
Abstract
Objectives:
A previous systematic literature review (SLR) evaluated 501 experiments on reducing patient anxiety across medical and dental environments. This integrative review examines those interventions and explores possible mechanisms leading to relative success or failure within those environments, in the interest of interprofessional education and communication.
Methods:
Reviewers evaluated 501 experiments testing interventions for reducing patient anxiety in a variety of medical and dental health care settings. Methodology for the SLR, largely following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, is briefly reviewed.
Results:
A total of 501 experiments (from 408 articles) met review criteria. One hundred and forty-three Music experiments were included, and Music interventions were largely effective, except in the case of colonoscopy. Education is the only intervention that occasionally (5 times of 130 experiments) raised patient anxiety in the face of a procedure; the discussion focuses on the wisdom of assessing patient need for information. Thirty-seven Cognitive Behavioral Therapy (CBT) experiments of various types are included, with a success rate of 89%, with a particularly high rate of success (12 of 12 experiments) in dentistry. Massage has a success rate that is similar to that of CBT, but Massage has been tested in far fewer specialty areas. Relaxation has been tested in every specialty area, except mechanical ventilation, with promising results. Acupuncture and Acupressure have not been widely tested, but their effectiveness rate is 100% when it comes to reducing patient anxiety in various procedural settings. Similarly, experiments show Hypnosis to be successful in 90% of trials. In contrast, Distraction was successful in only 40% of the experiments summarized, although it was more effective in dentistry. A variety of Nature-based Interventions (Aromatherapy, Nature Sounds, and Visual Stimuli) were highly successful across a variety of settings.
Discussion:
Possible mechanisms are discussed, along with commentary on feasibility. Limitations include publication bias, small sample sizes, and the lack of placebo controls. Future areas of research are pointed out.
Introduction
Health care providers interested in reducing patient anxiety through nonpharmaceutical interventions can benefit from interprofessional communication of research. 1 A companion systematic literature review (SLR) presents the importance of a large-scale SLR on reducing patient anxiety across health care settings, describes the methodology, and reports patterns of findings. 2 Based on 501 experiments captured in that SLR, and the different results across health care areas, the same researchers wrote this integrative review exploring possible reasons for the findings. This review addresses the question: What are the mechanisms that explain why effective interventions work?
Methods and Results
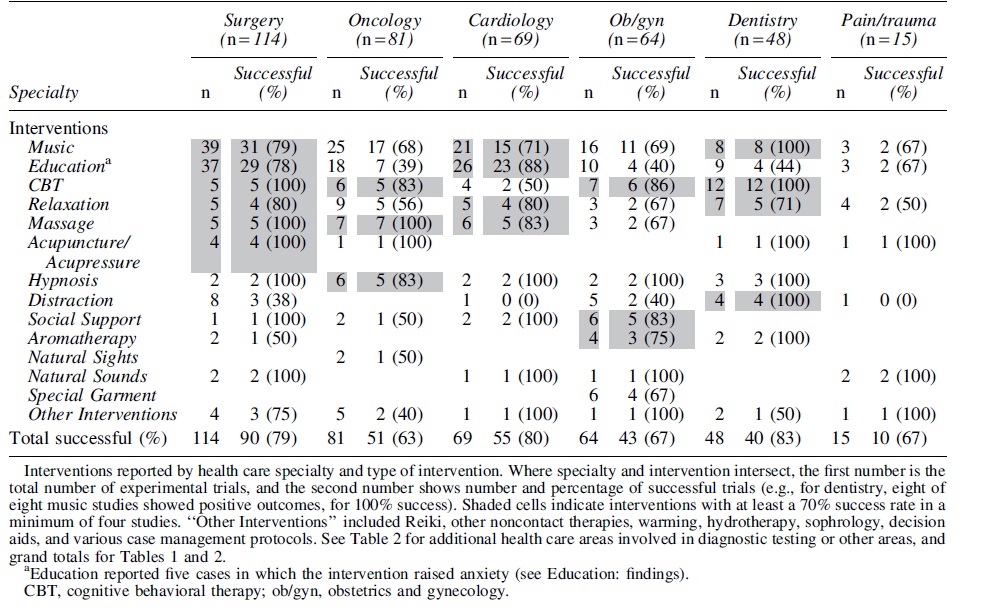
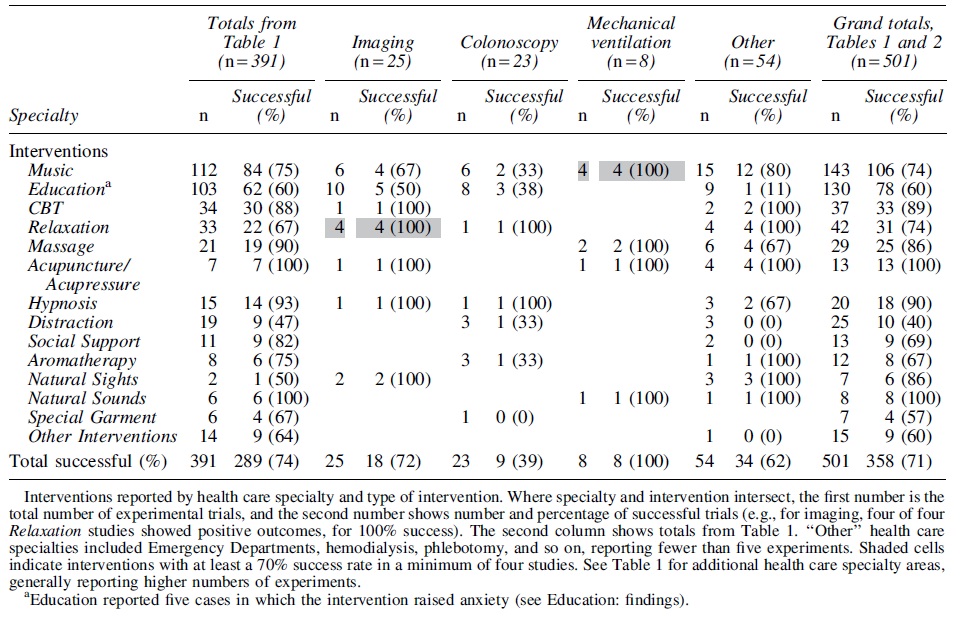
The companion SLR describes the protocol, search strategies, database information, and methods. The literature search captured 48,324 citations. After abstract review, 718 articles on reducing patient anxiety were read in full and coded for risk of bias and other criteria. The SLR identified 408 articles, containing 501 experiments, published between 1974 and 2018. The SLR answers three research questions concerning use of interventions in particular health care areas. Those results are summarized in Tables 1 and 2 (reprinted from the SLR) with additional notations pertinent to this discussion.
Reported Experiments by Health Care Area (Health Care Specialties)
Reported Experiments by Health Care Area (Diagnostic Testing, Mechanical Ventilation, Other)
Discussion
The tables show 71% of 501 experiments generating a statistically significant reduction in anxiety in the intervention groups compared with the control groups (or placebo groups). Acupuncture/Acupressure and Natural Sounds yielded success rates of 100%; however, they included relatively few experiments. Hypnosis, Cognitive Behavioral Therapy (CBT), Massage, and Natural Sights all reported success rates in the 80%–90% range, with relatively few experiments. Both Relaxation and Music reported 74% success, with Music having the most experiments (143). Next are Social Support (69%) and Aromatherapy (67%), with relatively few experiments. The lowest levels of success are seen in Education (60%), Special Garment (57%), and Distraction (40%). Other Interventions, which included Reiki, decision aids, and a variety of protocols, had 60% success in very few experiments.
What are the mechanisms that explain why effective interventions work for patients? This question is addressed, by intervention (Tables 1 and 2), largely in order of number of experiments. The discussion will draw from other reviews to discuss possible mechanisms and feasibility.
Music
Music: findings
More than one fourth of the articles included utilized Music as an intervention (with 74% success). Both genders benefited across many different countries, in all medical and dental procedures, except for colonoscopy.
No clear patterns emerged regarding mechanism of delivery, with null results reported with and without headphones. One study using headphones with or without music found that noise-canceling headphones alone did not reduce either pain or anxiety during prostate surgery. 3 One Taiwanese study directly compared music via headphones and music via broadcast system for anxiolytic effects on presurgical patients; both music delivery systems reduced anxiety when compared with controls. The authors recommended broadcasting music when there are sanitation concerns with headphones. 4 It appears that Music itself reduces anxiety, rather than noise-canceling headphones.
Music: mechanisms
Limiting patient choice may affect results. One study yielded success when patients chose easy listening CDs from 20 options 5 ; however, null results were found in two other preselected library studies. 6,7 In contrast, Ilkkaya et al. 8 asked surgery patients to bring in “their favorite music,” letting patients control the volume via headphones, comparing them with one group listening via headphones to operating room noise (a placebo group) and another group listening via headphones to white noise. Their music group showed a dramatic reduction in anxiety compared with both other groups. Ferrer achieved similar success, using a live guitarist and letting chemotherapy patients choose the melody. 9 Augustin and Hains said that their patients “verbalized the importance of personally choosing their music selections,” with 50% preferring to bring their own had it been suggested. 10(p. 750)
Studies identifying music genre often found classical music (Western, Turkish, or Chinese), easy listening, folk music, slow ballads, or jazz preferences. Slow-beat music is consistent with what music experts recommend—a steady tempo, slower than a normal heart rate, with a moderate volume. 11 Results for binaural beats (two tones, heard simultaneously, one in each ear) are mixed. One experiment found that binaural beats significantly reduced anxiety during dental surgery. 12 But two other studies found that Music significantly reduced patient anxiety, with or without binaural beats. 13,14
Music can easily be combined with other interventions. Sogabe et al. randomly assigned at least 50 patients to each of three groups: music, nature image on a television screen, and music plus image. 15 All intervention groups showed significantly reduced anxiety compared with controls, but the group with music-plus-nature-image showed the greatest reduction.
Music may distract patients from hospital noise, which can be twice as high as environmental experts recommend. 16 Yet, as reported above, noise-canceling headphones alone do not seem to reduce anxiety. 3 Other findings suggest that 15 min of music will lower anxiety, but 30 min is better. 17 Some assert that music entrains the body's natural rhythms, dampening autonomic nervous system (ANS) responses. 18 They point to studies documenting music lowering heart rate, respiratory rate, and blood pressure in patients on ventilators. 19
Education
Education: findings
Of 130 Education experiments, 78 reported meaningful reduction in patient anxiety, 47 reported null findings, and heightened anxiety was reported in 5 experiments from four different countries. 20 –24 Education in its various forms (by pamphlet, video, phone call, etc.) is the only intervention reviewed here showing contradictory findings, sometimes reducing and sometimes increasing patient anxiety. Guo showed similar results. 25 This pattern was seen in both genders, across most medical and dental procedures.
Education: mechanisms
According to Leventhal and Johnson, effective patient education addresses procedural and sensory information and behavioral instruction; they concluded that sensory information might be the most valuable for reducing anxiety. 26 Their recommendations were supported in a study providing surgical patients with a booklet containing procedural, sensory and temporal information, along with suggestions for coping with presurgical fear and recovery. 27 A patient's own need for knowledge may be a crucial predictor of how they will react emotionally to information. Peterson, looking at coping styles, identified cardiac catheterization patients as either “blunters” who seek distraction or “monitors” who desire more information. 28 Both groups showed lower anxiety after experiencing an educational intervention. Later research instruments focused on the patient's need for information in the health care context. One colonoscopy study identified patients as “information seekers” or “information avoiders” and provided normal procedural information or procedural plus sensory information to half of each group. 29 Patients were less anxious if they received the amount of information they preferred. But, findings were mixed in a dental clinic setting that included a placebo condition. 30
Importantly, some studies find that even information seekers do not experience reduced anxiety if they are given more information than they can comfortably process. One study tested needs-based education in day surgery patients in Thailand. 31 A control group had a traditional presurgery educational script read to them. The needs-based group first completed a self-administered questionnaire identifying how much information they wanted (from none to detailed). Notably, the needs-based group wanted less education, received less education, and showed a greater reduction in anxiety than the traditionally educated group.
The medium of information delivery may be important. One of the least successful interventions was patient education through video. If characterized more as distraction than education, the intervention was particularly ineffective (see the Distraction section). Even when the video was designed to enhance the patient's understanding, results have been mixed. In one colonoscopy study, half of the patients chose whether or not to watch an educational video, and the other half were randomized to educational video or no video; all groups became more anxious. 23
Relaxation (including guided imagery)
Relaxation: findings
Of 42 Relaxation experiments, 31 (74%) lowered patient anxiety. Various techniques were utilized, including deep breathing, progressive muscle relaxation (whole body or parts of the body, such as the jaw), autogenic relaxation, meditation, and mindfulness (sometimes with guided imagery or biofeedback). All 42 experiments utilized short-term interventions that were relatively easily administered, although many required training to administer correctly. For example, Litt et al. taught dental surgery patients autogenic relaxation (thinking of one's body as gradually getting heavy and peaceful) just before third molar extraction, with resultant lower anxiety compared with controls or patients given medication. 32 Another group received both autogenic relaxation and a CBT technique called “self-efficacy enhancement” and the combination reduced anxiety further.
Relaxation: mechanisms
Relaxation may be seen as an intermediate goal on the path to lowering ANS arousal; it is sometimes mentioned in discussions of music, massage, hypnosis, CBT, and other complementary and alternative medicine and psychological interventions. Relaxation, however, is sometimes directly pursued by means of relaxation training, biofeedback, guided imagery, mindfulness training, and so on, with focus on deep breathing and progressive muscle relaxation. Some techniques ask the patient to focus on one pleasant image to eliminate distressing thoughts. These techniques generally are effective when compared with controls or placebo treatments. 33
Cognitive behavioral therapy
CBT: findings
CBT showed a success rate of 89% in 37 studies. These studies were classified as CBT rather than Education if the focus was on teaching patients about their own emotional and psychological reactions (coping). Many different types of CBT were utilized, including “iatrosedation by dentist.” 34 One study utilized more common CBT interventions: “self-efficacy” therapy combined with needle desensitization with one group, and “self-efficacy” therapy plus relaxation in another group. 32 Both experimental groups showed significant anxiety reduction when compared with controls and a group given anxiolytic drugs. Other CBT techniques included psychoeducation, stress management, and group therapy, provided by nurses, psychologists, social workers, dentists, and other health care providers; in some cases, video training or a self-paced computer program was utilized.
CBT: mechanisms
CBT is generally effective in treating anxiety, 35,36 usually by providing a psychoeducational component that teaches the client how thoughts, feelings, and behaviors are interrelated. 37 Clients are then shown how to restructure dysfunctional beliefs and thoughts to improve mood and behavior. 38 CBT interventions for anxiety also include behavioral experiments, imaginal and in vivo exposure to feared images, bodily sensations, and situations, weaning of safety signals, and relapse prevention. 39
CBT was highly effective for dental anxiety probably because it addresses dysfunctional thoughts about dental treatment. 40 Patients often think that the treatment will be painful, dental staff will be judgmental of their hygiene, or the dentist will make a mistake. 41,42 Patients undergoing CBT for dental anxiety have reported cognitive restructuring and other coping skills as particularly beneficial in reducing distress. 43 Finally, CBT can be an effective intervention as it teaches the patient how to identify and evaluate dysfunctional thoughts and beliefs. 38 Patients may thereby feel more empowered, which further reduces anxiety.
Massage
Massage: findings
Twenty-five of 29 experiments reduced patient anxiety (86% success). Both genders benefited from Massage, across several medical procedures in many countries. Massage was not tested for dentistry, imaging, colonoscopy, or pain/trauma. Field's definition of Massage (“manipulation of soft tissue by trained therapists for therapeutic purposes”) was useful in classifying this group of articles as Massage or Other.44(p. 1270) Two studies utilized Krieger–Kunz Therapeutic Touch, which is based on a belief that vital energy can be balanced if a practitioner passes hands over or gently touches the patient's body. 45 One article employed Reiki, passing hands near the patient to transfer energy and facilitate healing. 46 We classified these studies as Other Interventions rather than Massage.
Twenty-four studies included various massage types: Swedish, back, hand, one Healing Touch (light touch), two Tactile Touch (a type of effleurage), one Tellington Touch (originally developed for nonhumans), one with hand holding, and another holding a hand on the patient's shoulder. In addition, five studies utilizing reflexology were analyzed in the Massage group. These 29 experiments tested techniques involving physical contact, with possible manipulation of soft tissue, as described by Field. 44 In 28 studies, a health care provider performed the massage, but in one labor and delivery study, the woman's partner performed massage. Twenty-five of 29 experiments (including the labor partner study) reduced patient anxiety. All five reflexology experiments successfully reduced anxiety, including one that compared hand massage to foot massage; researchers found that both groups benefited, but foot massage was significantly more effective. 47
A rapid review limited to cardiac catheterization patients included two massage experiments, only one of which reduced anxiety (both articles were included in our companion SLR). 48 Importantly, many of the 29 Massage interventions were single interventions, performed by someone with a reasonable amount of training, with minimal effect on care routines. For example, the labor partner was taught to do 30-min massage of the woman's abdomen, shoulders, and back during each stage of labor; the massage group experienced lowered pain and anxiety during the first (latent) phase of labor, although pain and anxiety increased for both the massage group and control group as labor intensified. 49 Couples reported that the massage protocol was easy to learn and helpful.
Massage: mechanisms
Field clarified that, while light touch (e.g., tickling) may be aversive, deep massage of soft tissue yields multiple benefits. 44 Using Gate Control Theory as a theoretical explanation, Chang et al. hypothesized that massage may stimulate large diameter fibers, thus closing the gate and minimizing the perception of pain, usually reducing anxiety. 49 A meta-analysis of massage therapy studies described reductions in state anxiety, blood pressure, and heart rate (but not cortisol) with a single application of massage therapy. 50
Anxiety typically is accompanied by heightened ANS activity. One theory suggests that massage works by shifting the ANS from a sympathetic response (which prepares the body to defend against threat) to a parasympathetic response. ANS arousal is associated with feelings of tension, increased stress hormone levels, and increased cardiovascular activity while a parasympathetic response is associated with feelings of calmness and well-being, and possible heightened immune system functioning. A parasympathetic response may involve stimulation of vagal activity, which is associated with applied pressure during massage therapy. 44 Although these theories offer great promise, none is universally supported. 50 Field also suggested that serotonin “may inhibit the transmission of noxious nerve signals to the brain,” 44(p. 1274) but the meta-analysis by Moyer et al. yielded only two studies linking Massage to increased serotonin. 50 Additionally, the meta-analysis suggested that cortisol is not significantly reduced by single applications of massage, an effect that would be expected with the activation of a parasympathetic response. 50 Thus, the literature provides contradictory findings regarding mechanisms.
Another promising neurophysiological mechanism theory suggests that Massage may result in an increase in oxytocin, a hormone known to facilitate social bonding. 51 Oxytocin has been shown to moderate ANS and vagal pathways, to have anti-inflammatory effects, 52 to reduce blood pressure and cortisol levels, 53 and to have physical analgesic effects. 54 Oxytocin levels in normally cycling women rose in response to relaxation massage and fell when sad emotion was evoked, with some interpersonal differences related to relationship history. 55 A recent study showed that a 10-min foot massage (by means of the caregiver's hands) was more effective than machine massage, in terms of releasing oxytocin and enhancing feelings of well-being. 56 Oxytocin has interactions with several components of the hypothalamic–pituitary–adrenal axis; clearly, more research is warranted. 57
Hypnosis
Hypnosis: findings
Eighteen of 20 hypnosis experiments reduced anxiety (90% success). Both genders benefited from hypnotic intervention, across a variety of medical and dental procedures; but no Hypnosis experiments met the SLR inclusion criteria for pain/trauma or mechanical ventilation. Notably, the 20 studies included here involved short-term hypnotic interventions.
Montgomery et al. defined Hypnosis as an agreement to participate in a “psychotherapeutic technique based on the hypnotist providing suggestions for changes in sensations, perception, cognition, affect, mood or behavior.” 58(p. 80) A 2019 meta-analysis concluded that Hypnosis is highly effective in reducing anxiety, with participants receiving hypnosis showing more improvement than 79% of controls. 59 They found no differences between interventions that incorporated self-hypnosis training and those that did not. Hypnosis was found to be more effective when combined with other psychological treatments for reducing anxiety, such as CBT, than when used alone.
Hypnosis: mechanisms
Hypnosis is explained as a special state or a set of socio-cognitive processes. The former idea posits that hypnosis leads an individual to enter a trance state 60 or a state of dissociation. 61 The dissociated control theory suggests that hypnosis activates lower order brain subsystems without involving higher conscious functioning. 62 Alternatively, the socio-cognitive processes approach suggests that hypnosis works by changing the patient's expectations about the outcomes of a social context. 63 Patients may be more amenable to change their outcome expectancies in a medical setting where they trust their health care provider. 64 When combined with CBT in the treatment of anxiety disorders, such as PTSD, hypnosis may augment the treatment. 65 It helps the patient to achieve affect regulation by promoting self-soothing and reducing general arousal, which frees the patient to think more clearly.
Despite many studies showing successful use of hypnosis in treating discomfort, distress, fatigue, and pain in medical procedures, the adoption of hypnosis in medical settings is relatively low. Broadening training could increase adoption levels. Hypnosis is cost-effective and can easily be structured to meet the needs of patients and providers, including training patients in self-hypnosis. 64
Acupuncture and acupressure
Acupuncture: findings
Six Acupuncture studies reduced patient anxiety (100% success). The studies included male and female adult patients in medical settings (and one dental setting) in China, the United States, Italy, Austria, and Turkey. Acupuncture is based on the idea that vital energy (qi) flows through the body in channels (meridians), and, if that energy is interrupted, disease results. Acupuncture needles are used to stimulate specific points on the meridians to restore balance and wellness to the person. 66 Four studies included a “sham” acupuncture group (placebo control). In the dental clinic study that used auricular acupuncture, both the true acupuncture and the sham group showed lower anxiety levels than the control group. 67 The authors acknowledged a possible placebo effect, but they stressed that, while both groups benefited from 20 min of treatment, true Acupuncture yielded a benefit that was both statistically significant and clinically meaningful compared with placebo.
Acupuncture: mechanisms
The mechanisms of Acupuncture are not well understood. 67 Acar suggests that acupuncture has physiological effects at three levels of the body. 66 At the peripheral level, it stimulates the release of endogenous opioids, diminishing pain perception; additional changes at the spinal and supraspinal levels further inhibit anxiety and the sensation of pain. Some authors argue that auricular acupuncture has advantages because it is easier to learn. 67
Acupressure: findings
Acupressure utilizes pressure or massage (by hand or specialized tools) applied by the practitioner to specific points on the energy meridians of the patient. The SLR yielded seven studies of Acupressure, all successful with both males and females, in Iran, Taiwan, India, Austria, and Malaysia, in a variety of medical settings (no dental). Three Acupressure studies utilized “sham” acupressure (placebo control group). One study compared two groups of patients on mechanical ventilation, over 17 days; one group received 6 min of shoulder massage followed by 9 min of acupressure (hands and ears) while the comparison group received 6 min of shoulder massage followed by handholding. 68 By the third treatment, the acupressure group reported lower anxiety than the massage comparison group. Acupressure is a simple and noninvasive intervention that can easily be taught to nurses, patients, and their family members. 68
Acupressure: mechanisms
Acupressure may release neurotransmitters that lead to relaxation. 68 Conceivably, Acupressure benefits could occur from practitioner touch—like the Massage benefits described above. This could be an additional advantage if the points of physical contact are stimulating neural pathways identified within Traditional Chinese Medicine as benefiting particular physiological systems.
Social support
Social support: findings
Nine of 13 experiments were successful (69% success). Social Support was operationalized as group support, couple support, presence or absence of family or partner, or intentional or empathic support of the health care provider. Five experiments were in fertility treatment settings or labor and delivery settings, and all five yielded positive results. The null findings were in surgical or testing settings. There is a long tradition (e.g., midwifery) of providing family and social support in the context of childbirth and for pediatric patients, and more research with adults is warranted.
Social support: mechanisms
Social Support may include material and emotional assistance from others, and there is a strong correlation between relationship longevity and Social Support. 69,70 On the physiological level, the “stress-buffering hypothesis” suggests that Social Support lessens the impact of stress on one's body. 71 Osterweis et al. suggests that persons who live in close proximity experience social entraining that affects one another's circadian rhythms, which regulate bodily functions including the immune system. 72 Thus, the continuing presence of a close companion might assist with anxiety management; conversely, the withdrawal of that companion might increase anxiety. In light of the finding that females are more sensitive than males to social support effects, 70 it is not surprising that most of the successful experiments with Social Support described here were conducted in obstetrics and gynecology (ob/gyn) settings.
Nature-based stimuli: aromatherapy, nature sounds, and natural sights
Twelve experiments employed natural odors (Aromatherapy), and an additional 42 experiments investigated using some other type of stimulus to comfort or distract the patient. These experiments seemed to fall into two general conceptual approaches, one involving natural stimuli, discussed below as Nature-based Interventions and the other involving innovative stimulation, with 25 studies classified as Distraction.
Nature-based interventions type I: aromatherapy
Aromatherapy: findings
Twelve studies were included and eight reduced anxiety (67% success). Fragrances included lavender, orange essence, grapefruit oil, and Osmanthus oil. Both genders benefited from Aromatherapy intervention for dentistry, colonoscopy, ob/gyn, and surgery.
Aromatherapy: mechanisms
Several studies proposed differing hypotheses explaining the success of Aromatherapy in reducing patient anxiety. The simplest hypothesized that patients benefited from the extra attention. 73 One meta-analysis investigating inhalation aromatherapy reported a significant reduction in cardiac surgery patients' anxiety, especially with lavender scent. 74 They hypothesized that stimulation of olfactory nerves directly impacted the limbic system, lowering stress hormones; the authors highlighted one study that showed inhaled lavender essence lowered cortisol levels. 75 The meta-analysis reported a pattern of reduction in anxiety and heart rate but not blood pressure. 74
Herz pointed out that only a few synapses separate the human olfactory nerve from the amygdala (emotion and motivated behavior) and the hippocampus (memory). 76 Thus, odor effects are nearly instantaneous and do not require processing in the bloodstream, which might delay impact for 20 min. Herz asserted that aromatherapy's neurochemical effects are probably overridden by psychological effects such as cultural conditioning in humans. 76 Another review of oxytocin effects 57 proposes a “hypothalamic–pituitary–adrenal (HPA) axis–oxytocin model” to address the question of why meditation and certain fragrances reduce anxiety. Another possible mechanism is offered by the Biophilia Hypothesis, which is discussed in the section on Natural Visual Stimuli.
With regard to Aromatherapy, the point raised by Herz is crucial that culture, personal experience, and expectation should be considered. 76 Humans evolved with rudiments of powerful odor-processing neural mechanisms with survival functions. Humans usually react positively to odors that reflect healthy natural stimuli, such as lavender, lemon, and pine; humans are disgusted by smells that accompany germs, such as smells of urine or vomitus. Health care environments must, at minimum, be free of smells that generate disgust or an urge to flee dangerous germs. Beyond that, it might be feasible to allow patients to choose among essential oils rather than imposing an odor that might trigger an individual fear reaction. 77 Harada et al. suggested that inhaled linalool (lavender extract) might be useful in premedicating surgical patients, especially patients who might have difficulty in tolerating other drugs. 78 Again, because of the strong and instantaneous effect that an odor can have, it would be prudent to discuss options with patients before exposing them to odors that may generate unfavorable reactions.
Nature-based interventions type II: natural sounds
Natural sounds: findings
Eight of eight Natural Sounds experiments reduced anxiety (100% success). Studies included patients of both genders, in different countries, for surgery, ob/gyn, cardio diagnosis, pain/trauma, and mechanical ventilation. Five successful studies provided nature sounds (e.g., birds chirping, or rain), either of the patients' choice or not. Another successful study allowed patients undergoing flexible bronchoscopy to hear taped sounds of nature, while they viewed portable murals of natural scenes. 79 Some authors of these studies proposed that patients were less anxious because they were distracted. A more likely explanation is the Biophilia Hypothesis presented below.
Nature-based interventions type III: natural visual stimuli
Natural visual stimuli: findings
Of seven Natural Visual Stimuli experiments, six reduced anxiety, in oncology and imaging settings (86% success). One study found that either real plants in the room or posters of plants lowered patient anxiety. 80 Some successful natural interventions depended on innovative technology, such as the “virtual window” projected on the wall for stem cell transplantation patients who could control the nature images. 81 The only study in this group producing null results had patients look at nature scenes through virtual reality goggles, possibly limiting patients' sense of control. 82 Like Music, plants and images of plants are recommended as an inexpensive and feasible intervention that can be easily implemented in health care settings. 83
Natural sounds and natural visual stimuli: mechanisms
It may be helpful to distract patients from the normal visual and auditory stimuli of the health care setting, but Distraction alone is not usually effective for reducing anxiety in adult patients. There is growing awareness that natural stimuli are powerful agents for calming the nervous system, and engineers and architects have become more interested in incorporating natural elements such as trees, fountains, and attractive landscapes into health care facilities. Some reviews call these interventions positive distraction; this term is used in Ulrich's Theory of Supportive Design for health care environments, 84 and it is often applied to research in pediatric settings. 85 A functional explanation grounded in evolutionary theory can be found in The Biophilia Hypothesis, which postulates that trees and bodies of water soothe humans because they signal the presence of plants and animals that sustain human life. 86 Humans may have evolved tendencies to be comforted by odors of pine and lavender because they signal lush settings where one might find shelter. Thus, more than being simple distractions, natural smells, sights, and sounds may organically generate an evolved sense of well-being that calms a patient's nervous system.
Distraction
Distraction: findings
In 25 experiments, a technological or instrumental intervention, not nature-based, usually described as Distraction, was used to alleviate anxiety in patients of both genders in several countries, with a success rate of 40%. Distraction was more likely to be successful for dentistry where Distraction devices were intentionally designed for use in the dental chair. Distraction interventions included headphones with white noise; stress balls (one of two stress ball studies lowered anxiety); video ping-pong; video word games; and visual distractions with or without virtual goggles. Most studies yielded null findings. Six studies involved having the patient view their own procedure (e.g., colposcopy) on a video monitor synchronously; in no case did this make the patient feel less anxious.
Distraction: mechanisms
Interestingly, although the pediatric literature suggests that Distraction may be very effective in calming children in situations such as receiving preschool immunizations, 87 adults seem to respond better to Music, Aromatherapy, or Nature-based Interventions than Distraction. Perhaps, adults have become accustomed to the comforts of nature. Also, unlike children, adults are typically fairly knowledgeable about what they are about to encounter in a health care setting, and any surprise, or attempt to change the subject might generate distrust. Adults may do better if they deal directly with their anxiety, by means of strategies such as CBT, with assistance from trusted providers.
Special garment
Special garment: findings
Four of seven Special Garment studies lowered patient anxiety (57% success). Only one experiment, an unsuccessful study with colonoscopy patients, included male participants. Typically, the Special Garment had been designed to replace a standard hospital gown or drape to allow female patients control over their privacy during invasive procedures such as a gynecological examination. In one study, one group of female patients wore a specially designed gown and another group wore that gown and listened to music; in both groups, anxiety was significantly lowered compared with controls. 88 In another study, one group of women wore a special garment and another group wore that garment and listened to nature sounds; again both groups showed lowered anxiety. 89 Interestingly, these two studies were conducted in Turkey, presumably with Moslem women who would likely have had strong cultural mores concerning physical modesty.
Special garment: mechanisms
Dallam 77 contended for patients who are victims of childhood abuse or adult sexual assault, disrobing, or undergoing invasive procedures may be re-traumatizing. Such patients might be assisted by being allowed to choose the gender of their health care providers, retain their own clothing, or have as much control over the procedure as possible. 90 Cultural mores are also an important consideration. Designing a garment that increases patient control over exposing one's body is a promising innovation that deserves more research.
Other interventions
Other Interventions (15 articles) present a mix of successful and unsuccessful outcomes. These represent cases in which fewer than five articles utilized a specific intervention (e.g., decision aids or patient warming or hydrotherapy); generalization of findings was not possible in such cases. These numbers are not discussed in detail.
Limitations and Future Research
Limitations regarding publication bias, sample sizes, and decisions regarding categorization are discussed in the SLR. There is little evidence of placebo controls (including true placebo, wait-list control, or attention control groups) in the research we reviewed. Because placebo effects come about, not because of the treatment itself, but, rather, because of the patient's belief that the treatment will have an effect, patients' beliefs and prior conditioning experiences are extremely important. 91 Substantial placebo effects have been demonstrated with regard to preventing migraine headaches 92 and pain. 93 In her 2012 systematic review of attempts to lower anxiety in cancer patients, Hedgpeth concluded that she could not confidently endorse findings from many randomized controlled trials because they lacked attention control groups. 94 Approximately half of the Acupuncture, Acupressure, and Aromatherapy studies included here had placebo controls that included sham treatments or infusers without an active scent, and, in nearly all cases, they reported significant reduction in patient anxiety. Future research would be improved with placebo controls appropriate to the particular experiments.
Conclusions
This review explored possible mechanisms underlying the following interventions for addressing patient anxiety: Music, Education, Relaxation, CBT, Massage, Distraction, Hypnosis, Acupuncture/Acupressure, Social Support, Aromatherapy, Natural Sounds, Natural Sights, Special Garment, and Other. Promising combinations of health care area and intervention are highlighted with shading in Tables 1 and 2, where an intervention has been tried at least four times with at least 70% success. The limited numbers of experiments, however, prohibit making recommendations with a high level of confidence.
Patient preferences repeatedly surfaced as key variables (see Music, Education, Relaxation, CBT, and Aromatherapy) predicting the success or failure of interventions. Ascertaining patient preference regarding the amount of education provided is particularly important. One study concluded, “Similar to the way in which patients have to be assessed before receiving treatment, patients' need for information should also be assessed before information is provided.”31(p. 672) Pre-procedural assessment can make patients less anxious, make procedures go more smoothly, and enhance patients' overall satisfaction. One useful assessment tool might be the Amsterdam Preoperative Anxiety and Information Scale, which uses six questions to assess anxiety and need for information. 95 Patient choice of clothing, artwork, and other environmental characteristics also emerged as important elements in many reviews.
A goal of this review is to provide a scientific framework within which specialists might benefit from the experimental work of others outside their discipline and also recognize gaps in the literature with an eye to planning future research. Research would benefit from streamlining terminology across disciplines. For example, these reviewers found it difficult to clarify findings when one report classified art as a distraction and another as a nature-based intervention. Because the underlying mechanisms are probably different, clarity is important.
The most striking finding may be the absence of research. In the tables here, 41 cells are blank—suggesting the absence of research exploring the effectiveness of a particular intervention within a medical specialty. Several specialties classified as “Other” have very little research represented here—including burn care and emergency department services. A principal goal of this review is that it will inspire health care providers to explore more interventions for alleviating patient anxiety, joining more fully with patients to achieve good health.
Footnotes
Authors' Contributions
C.C.W., J.A.T., and J.I.B. designed the project, and C.C.W. directed it. J.A.T. and J.I.B. executed the literature search, located abstracts and articles and assigned them for reading, and organized all references. J.A.T., J.I.B., C.C.W., and A.K. reviewed abstracts. C.C.W. did reliability training with A.K., R.E., B.R., E.B., and K.R. to prepare for reading and coding of articles and dissertations. Dissertations were coded by K.R. and E.B. Articles were read and coded by C.C.W., B.R., E.B., A.K., and R.E., with assistance from K.R., A.K., and K.D. coded included articles into health care specialty categories, with assistance from J.A.T. and J.I.B. R.E. and C.C.W. coded experiments into intervention categories. J.A.T., K.D., and C.C.W. designed figures and tables. C.C.W., J.A.T., K.D., R.E., B.R., and A.K. wrote the article, with input from the other authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.