
Abstract
Objectives:
This study describes the development and feasibility of Integrative Nutritional Counseling (INC), a Chinese medicine (CM)+biomedicine-based nutrition curriculum for Chinese Americans with type 2 diabetes. Although Chinese Americans often incorporate CM principles into their diet, scant research has explored how to integrate CM with biomedical nutrition standards in a culturally appropriate manner or if such a program could improve diabetes self-management.
Design:
This is a 1-month pre–post study design including three points of contact: baseline, in-person class, and 1-month follow-up.
Subjects:
Participants (n = 15) were Cantonese-speaking/reading Chinese Americans diagnosed with type 2 diabetes who had used some form of CM/medicinal foods in the last 12 months.
Interventions and Outcome Measures:
The INC program included baseline surveys and a CM intake interview conducted by a licensed acupuncturist. The acupuncturist generated a CM diagnosis, which was shared with the participant, and used this diagnosis to tailor brief nutrition education. To bolster this brief education, a bilingual registered dietitian provided a 2-h group education class in Cantonese to all participants, during which time participants also received a Chinese/English INC booklet. Participants completed surveys immediately after the class and at 1-month follow-up, with qualitative exit interviews.
Results:
Participants reported improved attitudes and dietary habits aligning directly with INC, and improvement in biomedically valued measures of type 2 diabetes, such as weight loss, and CM-valued measures of digestion/elimination and hot/cold feeling. Satisfaction with INC was high, but challenges included confusion with some INC information, structural barriers, and comorbidities.
Conclusions:
Chinese Americans with type 2 diabetes and interventionists found integrative nutrition approaches acceptable and feasible. Future research should examine INC with a larger population and explore optimal delivery of INC given reported challenges.
Introduction
Type 2
The idea of holistic equilibrium and balance underscores CM theories (for more information, see Kaptchuk 16 ) that have existed for millennia. However, the form of CM that is widely used today traces its roots to the 1940s when Mao Zedong codified certain parts of CM, notably herbal medicine and acupuncture. 17,18 Named “Traditional Chinese Medicine,” this decades-old version of CM is the basis for licensed forms of CM used globally. However, in unlicensed venues and lay usage, CM also includes practices such as tuina (massage), bone setting, acupressure, qigong, t'ai qi, and dietary therapy/nutrition. Although not always included in formal CM training, many Chinese American laypeople and licensed practitioners continue to incorporate dietary therapies in their practices to improve overall health equilibrium within the person as a whole, bringing balance in a holistic way to the person's interconnected systems. 19
Despite the fact that Chinese Americans use CIH at higher rates than the general population in the United States, 13 and that Chinese Americans are specifically interested in integrating CM and biomedicine for T2DM, 20 there are few biomedically tested guidelines to support such integration. Integrative Nutritional Counseling (INC)—the booklet and curriculum developed and tested in this study—was designed to address this gap with input from four stakeholder groups: licensed CM experts, unlicensed and lay CM experts, biomedical experts (e.g., primary care providers, nurses, dietitians), and Chinese American patients with T2DM. Development was guided by the PEN-3 Model, which makes culture explicit in designing health promotion materials. 21 Used in a variety of cultural contexts in Africa, the Middle East, the Caribbean, and among indigenous people and people of color in the United States, PEN-3 seeks and acknowledges individual and community beliefs and practices that may already be fostering positive health even if those practices are not typically recognized as health care. As such, both lay CM experts and Chinese American patients were included—to incorporate their knowledge and practice of dietary intake to support optimal health.
Despite growing interest in testing the safety and efficacy of Chinese medicinal herbs and foods for treating diabetes, 22 –24 no previous research has integrated CM principles and nutrition for diabetes. As a culturally sensitive integrative behavioral intervention for Chinese Americans with T2DM, INC incorporates biomedically based nutrition recommendations alongside Chinese medicinal food concepts. Biomedically-based nutrition recommendations commonly use the MyPlate method that suggests meals of ∼50% vegetables, ∼25% proteins, and ≤25% carbohydrates. 25 –27 From a Chinese nutritional perspective, foods can be ingested that move a person closer to holistic equilibrium because they contain energetic properties not recognized in biomedicine. In this study, these basic food properties were presented so patients could choose the most suitable vegetables, proteins, or carbohydrates for their Chinese medical condition while simultaneously staying within the constraints of the biomedically suggested ration of ∼50% vegetables, ∼25% proteins, and ≤25% carbohydrates.
This study used the framework from Bowen et al. 28 for testing the feasibility of INC among Chinese Americans with TD2M. Specifically, the authors assessed acceptability (participants' reactions to the intervention), demand (use of the intervention), and limited efficacy (testing in a convenience sample or with limited numbers or shorter time frame). 28
Materials and Methods
Intervention
The INC curriculum integrating biomedical nutrition concepts for T2DM with Chinese medicinal foods for T2DM was developed through iterative rounds of decision-making by the research team (Fig. 1). Team members had expertise working in Chinese and Chinese American communities as an internal medicine physician, a licensed acupuncturist/medical anthropologist, a registered dietitian, a health communication scholar, and a Cantonese linguist. The final rendition of INC included a 44-page full-color magazine-style booklet printed in Chinese traditional characters and English, large posters of materials from the booklet, and instructions for how to teach INC in a 2-h group setting.

Iterative INC guide and curriculum development. INC, Integrative Nutritional Counseling.
INC is designed to be culturally sensitive in two important ways. On a basic level, INC uses Chinese and English wording and including regularly available Chinese foods as examples and in pictures. More importantly, INC is culturally appropriate on a deeper level.
29
First, it includes culturally specific practical tips, such as categorizing dumplings as both protein and carbohydrate. Second, it tailors biomedically sound diet recommendations to three CM imbalance conditions: heat, dampness with heat, and cold/weakness (Fig. 2), each with corresponding INC food recommendations to address those imbalances (clear heat, clear heat/rid damp, nourish and warm). For example, a person with a heat condition is encouraged to eat more vegetables considered to have a cooling therapeutic profile within the CM paradigm, such as cucumbers or lettuce. By eating cooling vegetables rather than warming vegetables, a person using INC can control both their carbohydrate intake (biomedical perspective) and improve their equilibrium (CM perspective). INC has oversimplified professional CM individualized diagnoses (e.g., limiting to three basic diagnoses) and their corresponding treatments so that patients without extensive CM professional knowledge can still use it as a self-management tool (Fig. 3). To download INC, go to

Conversion of Chinese medicine diagnoses to INC assignment. Presented are three sample Chinese medicine diagnoses as written by the Chinese medicine practitioner and then as translated into the corresponding INC assignment. Diagnoses of dampness typically led to a yellow INC assignment. Diagnoses of heat typically led to blue or sometimes yellow INC assignments. Diagnoses of deficiency typically led to red INC assignments.
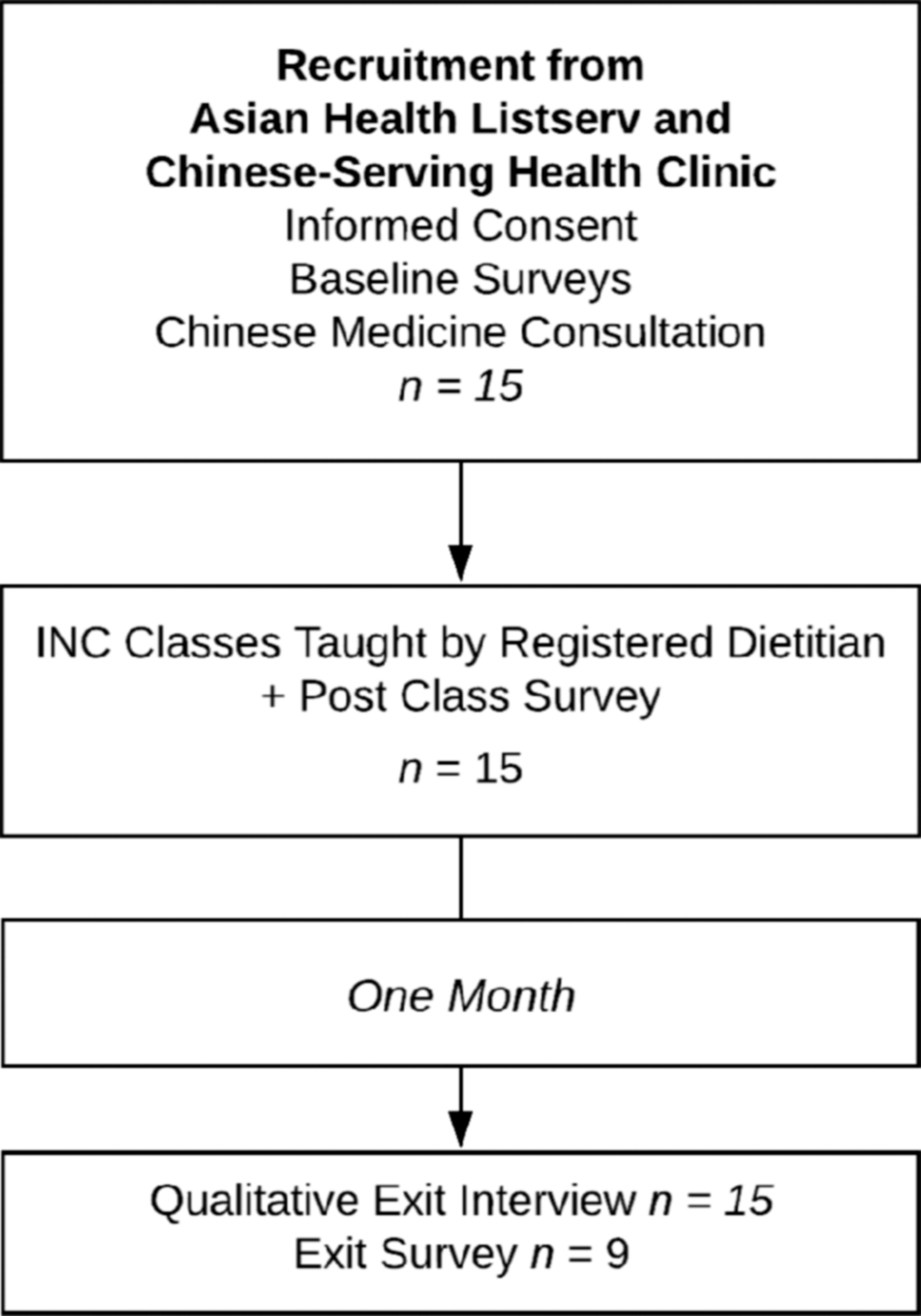
Flow diagram of study participants.
Research design
The authors chose a convergent design to triangulate data from a small sample. Open- and close-ended questions addressed acceptability, demand, and limited efficacy. This is a 1-month pre–post study design including three points of participant contact: baseline, in-person class, and 4-week follow-up. The baseline study visit included informed consent, survey administration, and a 30-min interview in Cantonese with a Cantonese bilingual licensed acupuncturist. The Chinese American acupuncturist used CM diagnostic techniques, including a clinical interview for symptoms and a tongue and pulse examination. The clinical interview was standardized using a CM-specific symptoms checklist adapted from Beinfield and Korngold's 30 organ-specific symptoms checklist (Appendix A1). Unlike a biomedical diagnosis of T2DM, a CM diagnosis is dynamic and depends on the patient's current holistic situation.
Following their diagnostic interview with the acupuncturist, participants attended a 2-h, small-group course taught in Cantonese by a Chinese American bilingual diabetes educator/registered dietitian with more than a decade of experience teaching traditional T2DM nutrition education classes to Chinese Americans. This class, however, was based on the INC curriculum. During the class, participants received the INC booklet and their individualized CM diagnoses, which placed them into one of three INC assignments (clear heat, clear heat/rid damp, warm). Participants completed surveys immediately following the class. Four weeks later, participants completed a follow-up interview. University of California San Francisco and University of San Francisco Institutional Review Boards approved the study.
Participants and setting
In San Francisco, where this research took place, Chinese Americans comprise 18.3% of the population, 31 and 62.9% are limited English proficient. 31 Study participants were a convenience sample targeting monolingual Chinese Americans recruited through physician recommendation at a predominantly Cantonese-serving public health clinic, passive Chinese-language advertising at a public safety net hospital, and an e-mail sent to an Asian health-oriented listserv. Recruitment materials described a research study including an educational class integrating Chinese and Western medicine nutrition for T2DM. Eligibility criteria included: (1) T2DM diagnosis; (2) ability to read Chinese/speak Cantonese; and (3) use of CM or CM diet principles within the previous 12 months. Participants chose one of three classes conducted in 2014–2015 at a university hospital conference room (n = 2) or the Cantonese-serving clinic (n = 1) and received a $30 gift card as an incentive. The recruitment period and intervention pilot were determined by budget and time constraints.
Measures
The baseline participant survey included questions about sociodemographics (e.g., age, sex, education, nativity), self-reported health status, and diabetes care. It also contained measures of acculturation (more Asian, bicultural, more Western) using the Suinn–Lew Asian Self-Identity Acculturation Scale 32 and preferences for Chinese or Western medicine (Chinese and Western Medical Beliefs Scale). 33,34
At baseline and follow-up 4 weeks after the intervention, surveys assessed dietary intake with four questions about the quantity of vegetables, fruit, and white and brown rice consumed in the previous day. These surveys also included measures of diabetes self-care (Summary of Diabetes Self-Care Activities Measure, 35 which includes an item querying how many of the last 7 days the respondent followed a healthful eating plan), diabetes distress (two-item Diabetes Distress Scale short form), 11 and self-efficacy (modified five-item Heisler's Self-Efficacy Scale, assessing degree of difficulty with T2DM-related self-care activities). 36
To measure satisfaction with INC immediately following the class, participants rated 14 statements about attitudes, beliefs, anticipated behavior, barriers, and communication on a 5-point Likert scale.
Qualitative interviews with stakeholders used a semi-structured interview guide developed by the research team to address key dimensions of feasibility and acceptability. Interviews with the acupuncturist and registered dietitian focused on their experiences delivering INC. Interviews with participants were conducted 4 weeks after the INC class. These interviews were audio-recorded, lasted ∼30 min in duration, and addressed health changes, current diet, usage of the INC guide and assignment, and sharing INC with others.
Data analysis
For descriptive analysis, the authors calculated means for continuous variables and proportions for categorical measures at baseline and after the intervention. Bilingual Cantonese authors (D.C., S.H., and Q.R.) conducted, transcribed, and translated the interviews, which were checked by another author (G.L.). Chinese American authors conducted a thematic analysis 37 (E.Y.H., G.L., M.T.C., H.L.-C., S.H., Q.R.) using inductive and deductive approaches. The authors iteratively conducted open coding and constant comparison by writing analytical memos 38 and then sorting codes into larger themes, coming to consensus as a team. Qualitative data analysis software, ATLAS.ti 8.3.0 (Berlin), was used to organize data and locate examples related to feasibility and acceptability of INC.
Results
Participants
Fifteen participants enrolled in and completed the study (Fig. 3). Most were aged between 61 and 70 years (53%, n = 8) and were female (67%, n = 10) (Table 1). All were immigrants with most (87%, n = 13) residing in the United States for more than 10 years, with fair or poor self-reported health (71%, n = 10) and taking medication for T2DM (93%, n = 14). Most (87%, n = 13) reported that they knew what a diabetic diet was.
Characteristics of Participants (n = 15)
Based on 14 respondents, missing n = 1.
Acceptability: Chinese American participants
Surveys conducted immediately after the INC class indicated high satisfaction and intention to act. All participants agreed or strongly agreed with the statements “I learned something new today about diabetes and diet,” “I feel confident that I will use the things I learned today,” and “In my next meal, I plan to use the things I learned today” (Table 2).
Average Rating of Intervention (n = 15)
Mean score across all participants on a 5-point Likert scale from strongly disagree (1) to strongly agree (5).
SD, standard deviation.
Interviews conducted 4 weeks later demonstrated continued satisfaction with INC (Table 3). Participants appreciated cultural aspects of INC including the use of Chinese language, numerous color pictures of vegetables, and typically eaten Chinese foods. A majority (8/15) actively used the INC booklet during the last 4 weeks, reading or referring to the book when making dietary choices. Participants appreciated INC as a unified system, made by trusted experts, that could be used while shopping. Although few participants shared the INC materials with their doctors, 11 of 15 (73.3%) reported that they had shared either the INC materials or something they learned from INC with friends or family members.
Patient Acceptability Exemplary Quotes
Acceptability: provider delivery of INC
The acupuncturist who met with all the participants reported that the symptom checklist was useful in guiding patient conversations. Because the visit was similar to what she would have done in a usual CM intake interview, she was quickly able to generate a CM diagnosis. When converting this individualized diagnosis into one of the three INC assignments (clear heat, clear heat/rid damp, warm), it became apparent that most participants (n = 14/15) needed both a primary and secondary assignment (Fig. 2). This realization generated a change in the protocol in which participants were instructed to focus mainly on nutrition education for their primary assignment, but that dietary choices appropriate for their secondary assignment could be utilized as well.
The registered dietitian was able to successfully deliver INC after 2 h of training with the research team and reported appreciation of the high quality of the full-color INC guide with large font and many pictures of Chinese foods. However, she reported an inability to answer some questions specific to CM that she was posed during the class and suggested future classes be co-taught with a CM provider who could answer those questions.
Demand: participant successes and challenges using INC
Dietary successes
The 4-week follow-up survey was administered to 9 of the original 15 study participants. No changes were observed for most survey measures (Table 4). In contrast, in qualitative interviews of 15 participants, all but 2 participants (86.7%) reported making a behavior change including eating less oil/fried foods, desserts, or carbohydrates, and eating more vegetables, or performing more physical activity. Twelve (80%) participants either reduced white rice consumption or increased brown rice consumption. Twelve (80%) participants reported that they tried to eat more vegetables and/or tried to conform to the MyPlate proportions. Participants also discussed dietary changes based on the INC suggestions, including suggested carbohydrate to vegetable and protein proportions, mixing white and brown rice, increasing physical activity, and eating fewer desserts (Table 5).
Intervention Outcome Measures, Baseline Versus Postintervention (n = 9)
Lower score is more optimal.
CI, confidence interval.
Demand: Participant Successes and Challenges Using Integrative Nutritional Counseling Exemplary Quotes
INC, Integrative Nutritional Counseling.
Dietary challenges
Some participants reported increased dietary intake of recommended foods. However, close reading of the text revealed that one third (5/15) mentioned increasing “fruits and vegetables” together as being part of the overall practice of “eating healthier,” despite emphasis in the guide that fruits raise blood glucose levels. Participants also reported challenges avoiding foods they especially liked, such as pineapple, taro, and spring rolls, or not enjoying some suggested foods such as bitter melon, collard greens, and brown rice (Table 5).
INC assignment successes and challenges
At 1-month follow-up, some participants forgot their INC assignment, despite its being reinforced in the class with multiple modalities (e.g., colored stickers on take-home materials). Other participants disagreed with their INC assignment. In exit interviews, a majority of participants (8/15) were able to remember both their primary and secondary INC assignment, 5 remembered only one correctly, and 2 could not remember at least one assigned assignment. Two people actively questioned or disagreed with their assignment, although they could remember it (Table 5).
Structural challenges and comorbidities
Participants reported a number of comorbidities, such as high cholesterol, that also motivated a desire to alter dietary intake. Conversely, some participants reported structural problems such as missing teeth (and needing soft foods) or food insecurity that made dietary changes difficult to follow (Table 5).
Patient-reported outcome measures: limited-efficacy testing
Exit interviews asked participants to report on any changes they noticed to their T2DM since beginning the study. Participants reported various signs that INC was leading to T2DM improvement, with assessments stemming from both biomedical and CM standards. Although HbA1C was not measured nor explicitly asked about in interviews, seven participants (46.7%) attributed reductions in their blood glucose levels to INC-related changes. Similarly, although participants were not asked specifically about weight, some reported losing weight (Table 6).
Patient-Reported Outcome Measures Exemplary Quotes
Participants also volunteered symptom improvement related to their CM assignments, despite this not being explicitly addressed in the interview questions. In response to the question, “has anything improved,” Yiru explained that after following the warming diet, her bowel movements were more solid (Table 6). Two additional participants mentioned digestive improvements as signs that following INC was working. For other participants (such as Yue), knowing the INC assignment allowed for dietary changes that addressed the body's feeling of temperature and psychological state (Table 6). Like digestion, having warm/cold extremities is often considered a sign that one's body is imbalanced according to CM.
Discussion
This mixed-methods study of a 2-h, in-person course integrating biomedical nutrition with CM shows promise for positive attitude and behavior change among Chinese Americans with bicultural values. Four weeks after the INC class, participants qualitatively reported positive changes in dietary intake and health outcomes, including better blood glucose measurements, better digestion, better hot/cold balance, decreased weight, and more positive mood. Provider acceptability was high, with both the dietitian and acupuncturist delivering the intervention with minimal training. Future work should examine INC implementation by a team that includes both a diabetes educator and CM practitioner, solidifying the integration between the two forms of medicine. This model would include, for example, both types of providers being present for the group class and for the diagnostic session.
INC was found to respect traditional culture, while also promoting evidence-based biomedical guidance of T2DM management. Regarding demand, 28 participants generally were accepting of mixing biomedical nutrition recommendations with CM recommendations, as evidenced by the numerous participants who shared the INC guidebook with friends and family. When participants used their INC assignments, they reported improvement using a vocabulary of hot/cold balance, confirming previous studies indicating the importance of and desire for guidance around addressing hot/cold balance in the context of T2DM management. 14 The goal of the INC curriculum was to provide a biomedically sound and culturally responsive education program that patients would use to promote dietary behavior change. Thus, a primary focus of the INC curriculum was adherence to CM principles. However, exit interviews illustrated that the actual INC assignments may not have been the most salient new information for participants. Instead, participants equally discussed other behaviors such as increasing exercise and vegetable/fruit intake, trying new vegetables, or avoiding sweets. (Notably, Chinese Americans with T2DM may struggle to identify fruits as carbohydrates because of a tendency to eat fruits over other sweet desserts. 39 ) This observation suggests that the CM diagnosis was not the most resonant lesson, which may be a reflection of a general lack of other diabetes education in this population or an increased responsiveness to education messages when they are framed in a familiar cultural context. Future research should explore whether INC assignments are more accessible to Chinese Americans with foundational knowledge of hot/cold balance and to what extent patients actually engage with that portion of the program.
After only 1 month, patients identified their behavior changes as positively affecting their blood glucose measurements. From a CM standpoint, imbalances of hot/cold and dampness are often manifest by problems with overall mood/energy, physical sensations of hot/cold, and changes to digestion. CM providers also typically ask about one's digestion in diagnostic questioning. Thus, it is not surprising that participants paid attention to and reported on their digestion as a way of tracking overall improvement in health. In future work, digestive symptoms may offer an opportunity for self-assessment of positive dietary change.
Overall, based on limited-efficacy testing, 28 participants were highly satisfied with the INC class and the diagnosis provided by the acupuncturist, but 1 month may not be adequate to detect clinically measurable changes in important outcomes. Future studies should increase the numbers of participants and time between intervention and exit testing and examine INC as a well-integrated component of clinical care, rather than as stand-alone T2DM self-management education.
Conclusions
The authors created and pilot-tested a Chinese-language, integrative nutrition guide and curriculum to elicit behavior change toward optimal T2DM management. Preliminary findings suggest that patients were highly satisfied, incorporated nutrition suggestions, and recommended the guide to family and friends. As a brief culturally relevant intervention, INC could be incorporated into existing T2DM self-management education if participants were able to obtain a CM diagnosis soon before the onset of the education; this structural barrier could be addressed by better integration between CM providers and biomedical providers. The study findings are limited. Small sample size does not allow us to determine whether observed behavioral changes were statistically significant. Without a control group or randomized participation, it is not clear whether the intervention was causally related to positive changes observed. Follow-up surveys were only collected from a subset of participants. Despite the limitations of this study, INC shows promise as a more culturally appropriate approach to supporting behavior change among Chinese Americans with T2DM than simply translating existing T2DM nutrition education. Future studies are needed to assess the impact of INC on patient-centered and clinically relevant outcomes, including attitudes, health behaviors, dietary adherence, weight, and glycemic control. INC may address an important unmet need for culturally relevant approaches to providing support for T2DM self-management among Chinese Americans.
Footnotes
Authors' Contributions
E.Y.H., G.L., and S.H.: project conceptualization, data collection, data analysis, writing, reviewing/approval of article. M.T.C.: data analysis, writing, reviewing/approval of article. D.C. and H.-L.C.: data collection, data analysis, writing, reviewing/approval of article. E.Y.H. and S.P.: project conceptualization, data analysis, reviewing/approval of article. Q.R.: data collection, writing reviewing/approval of article. H.K.S.: project conceptualization, data collection, writing, reviewing/approval of article.
Acknowledgments
The authors wish to thank the research participants for generously sharing their time and their stories with us, Anita Huang, LAc, and Jing Liu, RD, for delivering INC, and University of California San Francisco's Asian Health Institute and University of San Francisco's Faculty Development Fund for funding this project.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was also supported by the National Center for Complementary and Integrative Health (K01AT006545). The funding sources had no role or involvement in the design and conduct of the study; the collection, management, analysis, or interpretation of the data; or in the preparation, review, or approval of the article. Contents are solely the responsibility of the authors and do not necessarily represent the official views of the funders.
Appendix
Chinese Medicine Self-Assessment Health Profile
| INSTRUCTIONS: Mark the symptoms you have experienced during the last 6 months. Circle those that have been most troublesome. | |
| Heat | |
| ___ fever |
___ yellow, green, or foul smelling discharge |
| Deficient moisture | |
| ___ parched, thirsty |
___ constipation |
| Cold | |
| ___ lack of thirst |
___ edema |
| Dampness | |
| ___ dizziness or fullness in head |
___ sticky or greasy stool |
| Damp heat | |
| ___ dryness or thirst—no desire or ability to drink |
___ loose or sticky stool |
| Deficient qi | |
| ___ weak, lethargic, weary |
___ perspires easily with exertion |
| Diminished essence | |
| ___ profound weakness |
___ loosening or loss of teeth |
| Spleen network | |
| ___ tender muscles |
___ overwhelmed by details, upset by changes |
| Lung network | |
| ___ weakness of chest |
___ wheezing from fatigue or exertion |
| Kidney network | |
| ___ puffiness around eyes |
___ lack of stamina and endurance |
| Spleen–Kidney disharmony | |
| ___ slow digestion, sluggish intestines |
___ easily chilled in back, belly, legs or arms |