
Abstract
Objective:
To investigate the effects of 12 weeks practice of a structured yoga module on heart rate variability (HRV) and cardiometabolic risks in patients with type 2 diabetes (T2D) receiving similar kind of oral antidiabetic drugs (OAD) with yoga therapy and without yoga therapy, matched for all the known confounders.
Design:
Parallel design interventional (randomized control trial) study.
Subjects:
Eighty treatment-naive males with T2D were randomized into control group (n = 40) and study group (n = 40).
Intervention:
Study group participants received a structured yoga therapy that included asana and pranayama practice for 12 weeks in addition to OAD, whereas control group participants received OAD alone.
Outcome measures:
Before and after intervention, BP parameters, rate pressure product (RPP) as the marker of myocardial stress, total power (TP) of HRV, low-frequency to high-frequency (LF–HF) ratio of HRV, homeostatic model of insulin resistance (HOMA-IR), lipid profile and lipid risk factors, malondialdehyde (MDA), and high-sensitive C-reactive protein (hsCRP) were measured. TP of HRV was defined as the primary outcome. Association of TP (the marker of HRV) and LF–HF ratio (the marker of sympathovagal balance) with cardiometabolic parameters was assessed by correlation and regression analyses.
Results:
After 12 weeks yoga therapy, there was significant reduction in cardiometabolic risks (TP of HRV, RPP, lipid risks factors, levels of MDA, and hsCRP) in study group subjects compared with control subjects that did not receive yoga therapy. All cardiometabolic risk factors were significantly correlated with TP in study group, having maximum significance with homeostatic model of insulin secretion (r = 0.502, p ≤ 0.001). Multiple regression analysis demonstrated the independent contribution of decrease in RPP, HOMA-IR, hsCRP, and MDA to increased TP and decreased LF–HF ratio in T2D patients after yoga therapy.
Conclusion:
From the results of this study, the authors conclude that 12 weeks practice of a structured yoga module improves TP of HRV, sympathovagal balance, and metabolic functions, and reduce cardiovascular (CV) risks in patients with diabetes who received routine antidiabetic medicines along with yoga therapy, compared with the patients with diabetes who received antidiabetic medicines alone. The reduction in cardiometabolic risks in these patients is linked to the improvement in TP of HRV. Future studies should also include a control group with rapid walking or a similar exercise program of equal time to the yoga intervention group to discern whether it is in fact yoga that is leading to these results and not simply increased CV activity. Clinical Trial Registry of India (No. CTRI/2021/06/034074).
Introduction
Diabetes mellitus is a major public health problem globally. According to latest estimates, nearly 463 million people live with diabetes, which constitutes 9.3% in the general population. The occurrence of diabetes has been projected to increase to 25% in 2030 and 51% in 2045. 1 About 19% of diabetic population of the world is present in India and, therefore, India is considered as the diabetic capital of the world. 2 Diabetes being a chronic disease that requires life-long treatment, it has posed an economic challenge to the society. Owing to illiteracy and poor economic status of a sizeable population in India, the inadequate adherence to antidiabetic medications has resulted in considerable morbidity and mortality among the patients with diabetes. Therefore, efforts have been made to manage diabetes with alternative therapies that are less expensive and easy to practice. Recently, the authors have reported that the practice of yoga improves the quality of life, and decreases Indian Diabetic Risk Score (IDRS) and glycemic status in patients with type 2 diabetes mellitus (T2DM). 3
T2DM is known to be associated with increased risk of cardiovascular (CV) diseases. 4 The CV risk in T2DM has been stated to be linked to autonomic dysfunctions. The authors have reported that autonomic imbalance in the form of increased sympathetic activity and decreased parasympathetic activity contributes to CV risks in metabolic disorder, including obesity, hypertension, and diabetes. 5 –7 Excessive calorie intake, sedentary lifestyle, and increased plasma glucose levels provoke inflammation and oxidative stress (OS) in T2DM. 4 It has been described that dyslipidemia, OS, and inflammation are the possible pathophysiological mechanisms of diabetes severity and complications. 8 The reports from the laboratory have demonstrated the role played by insulin resistance, retrograde inflammation, adiposity, OS, and vascular endothelial dysfunctions in the etiopathogenesis of CV risks in diabetes and prediabetes in vulnerable population. 9,10
Sympathovagal imbalance mainly with sympathetic overactivity and reduced parasympathetic activity has been observed to be the cause of insulin resistance and metabolic dysfunctions in T2DM. 11,12 The authors have observed that enhancement in autonomic balance by yoga therapy leads to improvement in metabolic status, including glycemic control in T2DM. 3 Recently, the authors have reported total power (TP) of heart rate variability (HRV) as the marker of autonomic drive and low-frequency to high-frequency (LF–HF) ratio of HRV as an index of sympathovagal balance in health and diseases. 13 –16 Sympathovagal imbalance is known to be influenced by age, gender, body weight, and blood pressure of the individual. 17 Also, the authors have demonstrated that practice of yoga improves sympathovagal balance in prehypertension and hypertension. 18,19 Especially, they have observed the improvement in HRV and sympathovagal balance and CV functions after practice of pranayama, the slow breathing exercises. 20
There is a recent report of improvement of glycemic status and reduction in cardiometabolic risks in prediabetes after practice of yoga. 21 Also, there is a previous report of improvement of autonomic functions after practice of yoga in 15 patients with diabetes compared with their own preyoga practice values. 21 However, till date there is no report of the effect of practice of a structured yoga module on cardiometabolic risks in patients with diabetes receiving oral antidiabetic drugs (OAD) compared with patients with diabetes receiving OAD alone. The cardiometabolic risks are known to be more in males compared with females. 14 As such, diabetes in Indian population is more in males compared with females with a male–female ratio of ∼2:1. 2 Therefore, in this study, the authors have investigated the effects of 12 weeks practice of a structured yoga schedule on TP of HRV, lipid profile, inflammatory, and OS parameters in males with diabetes receiving similar kind of OAD with yoga and without yoga to assess the difference in improvement of autonomic functions and cardiometabolic status in these two group of patients.
Materials and Methods
Study design
This was a parallel design randomized control trial. After obtaining approval from Post-Graduate Research Monitoring Committee and the Institute Human Ethics Committee of Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, India, the trial was registered with Clinical Trial Registry of India (
For randomization, a computer-generated random number sequence was used. Random numbers were generated by an institute statistician who was not related to this project. The block randomization with random block sizes of 4, 6, and 8 were used. The sequence was concealed (allocation concealment) using serially numbered opaque sealed envelope (SNOSE), by the statistician. The third author (the clinician) enrolled the participants, and the first author (the MD student) allocated the patients with diabetes to one of the arms after assessing eligibility and after opening the envelope containing instruction for allocation to the group. After assignment to intervention, the second author was blinded, who had assessed the outcome measures. Approval of institute review board (IRB) was obtained.
Sample size calculation
The primary objective of the study was to assess the effect of yoga on HRV, that is, the TP of HRV and the secondary objective was to assess the cardiometabolic risks to sympathovagal imbalance. TP of HRV was defined as the primary outcome. Therefore, the previous reference of effect of yoga on autonomic function testing, including HRV in T2DM patients, 22 was considered for sample size calculation. The sample size was estimated using the statistical formula for comparing means with equal variance. With the minimum expected difference in the level of TP between the groups as 12 with the standard deviation of 3.7, the sample size was estimated at 5% level of significance and 80% power. The minimum sample size estimated for this study was 35 in each group. However, considering the dropout rate of about 10% as observed in the previous yoga research projects, the final sample size was estimated to be 40 in each group.
Grouping of the subjects
Control group (n = 40): Male T2DM patients receiving standard OAD treatment
Study group (n = 40): Male T2DM patients receiving standard OAD treatment + Yoga.
Inclusion and exclusion criteria
The males with diabetes between the age of 40 and 60 years, having normal body mass index (BMI), and prescribed to receive only metformin or glimepiride, or both in combination with atorvastatin were included for the study (Table 1). Patients receiving any other OAD or insulin and other medications, subjects with diabetic complications, with the history of coronary artery disease, other endocrine disorders, renal disease, autonomic dysfunction, inflammatory conditions, skeletal deformities, neuromuscular diseases, history of smoking and alcoholism, and subjects who were already practicing yoga were excluded from the study.
Medications Received by Diabetic Patients in Control Group and Study Group
As they were newly diagnosed diabetic patients, in both the groups either they had metformin as a monotherapy or the combination therapy of metformin+glimepiride. But both the groups were additionally treated with atorvastatin.
Procedures
Recording of anthropometric and basal CV parameters
The subjects were asked to report to autonomic function testing (AFT) research laboratory of physiology department at about 8 AM. Their height and body weight were recorded and BMI was calculated. After 15 min of rest in the supine position, the systolic blood pressure (SBP), diastolic blood pressure (DBP), and basal heart rate (BHR) were recorded using automated blood pressure monitor (Omron automatic blood pressure monitor HEM-8712; Omron Healthcare Company Ltd., Tokyo, Japan) and mean arterial pressure and rate pressure product (RPP) were calculated.
Recording of HRV
For HRV recording, the standard procedures of the AFT Lab as described earlier were followed. 6,20 The lead II ECG was recorded continuously for 10 min, and the data were acquired at the rate of 1000 samples per second for each channel using BIOPAC MP-100 data acquisition system (BIOPAC, Inc., USA). The RR tachogram obtained was analyzed using the Kubois software (Kubios HRV Version 1.1, Finland). The frequency domain indices such as TP, normalized low-frequency power (LFnu), normalized high-frequency power (HFnu), LF–HF ratio and time domain parameters such as standard deviation of normal to normal interval (SDNN), square root of the mean squared differences of successive normal to normal intervals (RMSSD), number of interval differences of successive normal to normal (NN) intervals >50 msec (NN50), proportion derived by dividing NN50 by the total number of NN intervals (pNN50) were calculated.
Biochemical parameters
Five milliliters of fasting blood was collected. Plasma glucose was estimated by GOD-PAP (Reckon Diagnostics, India) and insulin was assessed by enzyme immunoassay method (DiasourceInc, New York). For assessment of insulin resistance and secretion, the homeostatic model of insulin resistance (HOMA-IR) and homeostatic model of insulin secretion (HOMA-S) were calculated respectively using HOMA formula. 23 Total cholesterol (TC), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C) were assessed using fully automated chemistry analyzer (Olympus AU 400, USA) and low-density lipoprotein cholesterol (LDL-C) was calculated using Friedwald's formula. 24 The lipid risk ratios such as TC/TG, TC/HDL-C, LDL/HDL-C, TG/HDL-C, and atherogenic index of plasma (AIP) [Log10 (TG/HDL-C)] 25 were calculated. The high-sensitive C-reactive protein (hsCRP) was measured using ELISA kit (DBC, Canada) and malondialdehyde (MDA) was estimated by colorimetric method (Cayman's assay).
Intervention
For the subjects of the study group, three yoga training sessions on three consecutive days were held for sensitizing them for yoga practice. The yoga schedule for treatment of diabetes (Table 2) as prescribed by Bihar School of Yoga, Munger, India, and practiced at Advance Center for Yoga Therapy, Education and Research (ACYTER), JIPMER, Puducherry, was adopted for this study. 26,27 After the initial training, they could practice yoga 5 days per week (Monday–Friday) under supervision by a certified yoga instructor of ACYTER, JIPMER, Puducherry. During the remaining 2 days, they were instructed to practice the same yoga schedule at home. The yoga practice was continued for 12 weeks, after the postyoga training, and all parameters mentioned earlier were recorded (CONSORT Checklist).
Yoga Therapy Module
The details of the warm-up exercises, asanas, pranayamas, and relaxation (savasana) techniques have been described stepwise with the pictorial demonstration of each procedure in the Chapter of Yoga in Comprehensive Textbook of Medical Physiology. 47
The subjects of study group were instructed to practice yoga in addition to OAD as prescribed by the physicians. The subjects of control group were allowed to take OAD, but without practice of yoga. However, they were advised to do their routine works as per their daily normal schedule, throughout 3 months study period. All the parameters were recorded in patients of both study group and control group before 12 weeks (pretest) and after 12 weeks (post-test) of intervention. As adverse events have been reported to be associated with yoga, 28 patients were regularly monitored for development of any harmful or undesirable symptoms.
Statistical analysis
Statistical analysis was done using SPSS version 18 software (Chicago, IL, USA). Data were analyzed by Kolmogrov–Smirnov test for the normality. All data were expressed as mean and standard deviation. The data of eight dropouts were addressed as per the standard practice of handling missing data in randomized control trials. 29 As per Little's MCAR (missing completely at random) test, the dropout data were found to be MCAR. Therefore, observed data were used for analysis.
Comparison of postintervention data between the control group and study group was done by analysis of covariance (ANCOVA). The strength of correlation of TP and LF–HF ratio with cardiometabolic risk parameters was analyzed by Pearson's correlation. The independent association of TP and LF–HF ratio with the potential predictors such as BHR, RPP, HOMA-IR, Atherogenic Index (AI), and MDA was assessed by forward multiple regression analysis.
Results
Eighty-eight males with diabetes were randomized into control group (n = 42) and study group (n = 46) (Fig. 1). Two patients from control group and six patients from study group did not complete the 12 weeks intervention, as they moved to some other hospital for treatment. The preintervention (pretest) data of all the participants in control group (n = 42) and study group (n = 46) were considered for baseline comparisons, whereas the final sample size on completion of intervention (post-test) was 40 in each group. During the intervention period, two patients in the control group and one patient in the study group had common cold with mild fever for 2 days and they were treated with paracetamol tablets (500 mg, twice orally daily) and warm saline gargling of the throat. The patient in the study group who had common cold was advised not to practice yoga during 2 days of illness. As the illness was comparable in both the groups, it appears that the ailment was not related to yoga intervention. In general, the interventions in both the groups were found to be safe.
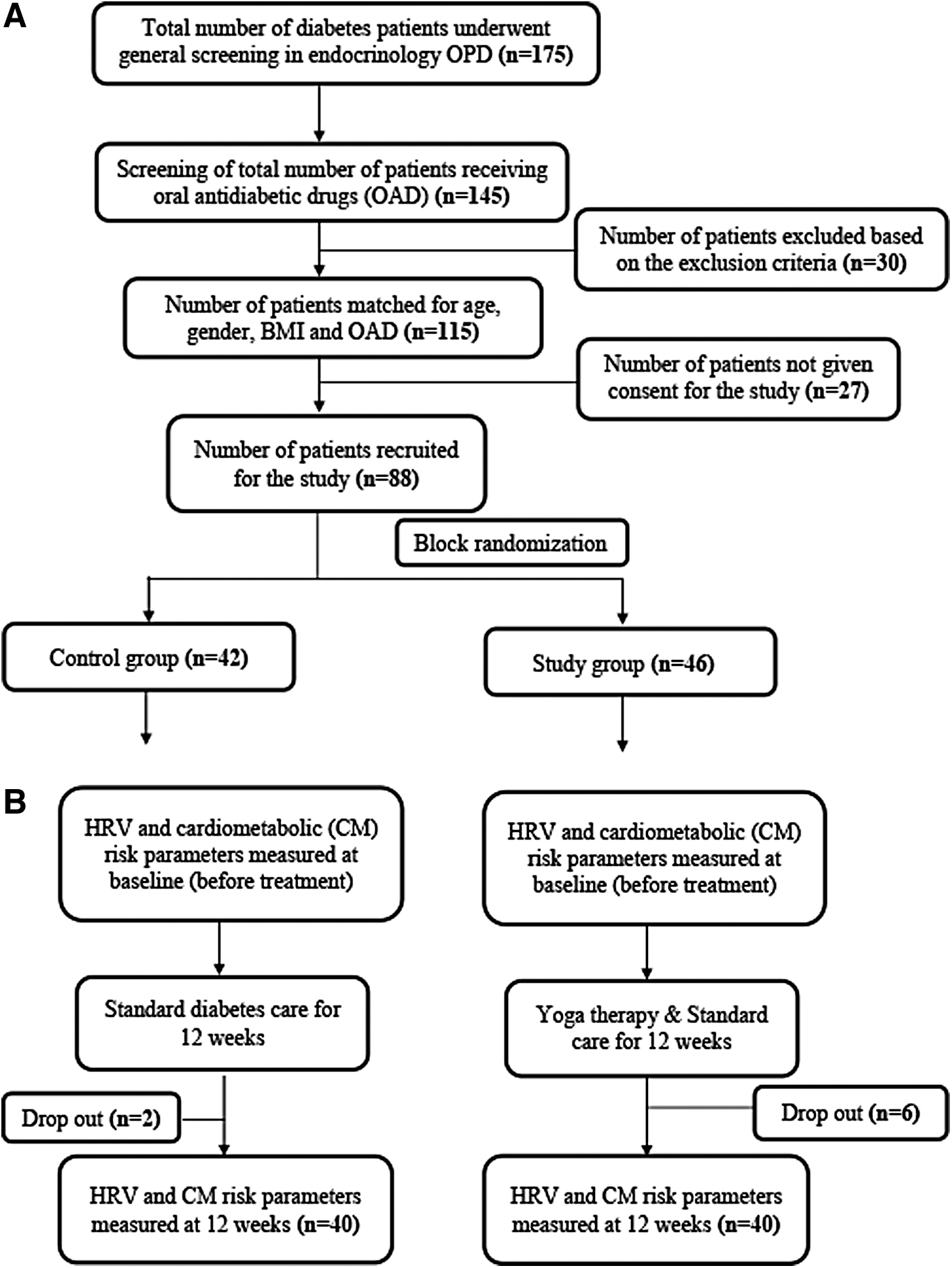
RCT consort flowchart. RCT, randomized control trial.
Anthropometric and CV parameters
There was no significant difference in body weight and BMI in study group compared with control group after 12 weeks of intervention (Table 3). CV parameters such as BHR (p = 0.012), SBP (p = 0.001), DBP (p = 0.056), and RPP (p < 0.001) were decreased in study group after 12 weeks in comparison with the control group postvalues (Table 3).
Descriptive Statistics and Analysis of Covariance Results of Post-Test (After 12 Weeks of Intervention) Anthropometric, Heart Rate, Blood Pressure, and Heart Rate Variability Parameters Between the Control (Diabetic Patients Receiving Oral Antidiabetic Drugs Alone) and Study Group (Diabetic Patients Receiving Oral Antidiabetic Drugs + Yoga) Subjects
Comparison of data between the control (post) and study (post) was done by ANCOVA. The p-value <0.05 was statistically considered significant.
ANCOVA, analysis of covariance; BMI, body mass index; CI, confidence interval; SBP, systolic blood pressure; DBP, diastolic blood pressure; BHR, basal heart rate; RPP, rate pressure product (SBP × DBP × 10−2); SDNN, standard deviation of the averages of NN intervals; RMSSD, square root of the mean of the sum of the squares of differences between adjacent NN intervals; NN50, number of interval differences of successive NN intervals >50 msec; pNN50, proportion derived by dividing NN50 by the total number of NN interval; TP, total power; LFnu, normalized low-frequency component; HFnu, normalized high-frequency component.
HRV parameters
SDNN (p = 0.005), RMSSD (p < 0.001), NN50 (p < 0.001), pNN50 (p < 0.001), TP (p < 0.001), and HFnu (p < 0.001) of HRV indices were significantly increased, and LF–HF ratio (p < 0.001) were decreased in the study group after 12 weeks compared with the postvalues of control group (Table 3).
Biochemical parameters
There was significant decrease (p < 0.001) in FPG (p < 0.001), insulin (p < 0.001), HOMA-IR (p < 0.001), TC (p < 0.001), LDL-C (p < 0.001), TG (p = 0.006) LDL-C/HDL-C (p < 0.001), TC/HDL-C (p < 0.001), TG/HDL-C (p = 0.002), AIP (p < 0.001), and MDA (p < 0.001), and significant increase in HOMA-S (p < 0.001) and HDL-C (p = 0.014) in study group after 12 weeks of yoga intervention compared with the control group postvalues (Table 4).
Descriptive Statistics and Analysis of Covariance Results of Post-Test (After 12 Weeks of Intervention) Biochemical Parameters Between the Control (Diabetic Patients Receiving Oral Antidiabetic Drugs Alone) and Study Group (Diabetic Patients Receiving Oral Antidiabetic Drugs + Yoga) Subjects
Comparison of data between the control (post) and study (post) was done by ANCOVA. The p-value <0.05 was statistically considered significant.
AIP, atherogenic index of plasma; ANCOVA, analysis of covariance; CI, confidence interval; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostatic model assessment-insulin resistance; HOMA-B, homeostatic model assessment-β cell function; HOMA-S, homeostatic model assessment-insulin sensitivity; hs-CRP, high sensitive C-reactive protein; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides; MDA, malondialdehyde; SD, standard deviation.
Correlation and regression analyses
Although there was no significant correlation of TP and LF–HF ratio with any of the parameters in the control group, the correlation of SBP, BHR, RPP, FPG, HOMA-IR, AI, and MDA with TP and LF–HF ratio (Table 5) was significant in the study group after 12 weeks of yoga therapy. The level of correlation was more with TP for all the parameters compared with the level of correlation with LF–HF ratio. In ANCOVA, the level of significance between post-test values of control group and study group was highest for HOMA-S (F = 457.603, p < 0.001, η 2 = 0.854), and in correlation analysis, the HOMA-S was more significantly correlated with TP (r = 0.502, p < 0.001) compared with LF–HF ratio r = 0.280, p = 0.041) (Table 5).
Pearson's Correlation of Total Power and Low-Frequency to High-Frequency Ratio with Heart Rate, Blood Pressure, and Biochemical Parameters in the Post-Test Groups of Both Control Group and Study Group Subjects
The p-value <0.05 was statistically considered significant.
AI, atherogenic index; BHR, basal heart rate; DBP, diastolic blood pressure; HOMA-IR, homeostatic model assessment-insulin resistance; hsCRP, high sensitive C-reactive protein; LF–HF, low-frequency to high-frequency
Multiple regression analysis demonstrated the significant individual contribution of RPP, HOMA-IR, AIP, and MDA to TP, in the study group after 12 weeks of yoga intervention (Table 6). Also, these parameters had significant association with LF–HF ratio in the study group after yoga intervention (Table 7). However, the level of contribution of RPP, HOMA-IR, and MDA was more with TP (Table 6), compared with the level of contribution of these potential predictors to LF-HF ratio (Table 7).
Multiple Regression Analysis of Total Power (as Dependent Variable) with Various Parameters (as Independent Variables) in Study Group Subjects After 12 Weeks of Yoga Therapy
The p-value <0.05 was statistically considered significant.
AIP, atherogenic index of plasma; CI, confidence interval; HOMA-IR, homeostatic model assessment-insulin resistance; MDA, malondialdehyde; RPP, rate pressure product; TP, total power of HRV.
Multiple Regression Analysis of Low-Frequency to High-Frequency (as Dependent Variable) with Various Parameters (as Independent Variables) in Study Group Subjects After 12 Weeks of Yoga Therapy
The p-value <0.05 was statistically considered significant.
AIP, atherogenic index of plasma; CI, confidence interval; HOMA-IR, homeostatic model assessment-insulin resistance; MDA, malondialdehyde; RPP, rate pressure product.
Discussion
In this study, 12 weeks practice of yoga resulted in notable improvement in HRV, as TP of HRV was increased in patients of study group who practiced yoga (Table 3) compared with patients with diabetes who did not practice yoga. TP depicts the strength of HRV and is considered as the most important indicator of overall vagal power of cardiac modulation. 30 It has been reported before that increase in TP is associated with decreased CV risks. 31,32 Also, decrease in TP has been reported to be associated with adverse cardiac events. 32 –34 Thus, increased TP in study group patients who practiced yoga indicates a considerable increase in CV health in them. In addition to improvement in cardiovagal modulation as reflected by significantly increased TP, the findings of this study indicate a considerable increase in cardiac vagal drive, as all the time-domain indices of HRV (SDNN, RMSSD, NN50, and pNN50) were significantly increased after 12 weeks of yoga therapy, symbolizing the substantially improved parasympathetic modulation of cardiac activity in study group subjects compared with control group subjects. It has been reported earlier that improvement in vagal tone is beneficial for CV health. 35 Thus, yoga therapy for 12 weeks appears to be effective in increasing TP of HRV, improving vagal power of cardiac regulation and decreasing CV risks in patients with diabetes receiving OAD. However, there was improvement HRV indices in control group subjects (OAD alone) also, although the level of improvement was significantly less compared with the improvements observed in study group (OAD+Yoga).
Although the exact mechanism of considerable improvement in TP of HRV in patients with diabetes who received 12 weeks of structured yoga module in addition to OAD compared with the patients with diabetes who received OAD alone, cannot be fully ascertained, it appears that it could be due to the substantial decrease in insulin resistance, OS, and dyslipidemia in yoga-treated patients. There was significant decrease in post-test value of HOMA-IR and increase in HOMA-S in the study group compared with post-test values of control group (Table 4), indicating the significant decrease in insulin resistance and improvement in insulin sensitivity in study group subjects after 12 weeks of yoga therapy. Since insulin resistance has been stated to cause autonomic dysregulation, 36 a greater alleviation of insulin resistance in subjects with diabetes after yoga therapy might have contributed to their substantial improvement in HRV and reduction in CV risk, as decrease in TP of HRV was significantly correlated with decrease in HOMA-IR in study group subjects (Table 5). However, the level of significance between post-test values of control group and study group was highest for HOMA-S (Table 4) and degree of correlation of increase in HOMA-S with increase in TP was more significant in study group (Table 4). HOMA-S has been reported as a maker of insulin secretion and sensitivity. 37 To avoid multicollinearity HOMA-S was not included along with HOMA-IR in multiple regression analysis (Table 6), which demonstrated the independent influence HOMA-IR on TP. Thus, the findings of this study indicate that increased insulin secretion and decreased insulin resistance could be associated with improved HRV. Three pranayamas included in the yoga therapy module in this study have been reported to improve vagal tone, 19,20,27 and increased vagal activity is known to facilitate insulin secretion. 38
Dyslipidemia is common in patients with diabetes, and dyslipidemia in diabetes has been reported to produce OS, 39 which then contributes to autonomic dyregulation. 40 In this study, all lipid profile parameters (except HDL) were significantly reduced in the study group (Table 4) after 12 weeks practice of yoga, and the AIP, a major lipid risk factor was significantly correlated with TP (Table 5). Moreover, in multiple regression model, AIP had a significant contribution to TP in study group subjects after yoga practice (Table 6), denoting that reduction in atherogenic lipid risk factors could have contributed to the improvement in HRV. Although there was significant improvement in lipid profile and decreased lipid risk factors in OAD-alone treated control group subjects, the improvements were significantly more in OAD+yoga treated study group subjects.
Although there was decreased hsCRP in the study group after 12 weeks of yoga therapy, it was not significantly different from post-test value of control group. Nevertheless, low-grade inflammation triggers autonomic imbalance influenced by insulin resistance, inflammation, dyslipidemia, and OS in first-degree relatives of patients having type 2 diabetes. 41 Dyslipidemia and OS are part of the pathophysiology of T2DM. 8 In this study, MDA was significantly decreased in the study group after 12 weeks practice of yoga (Table 4) and had a significant correlation with TP (Table 5), indicating that decreased OS might be associated with improvement in HRV. As MDA had independent contribution to TP, reduction in OS could be the link between the decreased atherogenic lipid profile and improved HRV in patients with diabetes after 12 weeks of yoga therapy. Nonetheless, reduction in OS has been reported to be a major contributor to the improvement in autonomic functions after yoga therapy administered as part of management in various metabolic disorders, including T2DM. 42
There is a report of improvement in glycemic status after practice of yoga in diabetes. 43 Also, there are reports of decrease in BP, OS, and lipid risk factors in T2DM patients after yoga practice. 42,44 In this study, there was significant decrease in RPP in study group subjects after 12 weeks of yoga therapy (Table 3) and RPP had independent association with TP (Table 6). As RPP, the marker of myocardial work stress, 45 has been reported to be reduced in FDR of T2DM patients after yoga practice, 46 the reduction in RPP is likely to reduce the CV risks in patients with diabetes. To the best of the authors' knowledge, till date there are no reports of effects of practice of yoga on HRV, RPP, and cardiometabolic risks in drug-treatment-matched patients with diabetes. Also, the duration of diabetes and many oral antidiabetic agents have been reported to influence autonomic functions in T2DM. Therefore, in this study, the authors had selected drug-naive (before initiation of OAD) patients with diabetes, receiving similar kinds of OAD (metformin and glimepiride) in both the groups.
In this study, there was significant decrease in LF–HF ratio in study group patients after yoga practice compared with the decrease in LF–HF ratio in control group patients. Decrease in LF–HF ratio indicates decline in sympathetic activity, enhancement in parasympathetic activity, and improvement of sympathovagal balance. 30 Thus, autonomic balance was remarkably increased in patients with diabetes who practiced yoga in addition to receiving OAD. Furthermore, all the cardiometabolic risk parameters were significantly correlated with LF-HF ratio and had independent contribution to LF–HF ratio after 12 weeks practice of yoga. Thus, findings of this study indicate increased sympathovagal balance could be linked to decreased level of cardiometabolic risks.
The 12 weeks practice of yoga resulted in increase in TP of HRV, improvement in sympathovagal balance, increased parasympathetic drive, and decreased sympathetic drive in the patients with diabetes receiving OAD. It appears that decreased OS, decreased lipid profile, and decreased AI have contributed to improved HRV and sympathovagal balance and thus have reduced the CV risks in these patients. India being a developing country, the addition of yoga to the conventional OAD drugs in the treatment of T2DM patients will certainly reduce the cost of management of patients with diabetes and improve their CV health. The limitations of this study are the modest sample size and absence of body composition analysis as a parameter of investigation in patients with diabetes. Also, the authors do not know if walking or other CV exercise for the same amount of time would yield a similar result to the yoga group. Thus, a major limitation of this study design is that they have not included subjects performing the walking or rapid walking as another control group, which would have helped them to prove if yoga indeed has made the difference and not just the increased CV activity. Furthermore, there may even be other yoga programs that may prove to be more efficient than the current program of this study.
Conclusions
From the results of this study, the authors conclude that 12 weeks practice of a structured yoga module improves TP of HRV, autonomic, and metabolic functions, and reduce CV risks in patients with diabetes who received routine antidiabetic medicines along with yoga therapy, compared with the patients with diabetes who received antidiabetic medicines alone. Thus, yoga is a promising adjuvant to medical treatment in improving CV health of patients with diabetes. Nonetheless, studies should be conducted in larger sample size to both confirm and extend the added benefits of yoga in T2DM. Also, the future studies should include an extra control group of subjects performing the walking or rapid walking to test if yoga indeed makes the difference and not just the increased CV activity.
Footnotes
Acknowledgments
Authors acknowledge the institutional intramural grant of MD Dissertation work received from JIPMER, Puducherry, India, for conduct of this study as part of postgraduate programme for the first author under the guidance of the second author.
Authors' Contributions
Conduct of the study, data analysis, and preparation of the article by M.D.; formulation of hypothesis, design of the study, supervision of the work of the study, data analysis, and preparation of the article by G.K.P.; design of the study and supervision of the work of the study by J.S. and P.P.; technical supervision of the study and data analysis by N.N.; work of the study and preparation of the article of the study by M.R. All the coauthors have reviewed and approved the article before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was carried out by JIPMER intramural academic funding.
Supplementary Material
CONSORT Checklist