
Abstract

Introduction
This article describes a historically significant, but previously unpublished, small study from 2006 that explored the acceptability, feasibility, and preliminary effectiveness of a meditative yoga practice. The significance was a function of both who the subjects were, and the context of the trial.
At the time of this study, leaders of the Walter Reed Army Medical Center (WRAMC) had an interest and an identified need to explore the feasibility and acceptability of complementary and integrative health (CIH) offerings as optional therapies for military service members. A chief interest was in symptoms of post-traumatic stress disorder (PTSD). This study, a specialized outpatient program at WRAMC, offered a yoga treatment for active duty military service members with PTSD. Although not formally engaged or reported as a feasibility study, the internal understanding at WRAMC was that positive outcomes could potentially influence additional implementation of yoga offerings for military members with PTSD.
Methods
A single cohort of seven active duty military members who scored a minimum of 40 on the PTSD checklist (PCL) participated in this 9-week study at the WRAMC in Washington, DC. The intervention included 18 group classes and prerecorded iRest yoga nidra practices for home use. The iRest program teaches skills for self-regulation and healthy interoception to help manage moods, memories, emotions, and physical sensations with conscious option-driven choices rather than unconscious reactivity. Because this form of yoga practice requires no physical effort, the practice can be safe even if the body is recovering from injury. Participants were instructed to listen to the home practice on days the class did not meet. Outcome measures included PTSD symptomatology (PCL) and depression [patient health questionnaire (PHQ)]. IRB approval: FWA#00001628, USU IRB Reference G188JO. Clinical Trials#: NCT00269490.
Results
Class attendance rate was 67% and overall home practice adherence was 42%, with a study attrition rate of 14%. Only one person dropped out of the study. The other participants maintained attendance except for explained absences such as medical appointments or scheduled leave. For these participants, the PCL appeared to demonstrate a clinically meaningful improvement in PTSD symptoms: three of these active duty military members had over a 10 point change (25, 22, and 15 point change) and two had a reliable change of over 5 points (7 and 9 point change) (Fig. 1). The PHQ showed a general trend toward decreasing depressive symptoms with a reliable change of over 5 points in three of the participants (7, 15, and 15 point change).
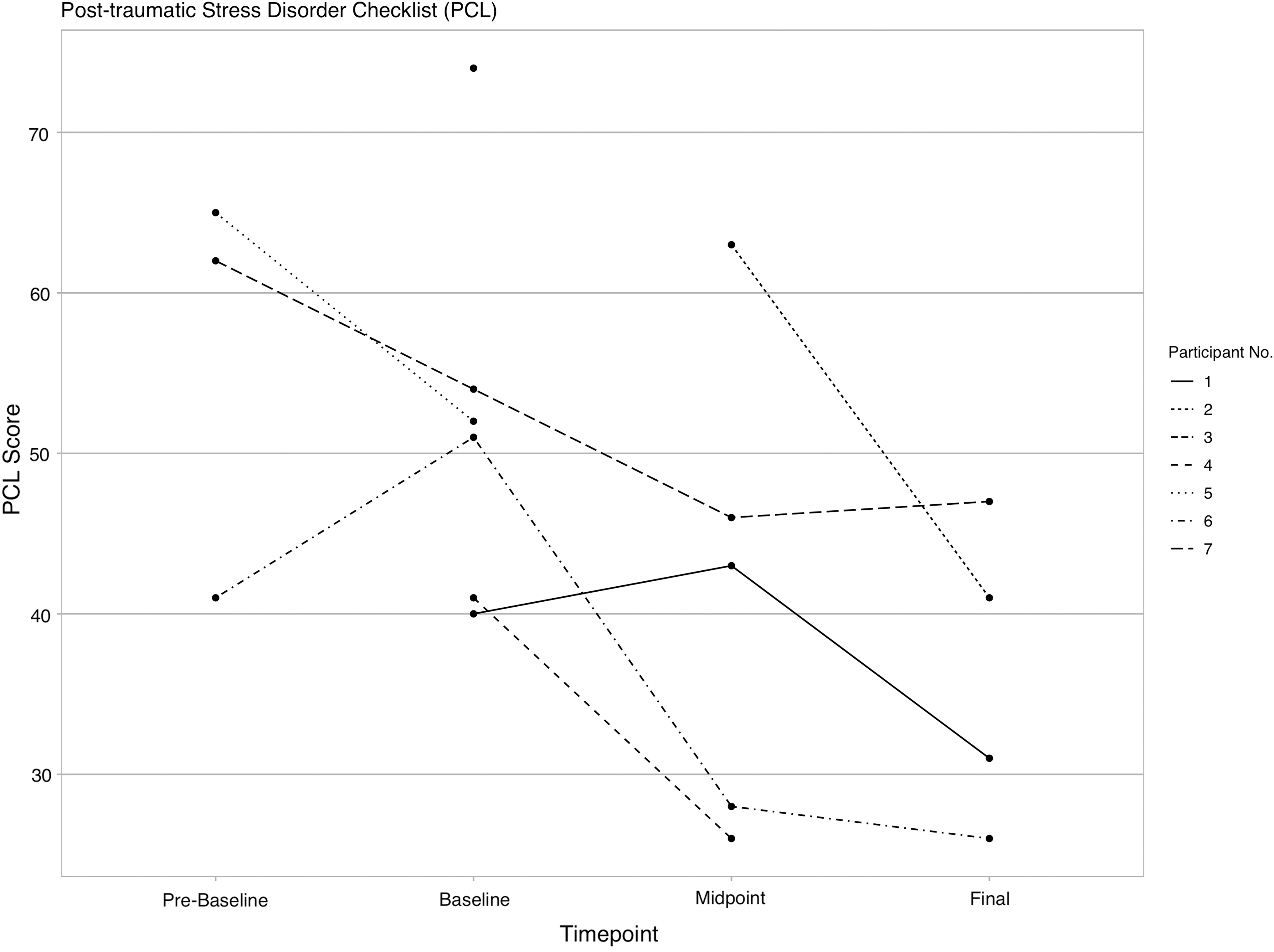
PCL: there was a general trend toward decreasing PTSD symptomatology. PCL, PTSD checklist; PTSD, post-traumatic stress disorder.
Limitations
The study had significant limitations, including the small size and lack of controls. Another limitation was the challenge of recruiting a single cohort as those recruited early on often dropped out due to assignment to other military installations or loss of interest waiting for the program to begin. The sample size was insufficient for inferential analysis and the data for some participants was not collected at all time points when they missed classes.
Conclusion
This small study indicated that a meditative yoga program appeared to be acceptable and potentially beneficial for active duty military service members with PTSD. It suggested that yoga nidra could be a promising CIH intervention for the active duty military and veteran populations.
Historic role
Although this study was never published, due in part to disruptions in employment and funding at the sponsoring organization, its impact proved to be significant. With the apparent acceptance of yoga nidra by military personnel, and with a known availability of instructors, the findings led to immediate implementation into the deployment health clinical center at WRAMC. WRAMC proved to be the first to launch this program, which is now, 14 years later, in over 50 Veterans Administration Hospitals and Military Installations across the United States for various mental and physical health conditions. 1 –3 In the War Related Illness and Injury Study Center in Washington, DC, this program has been offered since 2007 where studies have shown high satisfaction for helping with physical and mental health symptoms. 4,5 In addition, iRest yoga nidra has been recognized as a Tier I approach for addressing pain management in military care. 6
Footnotes
Acknowledgments
The authors of this report also acknowledge the work that went into the previous unpublished articles and study, including Damara Cockfield, MPA, Matthew Fritts, MPH, Joan Walter, JD, Nathalie Gerassimov, BS, Robin Carnes, MBA, Michael C. Freed, PhD, Kristie Gore, PhD, Charles Engel, MD, MPH, Wayne Jonas, MD, and Alison Whitehead, MPH.
Author Disclosure Statement
Richard Miller is the founder of iRest Institute. Stephanie Lopez is Senior Director of Teachings and Programs and Marlysa Sullivan is Head of Research for iRest Institute. There are no competing financial interests for this work.
Funding Information
This study was sponsored and funded by the Department of Defense, MILCAM2003 contract # MDA905-03-C-0003 with the Uniformed Services University of the Health Sciences.