
Abstract
Introduction:
Oral mucositis (OM) is the most prevalent side effect in patients with head and neck cancer (HNC). It causes an obvious decrease in quality of life (QoL) in these patients, so different medications have been recommended for OM, however, without optimal response. This randomized trial aimed to assess the effects of a honey–lemon spray compared with benzydamine hydrochloride in prevention of radiation-induced OM in patients with HNC.
Materials and Methods:
Forty-six patients with HNC received external beam radiotherapy for 5 days per week. Patients were randomized to treatment with either benzydamine hydrochloride spray or honey–lemon spray for 5 weeks and continued for 1 week after the end of treatment. The oral cavity was examined weekly, with a score given to each site based on the degree of mucositis using a 4-point scale, and a mean mucositis score was calculated as the primary outcome. Occurrence of OM, pain, QoL, and adverse effects were defined as secondary outcomes. Patients, therapists, and outcome assessors were blinded to group allocation.
Results:
No significant group differences occurred in the mucositis score, pain, or QoL. Mucositis occurrence rates were higher in the benzydamine hydrochloride group compared with the honey–lemon group (hazard ratio = 2.1, 95% confidence interval: 1.1 to 4.2). Two patients in the honey–lemon group had mild nausea and burning throat; no adverse effects occurred in the benzydamine hydrochloride group.
Conclusions:
There were no significant group differences in mucositis severity between patients treated with honey–lemon spray and benzydamine hydrochloride. The potential preventive effects of honey–lemon spray need to be confirmed in further trials.
The trial registration number is IRCT20161024030467N1.
Introduction
Head and neck cancer (HNC) accounted for ∼8% of new cancer diagnoses in 2018. Nearly 83% of HNC patients need radiotherapy and at least 60% of them will suffer from oral mucositis (OM)—the most prevalent side effect of radiotherapy in this patient group. 1,2 OM is defined as ulcerative lesions of the oral mucosa and it has become a challenging issue in the quality of life (QoL) of HNC patients. 2 Unfortunately, the pathophysiology of the disease is not clear enough. 3 Potential side effects of OM include severe pain, the increased risk of systemic and local infections, a disorder in the mouth and throat function, and mouth bleeding, which influence the daily activities of the patient such as eating, sleeping, and speaking and generally affect the patient's QoL. This may cause treatment interruption and deterioration in treatment results due to prolongation of the radiotherapy course. 4 Some patients need to be hospitalized longer, which also increases the treatment expenses. 5
In Persian medicine (PM) and other traditional health systems such as Ayurveda and Traditional Chinese Medicine, honey has been recommended to treat sores, 6,7 especially mouth sores, and recent studies have also indicated the effectiveness of honey in prevention and treatment of mucositis and mouth sores in HNC patients. 8 –10 In PM, honey is believed to have a hot temperament and to make the mouth dry. 11,12 Recent studies suggest that eating sweet foods worsens dryness in the mouth and they recommend that patients avoid them. 13 To overcome this issue, it was recommended to mix honey with lemon because in PM and other traditional systems, lemon is believed to have wet temperament. 14,15 Moreover, based on recent studies, lemon in different forms, such as lemon pastilles, lemon slices, and vitamin C tablets, 13 has been recommended for decreasing dryness in the mouth due to its sour stimulatory mechanism. 16
Many treatment methods have been suggested for preventing radiation-induced OM. However, efforts made to prevent OM during and after the radiotherapy are not satisfactory. In fact, there is no approved prophylaxis for OM 13 and mostly supportive treatments are recommended to patients, including decrease in pain, a healthy nutrition, and improving patient's saliva condition. 17 In a study that was conducted during the period 2005–2006 in Iran's Cancer Institute and some other trials, it was shown that benzydamine hydrochloride mouthwash had a significant effect in preventing OM in HNC patients. 18 –20 In addition, in the studies by Epstein et al. and Roopashri et al., benzydamine hydrochloride significantly decreased erythema and mouth sores, increased the intervals of the appearance of sores, and delayed the use of pain killers. 18,21 Since recent studies have emphasized the role of benzydamine hydrochloride in prevention and decrease of OM after radiotherapy, 22 this study aimed to examine the effects of honey–lemon spray compared with benzydamine hydrochloride in prevention of radiation-induced OM in HNC patients.
Materials and Methods
Trial design
This study was a pilot, double-blind clinical trial using an active control group, which was conducted between September 2019 and February 2020. Patients who referred to the cancer clinics of Jorjani and Shohaday-e Tajrish in Tehran, Iran, were potentially eligible. The methodology of the study did not change after the study was started.
Study protocol
HNC patients who required radiotherapy based on physician discretion entered the study if they fulfilled the inclusion criteria. According to the study inclusion criteria, patients who were between 18 and 80 years of age, who had enough mental and physical ability to cooperate, and who had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2 were eligible. At least 2 areas of 10 head and neck mucosal areas (lower and upper lips, right and left buccal mucosa, dorsal and ventral part of the tongue, floor of the mouth, oropharynx, and soft and hard palate) needed to be included in the treatment volume. At each weekly visit, a 4-point scale was used to score these areas at risk, and then the overall mean mucositis score was calculated. Signing the informed consent was mandatory. Patients who had used alcohol or medications affecting salivary gland function (such as antidepressants, opioids, antihypertensives, antihistamines, diuretics, any type of mouthwash, artificial saliva products, and cigarettes) during the study; had candidiasis or any oral lesions; had a history of receiving chemotherapy or radiotherapy to the head and neck area or using other mouthwash products during the study; had a liver or kidney failure; and were suffering from connective tissue diseases such as Sjogren disease, arthritis rheumatoid, and lupus erythematosus were excluded. Those who had a history of allergy to herbal medicine, had a positive pregnancy test, and those who had mental diseases and were taking medications for their mental disease were also excluded. Patients were randomly divided into two groups; the first group received the honey–lemon spray (intervention group) and the other group received the benzydamine hydrochloride spray (control group). An oncologist referred the patients to the researcher and the demographic information forms were also filled by the researcher. A head and shoulder thermoplastic mask was used for fixation of the patient's head and neck during radiotherapy. Computed tomography simulation was done for all patients and after defining target volumes, a treatment plan using three-dimensional conformal radiotherapy or intensity-modulated radiation therapy techniques was created. After plan approval, areas at risk that were within treatment volume for at least 50 Gy were defined in the evaluation form by a radiation oncologist to be evaluated by a researcher during treatment. All the patients were treated with 2 Gy per day for 5 days a week. Both groups of patients were evaluated before the treatment, including oral cavity examination, measurement of each patient's weight, and filling out the primary forms. In addition, the amount of radiation received, size of the field, area treated, designed final dosage, and required days of radiotherapy were written down. Examining the oral cavity and oropharynx to check the occurrence, or progress, of mucositis and oral pain was done every week until 1 week after the radiotherapy by the researcher. OM and pain were marked based on the defined scale. Sprays were given to patients for free and the patients were asked to start using them 1 day before starting the radiotherapy for 5 weeks or until they were excluded from the study for any reason. The spray had to be used four to eight times per day. Compliance was defined as use of at least 80% of the drug by the end of the treatment period. The sprays were collected at the end of the study to calculate how much is remaining. In cases of lack of compliance, the patients were excluded from the study. General recommendations for oral hygiene during radiotherapy were described to patients of both groups.
Drug preparation
For preparing the drug, honey and lemon juice were purchased from the Mahyar Company (Tehran, Iran) and Golchekan company (Mashhad, Iran), respectively. Honey and lemon juice were mixed in the ratio of 2:1 at room temperature, then filtered out to become completely flat. The liquid was then filled in 30-mL spray bottles. The prepared spray was standardized based on citric acid content.
For the control group, 120-mL benzydamine hydrochloride mouthwash solutions were purchased from the Behvazan Company and the liquid was filled in exactly the same spray bottles used for the intervention group. The labels for both sprays were the same. Then, all the spray bottles were coded by a research assistant who did not participate in the study.
Study outcomes
The primary outcome was defined as the mean mucositis score in radiation-induced OM. Occurrence of OM, pain, QoL, and adverse effects were defined as secondary outcomes.
Data gathering and tools
At the beginning of the study, all participants willingly signed the consent form before enrollment in the study. Before the intervention, the demographic information form (age, gender, marital status, and education level, etc.) was filled for each participant. The patients were visited weekly and mucositis in the risk area was graded based on the World Health Organization (WHO) mucositis grading scale. 23 In addition, at the beginning of the study and 1 week after the end of the intervention (sixth week), the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire, Head and Neck Module (EORTC QLQ-H & N 35), was filled by each participant. The validity and reliability of the questionnaire have been proved in previous studies. 24 Inspection of the mouth for examining the mucositis and grading it were performed as described before 25 (Table 1) and done by the same researcher before the study and after each week of receiving radiation (at least 5 weeks). This is a Persian version of the scale used by Silverman et al., 26 and the authors calculated Cronbach's α of 0.75 and correlation coefficient of 0.83 for that trial. Based on the treatment plan, the authors defined at-risk areas for each patient. These were areas receiving cumulative radiation doses of more than 50 Gy. A score was given every week to each area at risk by an oncologist, and then the overall mean score was counted based on scores gained from at-risk areas only. In addition, the visual analog scale (VAS) form for pain was checkmarked by the patient at the beginning of the study and at the end of each week during the study. Another form was given to patients to record the side effects experienced such as systemic or topical reactions during the intervention.
Oral Mucositis Scoring System
Sample size
Considering the study power as 80%, with 0.05 type I error, an expected difference of 40% in the mean of the OM score (based on the pilot analysis on 10 patients and the resulting outcome), and a dropout rate of up to 25%, the sample size was defined as 23 for each group.
Randomization and blinding
Randomization of patients was done by the research assistant using the Randomizer software and simple randomization method with an allocation ratio of 1:1. After providing written informed consent, each patient was given a code by a research assistant who was not involved in eligibility assessment or including patients in the study. The drug was also given to the patients by the research assistant and the code of the drug given to each patient was recorded. The allocation was decoded at the end of the study by the research assistant. In cases of life-threatening side effects, the allocation was immediately decoded by the research assistant and the patient was excluded from the study.
Patients, therapists, and outcome assessors were blinded to group allocation (CONSORT-2010-Checklist).
Data analysis
At the end of the study, data cleansing and preparation were done on the collected data. All data were analyzed on the basis of intention-to-treat sample analysis. For comparing the frequency and the mean score of OM between groups before and after the study, the mixed-effects zero-inflated Poisson regression was used. For comparing the amount of pain based on the VAS, the ANCOVA was used. The QoL score (generally and separately according to each of seven dimensions) was calculated based on the SF-36 scoring scale. The average score of QoL before and 1 week after the end of the intervention was calculated. Using the paired sample t-test or Wilcoxon signed-rank test, the average QoL scores of the intervention and control groups were compared. The effect sizes of tests were calculated using the Cohen-d formula.
Kaplan–Meier survival analysis was used to compare the risk of OM occurrence between groups. The hazard ratio (HR) with 95% confidence interval (CI) was calculated.
The data were analyzed with the Statistical Package for the Social Sciences (SPSS, Inc., Chicago, IL) software, version 21. Statistical significance was defined as <0.05.
Ethical issues
The trial complied with the Declaration of Helsinki and the relevant local research ethics committees. This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (
Results
The average age of participants in the intervention and control groups was 53.2 ± 14.8 and 52.9 ± 18.2, respectively (p = 0.957). The ratio of male to female participants in intervention and control groups was 10/13 and 17/6, respectively (p = 0.071). In the intervention and control groups, 11 and 8 patients, respectively, had nasopharyngeal carcinoma, and the primary sites of cancer in the intervention and control groups were the tongue (5 and 2 patients), larynx (1 and 4 patients), salivary glands (2 and 1 patients), oral cavity (3 and 4 patients), and unknown (1 and 4 patients), respectively (p = 0.323). The flowchart of patients' recruitment is shown in Figure 1.
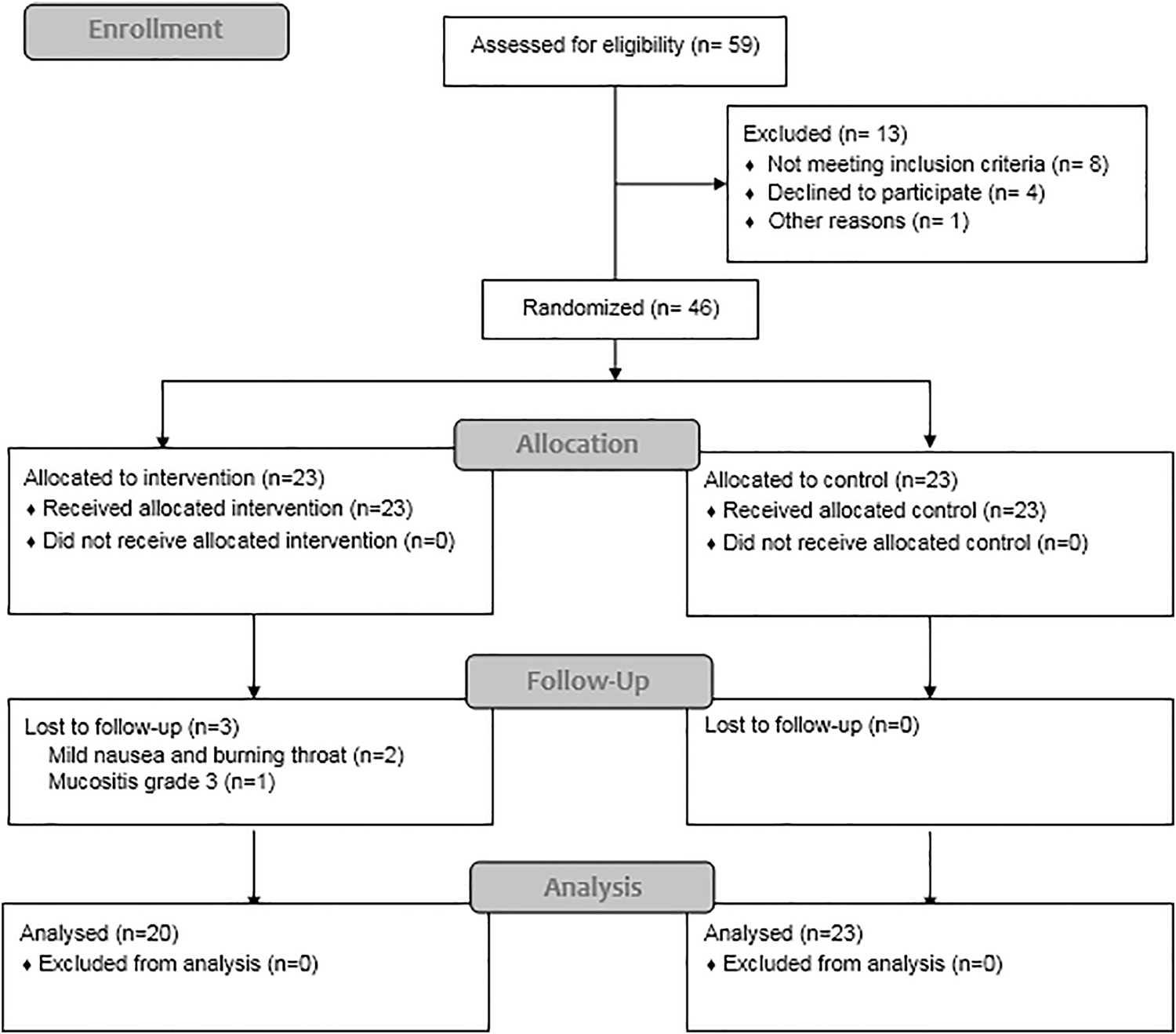
CONSORT flow diagram.
Figure 2 shows the trend of changes in mucositis scores on inspection, and Figure 3 shows the trend of changes in the amount of pain declared. As is evident in Figure 3, the reported pain scores in both groups do not show a statistical significance.
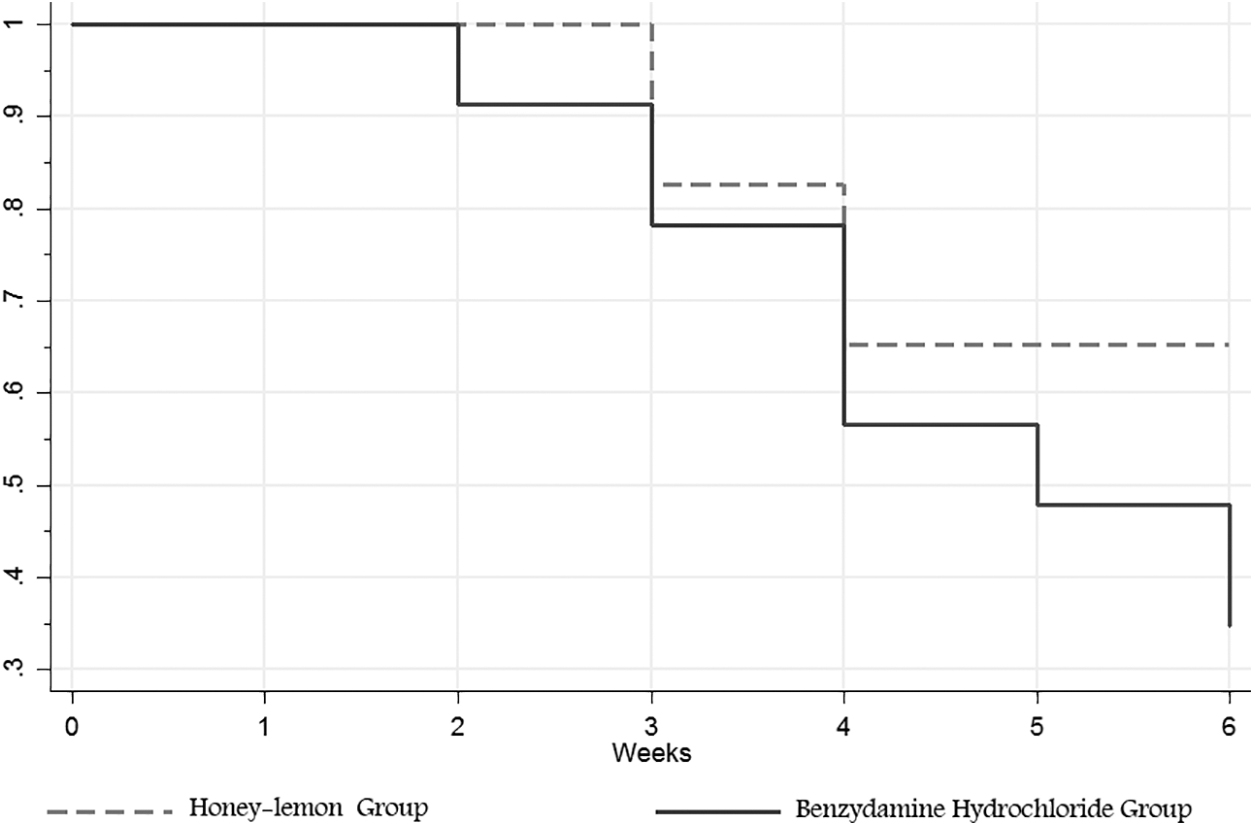
The trend of changes in mucositis frequency and mean scores based on physician's examination.
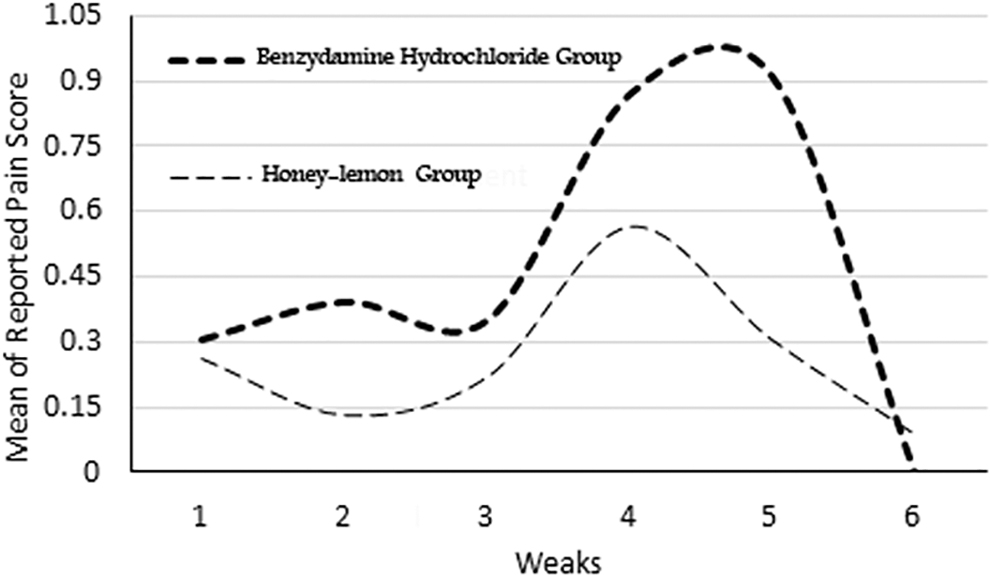
The trend of changes in the amount of pain reported by patients based on visual analog scores.
The physician's inspection and self-declaration by participants about their amount of pain based on the VAS indicator did not show a significant difference in the frequency and mucositis score of OM (p = 0.051) and the amount of pain (p = 0.28) during the 5-week treatment in both groups.
At the end of the trial, the occurrence of OM was observed 1 week earlier in the control group. On the other hand, 35% of patients in the control group did not have OM compared with 65% in the intervention group (Fig. 2). The risk of occurrence of OM during this study was twice as high in the control group compared with the intervention group (HR = 2.1, 95% CI: 1.1 to 4.2). Regarding the grade of OM occurring in patients during the study, 10 patients had grade 3 mucositis in the intervention group against 14 in the control group (p = 0.292).
As can be seen in Table 2, the QoL of both groups before and 1 week after the end of the intervention in seven dimensions of pain, swallowing, emotions, speaking, eating, social relationships, and dryness of the mouth was examined. There were no significant group differences in any of the seven dimensions.
The Quality of Life of Intervention and Control Groups Before and 1 Week After the End of the Intervention in Seven Dimensions
Based on Cohen's d.
CI, confidence interval.
Examining the side effects of the honey–lemon spray, two patients were found to have mild nausea and burning throat and were excluded from the intervention group. However, no side effect was reported in the control group.
Discussion
The results of the current study on 46 HNC patients indicated that the benzydamine hydrochloride spray and honey–lemon spray had similar effects with regard to the mean score of radiation-induced OM based on the physician's inspection and patients' self-declaration before and at the end of the 5-week treatment. This was also true about the amount of pain that patients experienced based on the VAS indicator. The QoL of patients in both groups was evaluated before and 1 week after the end of the intervention and the results did not show any significant difference in the seven aforementioned dimensions, which denotes that the benzydamine hydrochloride drug and the suggested PM drug had comparable effects on the patients. The risk of OM occurrence was lower in patients using the honey–lemon spray compared with those using the benzydamine hydrochloride spray.
Different studies examined the effectiveness of herbal medicine and natural products (in different forms such as syrup, mouthwash, and decoction) on prevention and treatment of chemotherapy/radiation-induced OM. 8 However, as far as the researchers know, the current study is the first clinical trial comparing the effects of the honey–lemon spray and benzydamine hydrochloride. Khanal et al. indicated protective effects of honey (oral and topical) against radiation-induced OM in their randomized clinical trial. 27 The same effect along with the antibacterial effect of honey was shown in a study conducted by Rashad et al. on 40 HNC patients who had chemotherapy and radiotherapy treatments simultaneously. 9 In the study by Motallebnejad et al. in 2008, it was demonstrated that using oral and topical honey had a significant influence on decreasing OM severity compared with the standard treatment. 28 In their study on 40 patients, Biswal et al. indicated that the group using oral and topical honey had a significant decrease in their grade 3/4 radiation-induced OM compared with the standard treatment. 10 In two other studies, ineffectiveness of Manuka honey in decreasing the frequency and severity of chemo/radiation-induced OM was observed and this is while both of the studies recorded low compliance of patients. 29,30 Most of the aforementioned studies demonstrated a significant influence of honey on radiation-induced OM. However, the tested spray in this study combined honey and lemon biochemicals, which may have synergistic effects on the mentioned properties. In addition, the honey used in this study did not originate from the Manuka plant, which is native to New Zealand, and this can justify the differences between the current study and the studies by Hawley et al. and Bardy et al. 29,30
The benzydamine hydrochloride spray has been examined as a known treatment for radiation-induced OM in recent studies and Rastogi et al. also recommended it for high doses of radiotherapy in 2017. 31 In 2 double-blind clinical trials on 151 head and neck cancer patients who were receiving radiotherapy, Sheibani et al. and Kazemian et al. demonstrated that benzydamine hydrochloride had a significant prevention effect in decreasing the frequency and severity of radiation-induced OM compared with the placebo group. 20,25 These findings along with newer ones, which have shown the effectiveness of benzydamine hydrochloride, 22,32 and the nonsignificant differences between the groups in the current study hint at a potential use of the honey–lemon natural product as a promising agent for decreasing radiation-induced OM in HNC patients. This needs to be confirmed in future studies.
The potential mechanism of action for the honey–lemon spray could be related to the anti-inflammatory, antioxidant, antibacterial, and wound healing effects of honey, which have been demonstrated in prior studies. 33 Decreases in inflammation factors, such as the C-reactive protein and erythrocyte sedimentation rate, and antibacterial and anticancer effects of lemon have also been reported. 34,35 These are mechanisms that are in line with some studies and show that herbal medicine or natural products can prevent or treat OM.
According to the literature, in evidenced-based medicine, factors such as effectiveness, public acceptance, safety, and cost-effectiveness of the suggested treatment should be taken into account. 36 Based on findings of the current study and the potential similarity of results in the considered indexes, the favorability of natural products and traditional medicine, and the examination of cost-effectiveness of the drugs (considering the relatively low cost of the suggested product), it is necessary to precisely examine this PM product as a possible alternative drug in the treatment of OM.
In spite of using valid measures in the study, the lack of an objective outcome measure was one of the limitations. However, it should also be noted that performing biopsies in the patients is also not ethical. The limited sample size, borderline imbalanced distribution of patients by gender in both groups, inability to mask the taste of honey or lemon for patients, and lack of long-term follow-up for patients are some other limitations of the study that might have influenced the results. Prescription of the honey–lemon spray with different dosages is another factor that should be taken into consideration in future studies.
Conclusions
Natural products and herbal medicine have a long history in the treatment of cancer and radiation-induced side effects. The effectiveness of some natural products has been shown in different studies. However, it seems vital to conduct high-quality clinical trials with a large sample size, which focus on the comparison of the suggested drug and standard drugs such as benzydamine hydrochloride. The similarity of effects of the honey–lemon spray and benzydamine hydrochloride on the frequency, mean score of OM, and QoL of HNC patients could lead to introduction of a natural product as an economical and more available alternative drug if more precise clinical trials are conducted on the suggested PM drug in the near future.
Footnotes
Authors' Contributions
G.H., A.A., R.C., and M.P. were involved in conceptualization. G.H., A.A., and M.P. performed the methodology. G.H., A.A., H.C., S.P., H.H., S.A., and M.P. performed the data curation. A.A. and M.P. performed the formal analysis. G.H., S.P., and R.C. performed the investigations. G.H., A.A., H.C., H.H., S.A., and M.P. wrote the original draft. A.A., H.C., R.C., and M.P. performed the writing review and editing. G.H. and A.A. performed the supervision. All authors have read and approved the final manuscript.
Acknowledgments
The authors would like to express their gratitude to the patients who trusted the research team and participated in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
CONSORT-2010-Checklist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.