
Abstract
Objectives:
Plantar heel pain (PHP) is the most common cause of heel pain and can be debilitating; 20% of patients are refractory to standard of care. The Fascial Distortion Model (FDM), a novel manual diagnostic and treatment strategy, is purported to be effective for chronic pain; however, no rigorous studies document its effectiveness. We assessed the FDM for care of PHP.
Design:
Single arm prospective effectiveness study.
Settings/Location:
Outpatient primary care clinic; Fort Gordon, GA.
Subjects:
Outpatient adults.
Interventions:
Participants received an FDM-informed diagnostic and treatment strategy to identify fascial “distortions” at the foot based on patient-reported pain patterns and palpatory examination and then to provide distortion-specific manual therapy at baseline and 1 week.
Outcome Measures:
Primary outcome measure (0, 1, and 16 weeks): the Foot Pain subscale on the validated Foot Health Status Questionnaire (FHSQ; 0–100 points on each of eight separate subscales); secondary outcome measures (0, 1, and 16 weeks): the seven remaining subscales on the FHSQ, visual analog pain scale (VAS, 0–100 points), and plantar fascia thickness of the most effected foot assessed by ultrasound (0 and 16 weeks). Analysis was performed per protocol using repeated-measures analysis of variance.
Results:
One hundred and ninety-seven participants were screened; 33 were enrolled. Twenty-eight participants received two FDM procedures. Compared with baseline, improvement on the FHSQ Foot Pain (33.8–23.6 points) and Foot Function (23.9–19.8 points) subscales and VAS (44.7–27.7 points) at 16 weeks was statistically significant (all p's < 0.001) and clinically important representing large effect sizes. Relative to baseline, 16-week ultrasound demonstrated reduced average plantar fascia thickness (0.6–0.9 mm [p = 0.001]). Demographic characteristics were unrelated to response. Satisfaction was high. There were no serious adverse events; side effects included consistent mild-to-moderate self-limited pain.
Conclusions:
Participants with PHP who received FDM-informed care reported significant and sustained improvement on validated foot pain and foot function measures; additional findings included decreased plantar fascial thickness. These results require corroboration in a larger randomized controlled study. Clinical Trial Registration No: DDEAMC17005.
Introduction
Plantar heel pain (PHP; plantar fasciopathy; ICD-10 plantar fascia fibromatosis) is the most common cause of heel pain and can be debilitating, resulting in ∼1 million outpatient visits per year in the United States. 1 PHP has a lifetime incidence of 10% in the general population, and ∼85% of the time, the etiology is cryptogenic. 1,2
The proximal cause of pain is complex and incompletely understood. Local inflammation due to overuse is understood to contribute to pain, but some studies report degenerative changes without inflammation consistent with other overuse soft tissue injuries. 3,4 In the absence of clear etiology, standard of care for PHP is multidisciplinary and includes several conventional and complementary therapies, including physical therapy, osteopathic manipulation, dry needling, injections (corticosteroid, blood products, prolotherapy), acupuncture, shoe inserts, nighttime splints, medication, shockwave therapy, radiofrequency ablation, and surgery. 5,6 Management varies and is clinician-dependent. 1,2 Approximately 20% of patients are refractory to routine care. 3,7
The role of fascia in musculoskeletal health and disease has received recent attention, and it is understood to be a pain-generating tissue. 8 How it is involved in chronic pain is not well understood; focal entrapment neuropathy in which a nerve is prevented from gliding within its fascial sheath is a potential contributor. 8,9 A diagnostic and treatment perspective known as the Fascial Distortion Model (FDM) was developed in 1991. 9 Proponents posit that musculoskeletal injuries are often the result of one or more of six specific alterations to fascia (“distortions”) and that specific manipulative techniques can restore altered fascia to a preinjury, anatomically “normal” state. 9,10 The FDM has been reported to be promising for several chronic conditions, including back pain, 11,12 adhesive capsulitis, 13 medial tibial stress syndrome, 14 chronic hamstring tightness, 15 shoulder pain, 16 and ankle sprains, 17 although rigorous studies including mechanistic and clinical trials are lacking.
Therefore, the authors prospectively assessed the FDM for diagnosis and treatment of PHP to test the hypothesis that participants would report decreased foot pain, improved foot function, and demonstrate normalized plantar fascial thickness on ultrasound assessment.
Methods
This single-arm prospective effectiveness study was approved by the Dwight D. Eisenhower Army Medical Center human subjects Institutional Review Board. Participants were recruited from the Dwight D. Eisenhower Army Medical Center from April 2018 to February 2019.
Inclusion criteria were being active duty military service members between the ages of 18–65 years with self-reported heel pain for 30 or more days and clinical diagnosis of PHP. Potentially eligible participants were identified using the Tricare beneficiary database, from which the billing codes for plantar fascial fibromatosis (M72.2) were screened from the previous 6 months. Patients were contacted by phone to be informed about the study and determine interest and eligibility.
Exclusion criteria included a history of aneurysm, bleeding disorders, active cancer, phlebitis, thromboembolism, foot site contraindications (infection, open wound, hematoma, or edema), planned military deployment within the 16 weeks postscreening, medical condition that would preclude study participation, and pain that would interfere with foot pain reporting.
Each foot was assessed separately; both feet were treated if both met eligibility criteria. Interested, eligible persons attended an informational meeting, provided written informed consented, completed baseline questionnaires and ultrasound examination, and underwent intervention.
Outcome measures
The primary outcome measure was the Foot Pain subscale of the Foot Health Status Questionnaire (FHSQ), a validated disease-specific quality-of-life questionnaire composed of 19 items in 8 subscales each ranging from 0 to 100, with higher scores denoting more favorable health status. 18 The remaining seven subscales of Foot Function, Shoe, General Foot Health, General Health, Physical Activity, Social Capacity, and Vigor were part of the secondary outcome measures. The FHSQ has a goodness-of-fit index of 0.9 and a comparative fit index of 0.96, suggesting high validity. 19 The minimal clinical important difference (MCID) criteria has been established for the Foot Pain (14 points), Foot Function (7 points), and General Foot Health (9 points). 19,20 The FHSQ was administered at baseline and then again at 1 and 16 weeks.
Other secondary outcomes included heel pain, plantar fascia thickness as measured by ultrasound, pain medication utilization, and duty limitations. Heel pain was assessed via a 100-mm visual analog pain scale (VAS); participants addressed the statement “Foot pain from plantar fasciitis: Mark the scale from zero (not at all severe) to 100 (extremely severe)” at 0, 1, and 16 weeks. VAS assessment is frequently used in pain assessment; the American College of Rheumatology identified a clinically important improvement in pain on the 100 mm VAS for the following conditions to be: 11 points for degenerative joint disease and musculoskeletal conditions, 28 points for postoperative pain, and 30 points for neuropathy, chronic low-back pain, and fibromyalgia. 21 Ultrasound-assessed plantar fascia thickness of the most affected foot was measured at 0 and 16 weeks. The thickness is the standard objective assessment for PHP. 22,23 Reduction in plantar fascia thickness is believed to be a reliable and accurate method of monitoring improvement following therapeutic interventions at the plantar fascia; however, the precise clinical relationship and statistical correlation between abnormal plantar thickness and PHP is not well known. 23 Plantar fascia thickness was measured with the Sonosite Edge ultrasound machine using an Edge II linear probe (HFL38xi 13-6 MHz). Images were obtained in the supine position and measured from the anterior edge of the inferior calcaneal border vertically to the inferior border of the plantar fascia per published guidelines. 23,24 Normal plantar thickness is less than 4 mm. 22,23 Images were obtained and read by one physician sonographer (Robert Kirtley, MD) credentialed by the Eisenhower Army Medical Center and overread by an musculoskeletal fellowship-trained radiologist (Mickey Chabak, see the Acknowledgments section). Readers were blinded to the patients' pre- and post-treatment status.
Pain medication was assessed at baseline, week 1, and week 16. Participants were queried regarding pain medication use in terms of “No change, decreased, or stopped” compared with the prior visit. Participants reported military duty limitations due to PHP at baseline, week 1, and week 16 by disclosing if they had a documented Department of the Army Form 3349, or “Physical Profile,” the framework used by medical and behavioral health providers to indicate a soldier's functional limitations. These profiles indicate how a medical condition limits their capacity to perform physical activity and their specific duties as a soldier. Demographics, duration of PHP, and prior therapies used were collected at baseline to characterize the sample. Side effects including procedural pain (mild, moderate, and severe) and adverse events were assessed postprocedure. Participants were discouraged from starting new therapies for PHP during the study period.
Procedures
At baseline, study participants were consented and enrolled; provided demographics and medical and military physical training profile histories; completed assessment questionnaires; and underwent physical ultrasound examinations and were treated. The FDM-trained treating physician (J.B.) assessed all participants at baseline and 1 week. Using physical examination and manual manipulation skills informed by the FDM, he identified and treated locations of presumed fascial distortion about the plantar area of the foot; “distortions” could include any of the six reported fascial anomalies in the FDM: continuum distortions, trigger bands, herniated trigger points, folding distortions, cylinder distortions, and tectonic fixations (Fig. 1). In this study, the following four distortions were identified; each was treated. Each is diagnosed using a combination of symptoms and signs detectable to an FDM-trained clinician. Herniated trigger points are suspected when the patient describes pain while pushing into soft tissue with a thumb or finger and the clinician detects a characteristic palpable tissue texture change over that area. 9,25 A continuum distortion is identified when the patient identifies pain using a single finger pressing on a bony prominence. 9,25 A trigger band is suggested by pain in a longitudinal pattern. 9,25 A folding distortion is suggested by pain within a joint often described by a patient's cupped hand. 9,25 Each distortion is associated with a recommended reparative manipulation. Briefly, with significant force, the tip of the clinician's thumb is pushed along the trigger band, into the herniated trigger point, or over the continuum distortion for 3–5 sec. 9,25 Treatment of folding distortions is more complex and consists of pushing or pulling the joint with medium velocity and low amplitude in a nonpainful plane. 9,25 The purported mechanism of action is that these distortion-specific manipulations restore normal fascial structure, although objective evaluation has not confirmed this hypothesis. 25
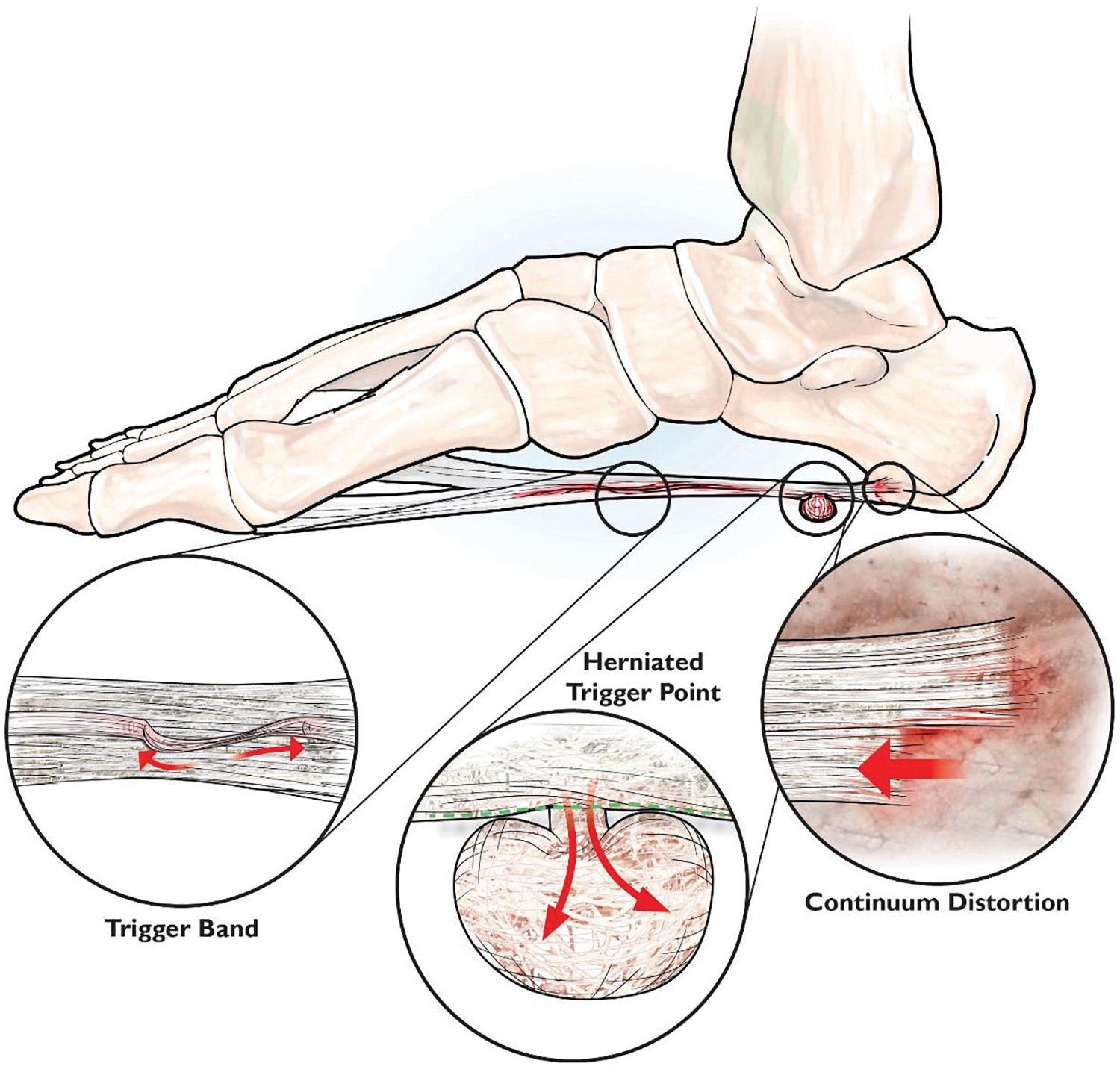
Illustration of three fascial distortions detected in the current study. Used with permission from illustrator Julie Coats. Color images are available online.
Analysis
A per-protocol analytic approach using SPSS 26.0 statistical package was employed to investigate whether manipulation using the FDM for PHP improved outcomes. Descriptive statistics were performed to describe outcomes at each time point; average value ± standard deviation (SD) was reported at baseline unless otherwise specified.
Repeated-measures analysis of variance (ANOVA) tested the hypothesis that there was a within-subject omnibus improvement over time in FHSQ and VAS scores. Statistical assumptions including sphericity were met. Post hoc within-subject paired sample t-tests were used to identify at which time points a statistically significant difference in FHSQ and VAS scores occurred (i.e., at 1 or 16 weeks later relative to baseline). Average values ± SD are reported for these analyses. The unit of analysis for both was the participant. Partial eta squared (ηp 2 ) was calculated by SPSS and reported to appreciate effect size. Within this context, small, medium, and large effect size values for ηp 2 reflect: 0.01, 0.06, and ≥0.14, respectively.
The unit of analysis for plantar fascia thickness was the most affected foot, regardless of whether one or both feet were treated. A paired sample t-test compared differences in the thickness of study plantar fascia at 16 weeks postintervention relative to baseline. One study participant did not undergo ultrasound at 16-week postintervention. The missing data point was resolved by imputation of 16-week ultrasound average.
A conventional p-value of ≤0.05 was selected to denote statistical significance. A priori sample size calculation was performed using G*Power 3.1. For the PHP subjects being measured across three observations with an alpha at 0.05, power set at 0.8, and assuming a large effect size, the study sample needed a minimum of 23 cases to be adequately powered to detect statistically significant change.
Results
Thirty-three participants were recruited. Five participants were excluded from per-protocol analysis after enrollment due to receipt of a corticosteroid heel injection (n = 2), detection of calcaneal fracture on procedural ultrasound (n = 1) and lower extremity deep vein thrombosis (n = 1) unrelated to therapy, and direct treatment by physical therapy (n = 1). There were no significant differences between those who completed the protocol and those who were excluded in terms of demographics, military rank, time in service, Medical Evaluation Board (MEB), or physical training profile status, majority of PHP treatment-related experiences, baseline outcome assessment, or types of fascial distortions encountered (Table 1). Therefore, 28 participants were included in the analysis (Fig. 2).
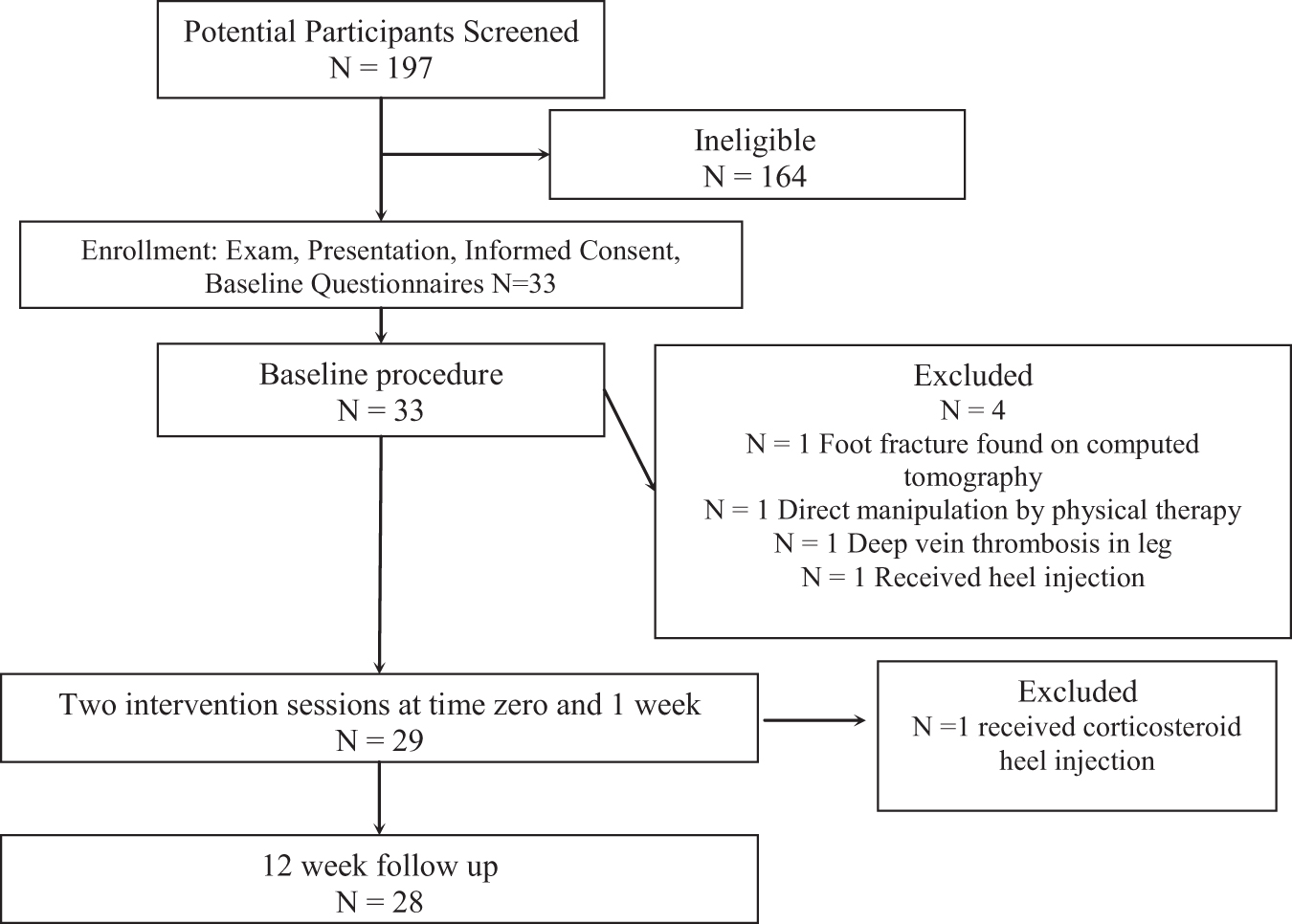
Enrollment intervention and follow-up of participants and completion of the study.
Participant Demographics
BMI ranging from 18.5 to 24.9.
BMI ranging from 25 to 29.99.
BMI ranging from ≥30.
N = number of cases; min, minimum; max, maximum; Junior Enlisted, rank of E ≤ 4; BMI, body mass index; FHSQ, Foot Health Status Questionnaire; MEB, Medical Evaluation Board; NCO, Non-Commissioned Officer representing enlisted ranks E5 to 9; NSAID, nonsteroidal anti-inflammatory drug; PT profile, presence of a current military duty-limiting profile; SD, standard deviation; TIS, time in military service; VAS, visual analog pain scale.
The study sample (N = 28; Table 1) consisted of 28 adults (13 female, 36.5 ± 7.6 years old, range 21–51 years) with a body mass index of 31.14 ± 5.19. 26 Baseline FHSQ and VAS scores, and plantar fascia thickness, suggest substantial disease severity. Participants reported 44.8 ± 55.5 months of PHP; 4 (12%) participants were undergoing a “MEB” (seeking disability-related compensation); 17 (60.7%) participants had a duty-limiting physical training profile. Among these, the duration of those on a duty-limiting profile was 669.7 ± 842.4 days. Most participants had tried and failed two or more conservative measures (Table 1). No participants were taking opioids at any time during the study. Based on the pain patterns identified by patients and palpatory examination findings, the treating physician identified herniated trigger point, folding, continuum, and trigger band fascial distortions. There were no cylinder or tectonic fixation fascial distortions.
Self-reported outcomes
Repeated-measures ANOVAs were performed for each of the eight subscales of the FHSQ encompassing baseline and follow-up 1- and 16-week data collection (Table 2). Significant, clinically relevant improvement from baseline to 1 week was reported in FHSQ scores for Foot Pain (33.8 ± 23.6 points), Foot Function (23.9 ± 19.8 points), Shoe (15.2 ± 24.0 points), and General Foot Health (20.7 ± 23.6 points) subscales (all p's ≤ 0.005; all effect size [ηp 2 ] estimates were considered large; Table 2); improvement in excess of MCID endured through 16 weeks. Significant change was not demonstrated on the General Health, Physical Activity, Social Capacity, or Vigor subscales (all p's ≥ 0.110; effect sizes [ηp 2 ] ranged from small to medium; Table 2). Twenty-three of the 28 (82%) participants met or exceeded the 14-point improvement MCID cutoff on FHSQ pain subscale. There was no statistical association between this response and any baseline demographic characteristics.
Outcome Data: Foot Health Status Questionnaire, Ultrasound, and Visual Analog Pain Scale Change Scores
Effect size estimation = partial eta squared (ηp 2 ) where small, medium, and large effect sizes represent 0.01, 0.06, and ≥0.14, respectively. F/U, follow-up. N = 28 for FHSQ and VAS. N = 28 plantar heel pain involved feet for ultrasound, sickest foot selected if both feet were available.
On the VAS, participants reported improvement in heel pain in excess of MCID (44.7 ± 27.7 points; p < 0.001; a large effect size [ηp 2 ] was demonstrated; Table 2) that followed a temporal pattern similar to the FHSQ pain subscale.
Baseline ultrasound evaluation identified 15/28 (54%) most effected feet as having a plantar fascia greater than 4 mm. Compared with baseline, 16-week follow-up demonstrated an average (SD) reduction in plantar fascia thickness of 0.6 mm (0.9 mm) (p = 0.001; this is considered a large effect [ηp 2 ] size; Table 2). The 12/13 (92%) fascia with baseline thickness less than 4 mm remained normal at 16 weeks. Among 15 fascia that were greater than 4 mm at baseline, 8/15 (53%) normalized from pathologic (>4 mm) to nonpathologic (≤4 mm) (Fig. 3a, b). There was no statistical association between intervention response and baseline demographic characteristics.

The fraction of participants on a duty-limiting profile decreased from 17/28 (61%) at baseline to 5/28 (18%) at 16 weeks. Nonsteroidal anti-inflammatory drug (NSAID) use decreased from 27/28 (96.4%) at baseline to 7/28 (25%) at 16 weeks. Anecdotally, participants were satisfied with care. Side effects included expected mild-to-moderate procedural pain in all but one participant who experienced brief moderate-to-severe pain. All procedural pain was self-limited and resolved within 10 min. There were no self-reported adverse events.
Discussion
This single-arm prospective effectiveness study of participants with PHP treated with an FDM-informed diagnostic and treatment protocol presents two main findings: after the FDM procedure, participants reported substantial consistent improvement exceeding the MCID for this indication on four of the eight FHSQ subscales, including the primary outcome Foot Pain, and a pain-specific VAS at 1 week (two treatment sessions) that endured through 16 weeks while also demonstrating large effect sizes. Second, ultrasound assessment showed decreased thickness in most participants and normalization of pathologic plantar fascia in some. Additional findings include reduced number of military profiles and decreased NSAID use. The current study is the first to objectively assess affected tissue after treatment with FDM-informed manipulation. While the authors are not able to assign causality outside a randomized clinical trial with comparison/control group, the severity and chronicity of participants' pain, rapid improvement after treatment, and concomitant ultrasound change suggest that FDM-based manipulation, rather than natural history or maturational effects, suggests that the receipt of FDM-informed care was a factor in the observed outcomes.
All participants were active duty personnel, although not athletes, which includes some daily physical activity. Therefore, the results likely extrapolate to a nonmilitary moderately active population. Although the physical activity component of the FHSQ did not reveal significant improvement, “on profile” status decreased by 70.5%, allowing those service members to return to full duty and suggesting substantial functional improvement. Increased readiness for deployment of a soldier and their unit is a primary goal of military medicine. Pain and function, while related, are understood to have independent elements. 27
FDM is an unconventional perspective from which to view anatomy and pain. It was developed by Stephen Typaldos, DO, who reported his identification of six different fascial “distortions,” pathologic anatomic alterations of the fascia, from 1991 to 1996. 9,10 Proponents identify fascia, the collagenous connective tissue that invests, stabilizes, and encloses muscles and internal organs, as a primary pain-generating tissue. 25 From the FDM perspective, purported distortions are understood to cause pain, present consistently, and are detectable to a trained FDM practitioner based on patient-reported pain distribution and palpatory examination. 25 They may be resolved using a distortion-specific manipulation. FDM is recognized by the American Osteopathic Association, used by osteopathic physicians and other manual therapists, and taught in some osteopathic medical schools, residency programs, and continuing medical education activities. 28
Little research has been conducted about FDM. The results of this study are consistent with reports using FDM principles and techniques for diagnosis of a fascial distortion and resolution of pain, respectively. Richter et al. in a prospective controlled trial compared the FDM with the German National Disease Management Guideline for the treatment of low-back pain. 11,29 As a stand-alone treatment, the FDM was noninferior and appeared to contribute to pain relief and functional improvement for the lower back. 11 Schulze et al. assessed treatment of medial tibial stress syndrome with the FDM in a prospective case–control study demonstrating favorable results after 6 days of treatment. 14 Maetzler et al. in a cohort study described the successful FDM-informed treatment of patients with ankle sprain. 17 In these reports, the authors have discussed the FDM procedures as clinically safe; however, no studies have been powered to detect rare or long-term side effects or adverse events.
No prior studies have investigated FDM-based care as a treatment for PHP. FDM-based therapy appears to compare well with other nonsurgical standard of care modalities. Numerous reports document inconsistent outcomes of other therapies, including corticosteroid injections, platelet-rich plasma injections, radiofrequency ablation, and shockwave therapy. 5,30,31 Corticosteroids are effective in the short term; however, multiple injections result in tendon rupture in an estimated 2.4% of cases. 4,5 Platelet-rich plasma injections may provide a more sustained improvement to 3 months 30,32 ; however, a meta-analysis showed minimal, if any, benefit compared with control. 33 Shockwave therapy appears safe, but it is more expensive and has a longer recovery and less change in the thickness of the fascia. 34,35 Radiofrequency ablation is relatively invasive and expensive, requires specialty equipment, and is not readily available. 31
The treatment of fascial abnormalities and FDM, in particular, is controversial, and content experts have called for more and better research. 9,36 The distortions themselves, and a mechanism of action for distortion-based pain resolution, have not been objectively demonstrated. Indeed, pain medicine has not historically focused on fascia as a pain-generating tissue. However, research suggests that fascia is a pain-generating tissue; the general principle that chronic pain diagnosis and treatment can be based on and be directed toward, fascia via fascial manipulation is therefore reasonable. 8,37,38 Free nerve endings, mechanoreceptors, nociceptive, and proprioceptive receptors found within the fascia likely are significant contributors to the pain, and proprioceptive changes are often seen in musculoskeletal injuries. 8,38 During an acute injury, proinflammatory cytokines can create a cascade of events leading to substance P and transforming growth factor beta that promote collagen deposition into the fascia and other connective tissue. 8 This increased collagen can tether or entrap nerves, increasing pain. 8 Indeed, osteopathy specifically addresses the myofascia; early research has reported that myofascial release can effect fascial pain generation. 39,40 One intriguing mechanistic possibility potentially related to FDM-informed manipulation for PHP involves focal compression or entrapment neuropathy of terminal branches of the inferior calcaneal nerves. 41,42 In this context, FDM-informed manipulation may release entrapments, for example, an entrapment causing the well-documented Baxter's neuropathy, and reduce pain, potentially through reduction of tissue- or nerve-based inflammation, or via a noninflammatory mechanism. 9,31
Limitations of this study include small sample size, short follow-up, lack of comparison or waitlist control group, and limited generalizability given its military-based cohort. However, patient-oriented outcomes were consistent and robust; disease-specific outcomes were provocative. Given that this was an initial study, the authors opted to employ a per-protocol analytic strategy in an effort to highlight the best-case scenario of the potential impact the FDM protocol may have on outcomes, which may introduce bias. Through replication with larger sample sizes in military and nonmilitary personnel within the setting of a randomized clinical trial and using an intention-to-treat analytic strategy, those results may or may not be as robust as those shown in this study. The authors did not formally assess patient satisfaction nor the therapeutic response of individual feet by self-report. NSAID use was not assessed in a dose-related manner.
Conclusions
Patients with PHP assessed and treated using strategy informed by FDM principles reported significant and sustained improvement on validated pain and function measures. Additional findings include reduction of plantar fascial thickness in some participants. While assigning strict causality in this single-arm prospective effectiveness study is not possible, these promising findings require replication and more rigorous corroboration with a randomized controlled trial employing larger military and nonmilitary patient samples.
Footnotes
Acknowledgments
Mickey Chabak, MD, Major, Medical Corps, United States Army, Musculoskeletal Radiologist, Chief of MRI Section in Dwight D. Eisenhower Army Medical Center and Fellowship trained in Musculoskeletal Radiology, overread of ultrasound images.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.