medical assistants, social workers, or behavioral health.
Conclusions:
Obtaining life stories of chronic pain patients is a cost-effective way to reduce pain while simultaneously improving the physician–patient relationship and increasing physician empathy.
Introduction
Doctor–patient relationships have been shown to matter for medical outcomes. 1,2 Within medicine, a general idea exists that the more physicians know about the lives of their patients, the better the care they provide. 3 –5 While many advocate for this concept and it seems commonsense to most primary care physicians, the idea has not been empirically studied as evidenced by searches in PubMed, OneNote, Google Scholar, and other search engines for empirical data on this topic.
The idea that knowing the patient's story is valuable has gathered traction in the training of physicians. Wong et al. 6 argue that engaging with patients through hearing the patients' stories allows students to develop knowledge about how to practice with empathy and how to better form and maintain relationships with patients in their care. Knowing the patients' stories informs their practice and their professional decision making. They say that patients' stories inspire students to think more deeply about their practice and to become more empathetic and more competent.
Martin 7 discusses the difficulties inherent in knowing the lived experience of another human being, especially one who is ill, and presents evidence that, the greater the knowledge of that lived experience, which comes through hearing the other person's stories, the better the health care will be. Computed tomography-guided periradicular therapy succeeds better when the patient feels understood by the physician. 1 Chronic pain patients feel less stigmatized by physicians with whom they have had long-term relationships. 2 To explore these ideas, we chose to focus on patients with chronic pain and comorbid anxiety and/or depression. Chronic pain is prevalent in the United States and frequently coexists with anxiety. 2 Depression is commonly experienced as comorbidity with chronic pain 8 and can impact an individual's ability to recover. 9 Since psychosocial factors have been found to be a strong predictor of outcomes, 8 there is a growing consensus that clinicians need to focus more on the importance of such psychosocial factors. 10
The presence of depression or anxiety or both is associated with how severely women rate their pain. 11 Severity of anxiety and depression is associated with more disabling and severely limiting neck and low back pain. 12 A current anxiety disorder and a comorbid depressive and anxiety disorder are strongly associated with cardiorespiratory pain. 13
In 2008, according to the Medical Expenditure Panel Survey (MEPS), about 100 million adults in the United States were affected by chronic pain, including joint pain or arthritis. Pain is costly to the nation because it requires medical treatment and complicates treatment for other ailments. Pain lowers worker productivity. Using the 2008 MEPS, Gaskin and Richardy 14 found that the total costs ranged from $560 to $635 billion in 2010 dollars. The additional health care costs due to pain ranged from $261 to $300 billion. This represents an increase in annual per person health care costs ranging from $261 to $300 compared with a base of about $4,250 for persons without pain. The value of lost productivity due to pain ranged from $299 to $335 billion. Gaskin and Richardy 14 found that the annual cost of pain was greater than the annual costs of heart disease ($309 billion), cancer ($243 billion), and diabetes ($188 billion). Their estimates were conservative because they did not include costs associated with pain for nursing home residents, children, military personnel, and incarcerated persons. Total charges associated with just low back pain hospitalizations in 2010 totaled $15,525,264,249 (adjusted in 2017 dollars). On average, charges increased significantly by ∼109% across time, from $17,340 in 2001 to $36,159 in 2010 (p < 0.001). 15
Patient-centered care is a movement toward improving the quality of medical care that patients receive from their primary care physicians. 16 Although this approach to care shows promise in giving voice to the patient and improving the physician–patient relationship through care coordination and integrated services, it leaves out the physicians' perception and personal understanding of patients' pain. Narrative medicine is an approach that can provide physicians with a better understanding of their patients' pain and suffering. 17 Illness narratives or pain narratives are stories about people's experiences with illness, pain, and disease. 18 These stories are told, not only, from the perspective of the patients diagnosed with an illness, but also from experiences of those that treat them. “By listening to such stories, and by hearing and seeing what is being told, third parties (including doctors) can grasp something of a world they might not encountered directly.”18(p.253)
Life story interviews have been used in a variety of research areas on the edges of medicine. For example, Reischer et al. 19 conducted life story interviews with middle-aged individuals, finding that highly self-transcendent individuals tended to narrate their lives as spiritual journeys of humanistic growth. Cowan et al. 20 found that life story interviews could be used to predict later depression as well as psychological wellbeing and life satisfaction. Ryborg-Joensson et al. 21 conducted a qualitative interview of older adults in Denmark with multiple comorbidities, finding that patients had learned that the details of their lives held no interest for their biomedical practitioners and so they did not share those details in their medical visits. These patients also considered the details of their lives too private and believed that sharing personal details would render them inferior to the physician. The authors described this as “discarded patient knowledge,” and showed how physician awareness of such knowledge would have changed physician understanding of the problems and provided different solutions that could have led to better health.
In this study, we aimed to assess whether conducting life story interviews and sharing this information with physicians would communicate to patients that their life stories did matter, and that knowledge of these life stories would influence the treatment process. Our study began in a family medicine residency training clinic with the recognition that our residents experienced personal distress when seeing the names of some of these chronic pain patients on their schedule. They were in a state of actively trying to avoid these people. Our goal was to determine if we could transform their personal distress into a state of empathetic concern. Keen has written, “personal distress, an aversive emotional response also characterized by apprehension of another's emotion, differs from empathy in that it focuses on the self and leads not to sympathy but to avoidance. The distinction between empathy and personal distress matters because empathy is associated with the moral emotion sympathy (also called empathic concern) and thus with prosocial or altruistic action. Empathy that leads to sympathy is by definition other-directed, whereas an over-aroused empathic response that creates personal distress (self-oriented and aversive) causes a turning away from the provocative condition of the other.”34(p.208)
This study sought to determine if knowing more about the lives of chronic pain patients would improve the quality of the physician–patient relationship and if such improvement would be associated with improvements in chronic pain, levels of depression, and levels of anxiety. We also wondered what the effects of participating in this process would have on physician empathy.
Methods
Participants
We aimed to recruit 125 family medicine patients, over the age of 18 and without a diagnosis of a neurocognitive disorder, who were diagnosed with a chronic pain condition. This was based upon a “best-estimate” effect size based upon minimal data given the lack of studies.
Eligible patients for the study were brought to the attention of the researchers by their primary care provider (PCP). The study was explained to them at the conclusion of their office visit. We told potential participants that we were seeking to determine if their PCP's knowing their life story would improve the quality of the physician–patient relationship for both parties. We were also wondering if better physician–patient relationships would be associated with improvements in pain, anxiety, and depression.
Setting
The study took place in a family medicine residency training clinic in East-Central Maine, an area that is quite rural with the common difficulties of poverty, lack of transportation, and unhealthy lifestyles. The clinic's patients were primarily the medically underserved and included patients who had been discharged from other primary care clinics due to missed appointments or noncompliance to treatment regimens or both. We began with training for the residents in narrative medicine and the importance of story. We provided training in narrative medicine and in the life story interview for medical students (primarily from the University of New England) who rotated through our clinic. We required each medical student to do one life story interview during their 4–6 weeks at the clinic.
Training
During the training and during Balint groups, we helped residents to identify which patients they considered difficult. We jointly arrived at a definition of difficult (for the residents) as meaning that the patients were not improving regardless of what the residents did, the patients were not pleasant and enjoyable in their interactions, and the residents felt stressed after seeing them. We invited the residents and the faculty physicians to refer patients who met this definition for them to the study.
Procedure
Before the life story interview, the physician and the patient completed the Doctor–Patient Relationship Assessment Questionnaire-16. Patients rated their pain using the McGill Pain Inventory (MPQ), their anxiety using the Zung Anxiety Scale, and their depression using the Center for Epidemiology Depression Rating Scale. Physicians completed the Jefferson Physicians' Empathy Scale (JPES) at the beginning and at the end of the study. All measures, except the JPES, were repeated 3–6 months after the initial measurement (at the time of the patient's next medical visit). Then we conducted a 1–2-h life story interview. Interviews were conducted by Dr. Mehl-Madrona, by medical students from the University of New England rotating through outpatient family medicine, or by family medicine residents. Participants received a token gift card worth $5 each time they interacted with the research team to show our appreciation. The project was approved by our Institutional Review Board and all participants gave informed consent. Figure 1 presents the flow chart of the study.
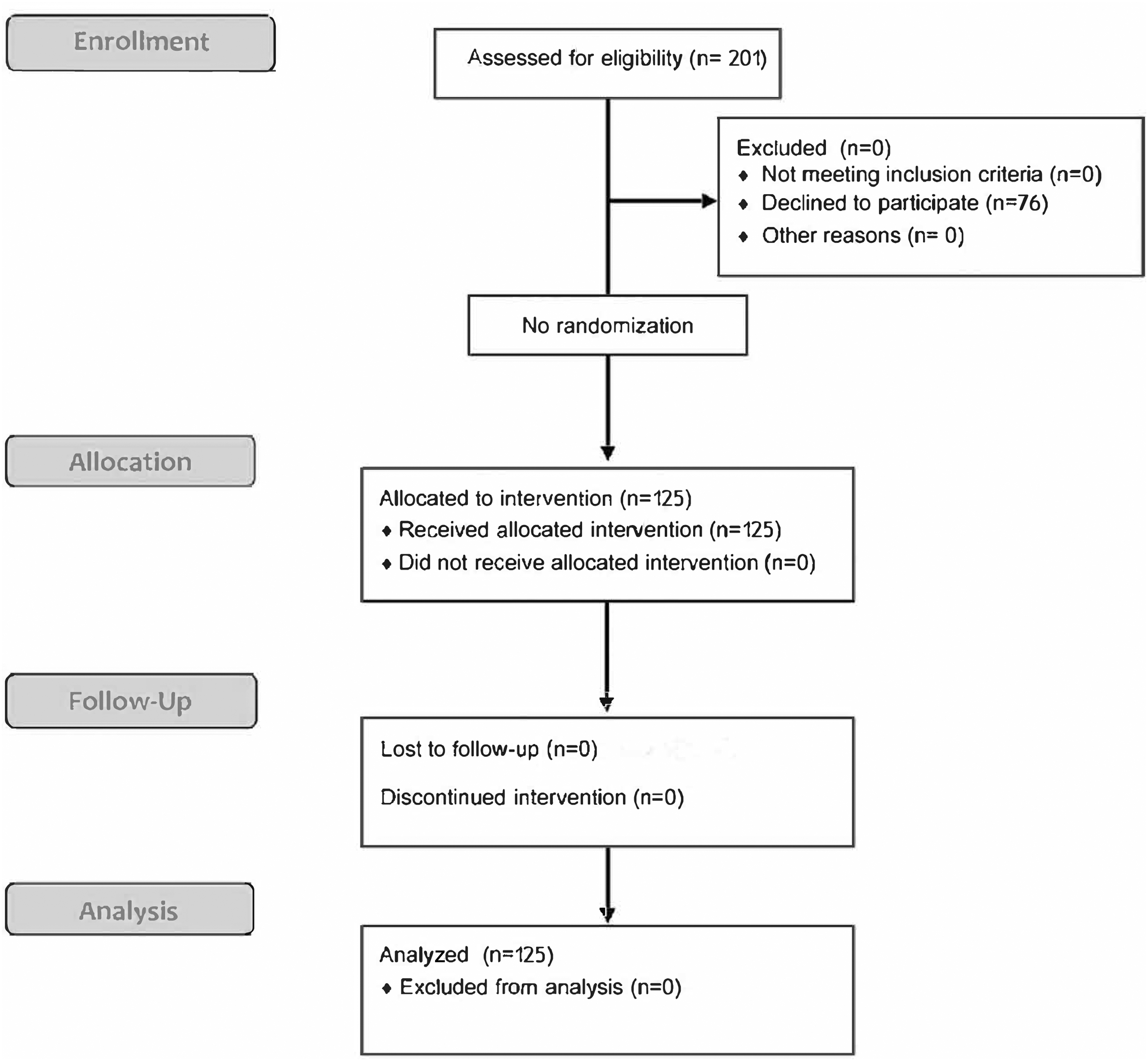
Flow chart of study.
The life story interview
The interview format is a modification of a standardized interview developed at the Northwestern University's Foley Center for Aging and is called “The Maine Life Story Interview.” It included questions about the important experiences of peoples' lives that have made them who they are today. Participants were asked to tell the stories that they wished their doctors knew about them. They were asked about high points, low points, and turning points. We worked together with participants to build a narrative about which they are happy to have their physician read. This sometimes required two meetings depending upon how much editing participants wanted to do.
We modified the Northwestern University Life Story Interview (which is public domain) by lowering the educational level of the questions and adapting the questions to a population that watches movies but does not read novels. Before obtaining informed consent, we confirmed from the medical record a legitimate diagnosis of chronic pain and of an anxiety disorder and/or a depressive disorder. All of us were proficient typists and the interview was entered into the Electronic Health Record as it progressed. Patients were given a printed copy of the interview to take home. They could make any desired changes at any time. They were encouraged to update their interview and to continue to add to it, although, to our knowledge, no one did.
When the life story was in the record, the physicians were sent a message that it was available to read. All physicians read the entire document and referred to it from time to time as they cared for the patients.
Questionnaires
The Center for Epidemiologic Depression Scale (CES-D) was used to measure the level of depression. The scoring range for the CES-D is 0–60, with 16 being the typical cutoff for declaring depression. 22 The CES-D is a self-report measure of individual's level of depression. The CES-D is a valid measure of depression in patients with chronic pain and is considered to be a valid and reliable measure of depression in medical settings. 23 The CES-D has an internal reliability of 0.85 in measuring depression. 24
The MPQ was used to assess patients' perception of pain. The scoring range for the MPQ is a minimum of 0, meaning the individual has no pain, to a maximum score of 78. 25 The higher the score on the MPQ, the greater amount of pain the individual is experiencing. The MPQ is an instrument often used in medical settings to measure a patient's level of pain. More specifically, the MPQ has been used to measure osteopathic and rheumatological diseases and was found to have strong content validity especially in its ability to detect even mild pain 26 and a good reliability score of 0.70 indicating that it is an instrument that provides a reliable and valid measure of pain in patients with chronic pain.
The Zung Anxiety Scale 27 goes from 0 to 60 and has been especially well validated in medical settings. 28 It was used to measure the level of anxiety.
The Doctor–Patient Relationship Questionnaire-16 (DoPRAQ-16) is a 16-item self-report measure of the quality of the physician–patient relationship from both the physician and patient's perspectives. The DoPRAQ-16 has an internal consistency of 0.93 and is considered to be a reliable and valid measure of the physician and patient relationship. 29
The JPES is a self-report assessment that measures physician's level of empathy. It is an instrument that has been administered in medical settings to assess both medical students and physicians' level of empathy. The scale was found to have a coefficient α of 0.89 in a study of medical students and 0.87 for residents. 30 The scale is considered to be a reliable and valid measure of empathy for both medical students and residents. The JPES is a 20-item Likert scale. 31 Scores can range from 20 to 140 with the higher score representing a greater degree of empathy. 31 It is only administered twice and not for each patient.
Patients and doctors rated their relationship again every 3–4 months for 1 year. Patients also rated their depression, anxiety, and pain every 3–4 months, also for 1 year. The doctors completed an empathy scale at the beginning of the research and at its conclusion or before their graduation from the residency, whichever came first.
Statistical analysis
We used the paired t-test procedure within SPSS for comparing mean of preintervention and postintervention ratings on the scales.
Results
Table 1 lists the demographics of this population. The distribution seemed reflective of the population of the clinic.
Demographics of the Sample
SD, standard deviation.
Two hundred one patients were approached to obtain 125 life story interviews. The main reason for declining participation was a lack of time. Before coronavirus disease 2019 (COVID-19), we were not permitted to do patient encounters through zoom, and patients had significant problems with transportation, the major one being that they had to tell their Medicaid covered transportation when they would be done at the clinic at the time of scheduling their ride to the clinic. Typically, they underestimated how long the visit would take and were running to meet their ride lest they be stranded in town. Other patients relied on family members for transportation and had to meet into their family's schedule. No patient actually refused because they thought the interview was a bad idea. All who refused did so in relation to lack of time, lack of transportation, and scheduling difficulties with their many other appointments and activities. Since the study's completion and the onset of COVID-19 restrictions, we have continued doing life story interviews and have had complete acceptance from patients who have smart phones, tablets, or computers to do the appointment through telehealth. All patients but one very much enjoyed the life story interview and expressed their appreciation for participation. The one patient who was distressed by the interview also carried a diagnosis of borderline personality disorder and was able to resolve her distress in conversation with her psychotherapist. All physicians read all interviews and expressed appreciation at having this important information. All agreed that knowing their patients' life stories made them feel more empathetic toward patients whom they had previously viewed as difficult. No physician reported that reading the life story was a waste of their time.
Table 2 shows the results for changes in the outcome measures. The patients' and the doctors scores on the DoPRAQ-16 did not change from initial measurement to baseline measurement. The patients' average physician–patient relationship rating score significantly rose from 3.80 at the time of their life story interview to 4.40 during the course of the study. The physicians' average rating of the physician–patient relationship quality rose significantly from 3.43 (at the time the patients' life story interview was obtained) to 4.20, a greater increase compared with the patients. The sensory component of the MPQ did not change between initial measurement and baseline but did change significantly from 17.2 to 11.7 over the course of the year after the life story interview. The affective component also did not change between initial measurement and baseline but did change significantly from 4.2 to 2.1 over the course of the year following the life story interview. The Pain Perception Index of the McGill did not change between initial measurement and life story interview but did change significantly from 3.7 to 2.4 over the course of the year following the life story interview. The depression and anxiety scales did not change significantly. The JPES increased significantly over the course of the study from 117.2 to 125.1.
Results for Outcome Measures
CES-D, Center for Epidemiologic Depression Scale; CI, confidence interval; NS, non-significant; PPI, Perceived Pain Index of the McGill Pain Scale; SED, standard error of difference; SEM, standard error of mean; VAS, Visual Analogue Scale of the McGill Pain Scale.
All patients statistically significantly reduced consumption of opiates, benzodiazepines, and sedative hypnotics.
Discussion
This study represents an effort to explore how exposure to longer stories about patients' lives can improve the quality of the physician–patient relationship, thereby potentially reducing patients' level of pain and increasing physician empathy. The quality of the physician–patient relationship and patients' pain ratings did not change during our “run-in period” consisting of 3–6 months before the life story interview. Following the life story interview, significant improvements occurred in the quality of the physician–patient relationship, the level of perceived pain of patients, and in the physicians' empathy scores. Knowing more about patients' lives appears to improve the physician–patient relationship and is associated with reductions in patients' perception of pain.
Our study is limited by lack of a control group and randomization. The use of a lead-in period to show that the measures were not changing over 3–6 months is helpful, but not the same as having a parallel control group, a study we are now conducting. We are also conducting focus groups with the patients and the residents to explore their beliefs about how participating in the project changed things for them.
Our study was helpful in showing that knowing patients' life stories was associated with measurable changes and in calculating effect sizes of those changes to aid in designing a randomized, controlled trial. The study is also encouraging in suggesting that the physician–patient relationship is an important tool in managing chronic pain and that improving that relationship may be a reasonable intervention for treating chronic pain. Importantly, we learned that the reasons for patient refusal were logistical and, thanks to the changes occurring in medicine from the COVID-19 pandemic, modified our life story interviewing to a telehealth approach, in which all patients asked, have now agreed to participate. It was also helpful to see that all the physicians enthusiastically read the life stories and that 124 of 125 patients stated that the interview was a positive experience.
While all patients reduced consumption of controlled substances, we did not further analyze these data, since we believe it was confounded by changes in Maine's laws and licensing regulations toward the prescription of controlled substances over this same period. The prescribing of opiates became dramatically more regulated, restricted, and surveyed with the implementation of a prescription-monitoring system, requirements that acute opiate prescriptions be for 1 week or less, requirements that no patients receive more than 90 mg of morphine equivalents per day (except those in hospice), and a general discouragement by the licensing boards for prescribing any opiates for chronic pain. Therefore, we could not legitimately argue that knowing the life story reduced opiate prescribing given the presence of these other factors.
Narrative medicine ideas in conjunction with the concepts of patient-centered care are emerging around the world and are changing physicians' attitudes toward patients and the process of primary care. Research remains to be done on how to best introduce these ideas to physicians and to understand how well they will be received. We have chosen to focus on one population whom physicians consistently rate as challenging—people with anxiety and/or depression who have chronic pain. The goal of this study was to investigate the impact that reading their patients' life stories and stories about their pain would have on the quality of the physician–patient relationship as measured from both perspectives. We asked also if improvement in the quality of the physician–patient relationship will improve patients' quality of life and physicians' empathy.
Merely hearing a description of the actions of a person who is absent activates mirror neuron areas during functional magnetic resonance imaging of the human brain. 32 Although the effects are strongest in real life, face-to-face interactions, they still operate when we read stories about other people 33 as in the current study. People scoring high on empathy scales show high activity in their mirror neuron systems. 33 Keen writes about the efforts of contemporary virtue ethicists, political philosophers, educators, theologians, librarians, and other interested parties to connect the experience of empathy with outcomes of changed attitudes, improved motives, and better care and justice. 34 In this study, we have shown that reading difficult patients' life stories improves the physician–patient relationship and is associated with reduced levels of perceived pain. Participating in this study was associated with increased empathy levels at the end of 1 year among the physicians.
Egnew states that our approach to patients with pain should take into account the personal understanding of the patient's experience of pain. 35 Hearing their subjective experiences of pain in their own words contributes toward making meaning of the pain. Egnew writes that the power of the physician–patient relationship assists people to reduce their pain and suffering. Through listening to patient's stories, physicians gain a better understanding of their patients' pain and suffering as well as enter their patients' world and join their patients in making meaning out of their pain. 36
The importance of the physician and patient relationship in the healing process is recognized as having a vital impact on physicians themselves, and especially so for physicians who treat patients with chronic pain. 37 Patients diagnosed with chronic pain can pose challenges that include both relational and communication difficulties. Providers have described the importance of an effective physician–patient relationship in the treatment of chronic pain that they often felt pressured to prescribe opiates, and finally that they felt frustrated in caring for some patients with chronic pain. 37 There is also a necessity to increase physicians' capacity for patient-centered communication skills that includes empathy for patients with chronic pain and shared decision making between physician and patient. 37
Recognizing the importance of physician empathy, DasGupta and Charon utilized reflective writing as a tool to increase the empathy of 2nd year medical students. 38 They had medical students write and share with their colleagues their own personal illness narratives. The study recognized that physicians who experience physical illness themselves have a greater understanding of the pain and suffering experienced by their patients. It is this understanding of personal pain that places physicians in a unique position to work with patients experiencing chronic pain. It is personal illness narratives that can help to create a better understanding between the patient and doctors, 39 as well as empathy and a sharing of responsibility for ongoing care. 37
Kenny examined the interactions between physicians and patients who were suffering from chronic pain and found that many of the interactions between physician–patient undermine recovery and, in fact, were distressing for both parties. 40 Implications of Kenny's research include the need to identify and better understand problematic relationships that can develop between physician and patient.
Narrative medicine is a medical model that is informed by both patient-centered and biopsychosocial models of medicine. 17 It is a practice that bridges understanding and the complex connection of the physician–patient relationship.17(p.1897) According to Charon, a physician who practices with narrative competence is one that practices with empathy. Narrative knowledge deals with the interactions between two people. 17 A physician with narrative knowledge or competency is one who not only has empathy for his or her patient, but also has the potential to bridge the gap between physician and colleagues, the public, while also creating a space to appropriately advocate on a patient's behalf. 17
Included in the connection between patient and physician is what Charon 17 calls empathic engagement. According to Charon, empathic engagement is a process of listening to patients' stories of illness, while also understanding the patients' difficult journey. It is a way of witnessing and joining with the patient in his or her pain and through that joining with the patient being able to effectively care for their patient. 41 A physician that is not able to achieve empathic engagement with a patient means that the patient may not feel heard or understood. In the end, this means that physicians may order tests that are not necessary, may make an inaccurate diagnosis, and encounter a patient that is noncompliant with recommended care. 42
Without understanding the patient's story and without empathic engagement, patients with chronic low back pain and depression may continue to suffer in isolation and physicians continue to feel frustrated without real solutions to fix the patient's pain. Walker et al. utilized a narrative approach to gain further understanding of the lived experiences of twenty back pain patients who were seeking treatment from pain clinics in the United Kingdom. 43 A major theme that emerged was focused on how the system that was supposed to support and rehabilitate the patients, actually made them feel more powerless. They emphasized that narrative accounts of patients who seek treatment for chronic pain may help clinicians have a better understanding where negative attitudes stem from and how this impacts patients' ability to get better.
Kim writes about the potential for therapeutic relationships to be transformative. 44 Here is where the physician can shine and outperform nurses working with artificial intelligence systems. Through building a therapeutic relationship, physicians can become agents of transformation. Those relationships begin with story, with knowing the patient's life story beyond the elements necessary for billing Medicare.
Conclusions
Knowing the patient's life story, improved the quality of the physician–patient relationship for the physician. After telling their life story, patients reported higher levels of quality of their relationship with their physician. Telling their life story to a medical student significantly reduced patients' perception of pain, which persisted over 1 year. It did not change their perceived levels of anxiety or depression.
General agreement exists that increasing physician empathy is a good idea and multiple interventions have been designed to do this, 45 including using simulated patients 46 and communication skills training programs. 47 Empathy is considered central to patient-centered medicine. Higher levels of physician empathy are associated with greater levels of patient satisfaction and enablement. Despite this, empathy in clinical encounters is often lacking and empathy in medical students decreases as they progress through their training. 46
Footnotes
Acknowledgments
The authors acknowledge and appreciate the medical students and residents who did some of the life story interviews described in this article.
Author Disclosure Statement
The authors have nothing to disclose and have no conflicts of interest.
Funding Information
This work was supported in part by Coyote Institute, Orono, Maine.