
Abstract
Background:
Meditation-Based Lifestyle Modification (MBLM) is a new mind–body intervention that is based on classical yoga; it implements virtue-based ethical living, physical yoga, and meditation in a therapeutic context. This qualitative study aimed at understanding better how depressive patients who received MBLM as a treatment experience intra- and interpersonal outcomes of their practice.
Methods:
In a larger randomized controlled trial of MBLM in depressive outpatients, a subsample (n = 12) completed in-depth interviews. To determine short-term and long-term effects, cohorts were interviewed at two different times after intervention onset (T 1 = 8 weeks; T 2 = 6 months). Verbatim interview transcripts were analyzed by using thematic analysis.
Results:
Three themes emerged in the interviews: (1) Reappraisal of past and present life patterns, leading to a reflection on one's own values; (2) Serenity, attained by states of calm, growing acceptance, and the ability to set boundaries; and (3) Mindful living as expressed by increased self-awareness, being more present, and conscious interactions. The ethical component of MBLM was identified as a key factor in individual empowerment and appreciation of one's own strengths. Systematic changes in the importance of reported themes after 6 months (T 2) reflected the sustained effects of the intervention.
Conclusions:
The findings speak clearly for the benefits of MBLM in the treatment of depression. In particular, the explicit therapeutic implementation of virtue-based ethics offers a valuable addition to previous yoga and meditation programs. Clinical
Introduction
Recent research has shown the positive impact of yoga in the treatment of different mental health conditions. 1,2 In particular, the treatment of depression has been investigated through a larger amount of quantitative and qualitative analyses in different populations. 3,4 Commonly, yoga practices in mental health care focus on physical exercises, breathing techniques, and, to some extent, meditation techniques. 5 These primarily body-oriented techniques contribute to physiological and psychological pathways in alleviating depression: At the physiological level, they likely improve mood based on physiological mechanisms that are related to stress-reducing and anti-inflammatory modulations of the autonomic nervous system and neuroendocrine circuits, 6 presumably mediated by epigenetic mechanisms. 7 At the psychological level, body-oriented yoga has positive effects on body awareness and mindfulness, and it leads to feelings of connectedness, reappraisal, and improved coping. 8,9 However, body-oriented aspects represent only part of yoga in the traditional understanding of it as a spiritual practice and path to self-realization. 10 Our work extends research to more traditional—ethical, spiritual, and meditative—aspects of yoga to unveil potentials of yoga practice that have not yet been tapped in mental health care.
What is traditional yoga about? The most authoritative and seminal text answering this question is the Yoga Sutras by Patanjali, in which preexisting traditions have been collated and systemized. 11(p. xxxiii) Yoga is defined as a primarily meditative practice, by which the mind is stilled to achieve self-realization. The term “self” refers here to “pure consciousness” or innermost self, loosely related to the soul in Western Greco-Abrahamic traditions.11(p. xvii) From a psychological perspective, the humanistic concept of self-actualization is, to some extent, comparable to that of self-realization in the eastern traditions. 12 Yoga can be interpreted as a developmental process that facilitates self-actualization, which, in Maslow's hierarchy of needs, 13 describes the attainment of one's full potential as a human being—a goal that is highly relevant in the psychotherapy of depression. 14 In fact, in yoga psychology, the practitioner ultimately even transcends fulfillment on a personality level, which has been mentioned by Maslow in his later thoughts as a final motivational step beyond self-actualization. 15
In addition to yoga postures and breathing exercises (asana and pranayama), the yoga sutras name further limbs of yoga's 8-fold path to self-realization: inter- and intrapersonal virtue-based ethics (yama and niyama) and four stages of meditative practice (pratyahara, dharana, dhyana, and samadhi). From a perspective of positive psychology, moral virtues and character strengths have been widely recognized and their contribution in depression treatment is well founded. 16 Regarding meditation, recent meta-syntheses of randomized controlled trials unanimously concede that meditation has substantial beneficial effects on depressive symptoms in clinical populations. 17,18
Meditation-Based Lifestyle Modification (MBLM) is a new therapy developed for mental health care, 19 in which all eight aspects of classical yoga have been integrated and that has been shown to be feasible in the treatment of patients with mild-to-moderate depression. 20 The MBLM goes beyond the third wave of behavioral therapy, 21 seeing itself as representative of more recent developments (second generation mindfulness-based interventions). 22 These focus on human virtues, individual strengths, and resilience in the sense of positive psychology; include the body in the individual process of becoming conscious (embodiment); and are overtly spiritual (but conveyed in a strictly non-dogmatic and non-sectarian way).
Mixed methods have proven helpful in understanding complex mind–body interventions such as MBLM. Qualitative approaches aid comprehensive interpretation of intangible experiential information, which is particularly relevant to mind–body practices. 23 A recent synthesis of 11 qualitative studies explored the lived experience of yoga practice for people with depression, posttraumatic stress disorder, and anxiety disorders. 4 In these studies, the interventions were usually physical yoga exercises with no explicit focus on ethical and meditative aspects. To evaluate the impact of these ethical and medicative components, we present qualitative data generated through in-depth interviews of psychiatric outpatients with mild-to-moderate depressive disorder who participated in the MBLM program.
The aim of this study was to better understand how MBLM practitioners with depression perceive intra- and interpersonal outcomes of their practice (including subjective assessments of how well it worked), and to discuss these in the light of the existing qualitative findings.
Methods
Design and setting
This qualitative study was part of a larger randomized controlled study, Meditation-Based Lifestyle Modification in Depression (MBLM-D), which was conducted from August 2018 to June 2020. The study was registered at
Participants were assessed quantitatively at three points: at baseline, before the intervention (T0); post-test, immediately after the intervention (T1); and during follow-up, 4 months after the intervention had ended (T2). At the first visit (T0), within 1 week before the MBLM program started, participants provided informed consent and completed a baseline survey, including sociodemographic and psychosocial questionnaires. The participants (N = 81) were randomized into three treatment groups: (1) MBLM program, (2) tailored psychiatric–psychotherapeutic therapy, and (3) drug continuation therapy (Fig. 1). The intervention lasted 8 weeks.
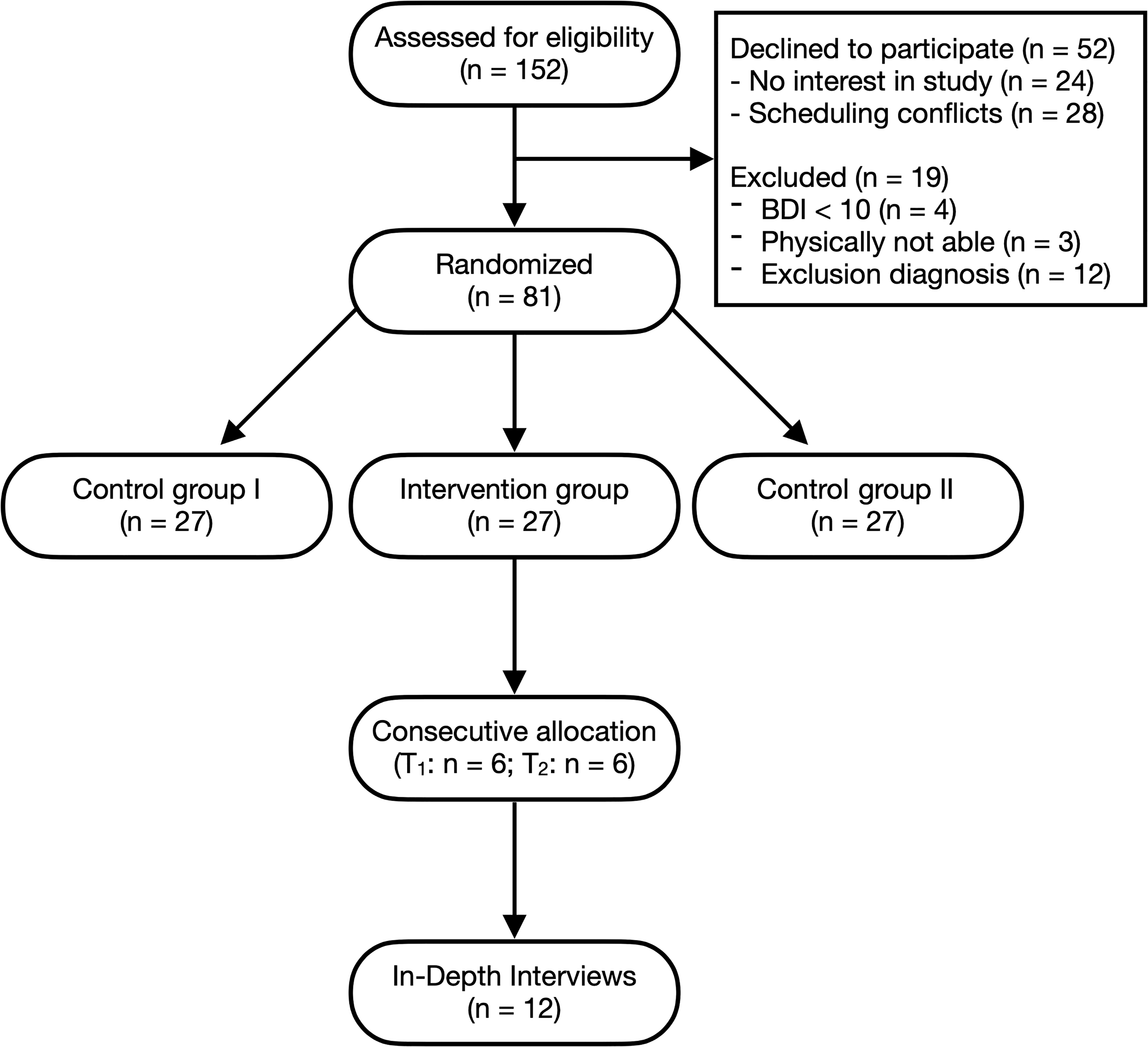
Participant flow. BDI, Beck Depression Inventory.
For this qualitative study, we interviewed participants either post-test (T1) or at follow-up (T2), to identify any differences between short-term and long-term effects of the intervention. We interviewed only participants from the MBLM program, as we were interested in their subjective theories on the efficacy and working mechanisms of this specific treatment. Participants were contacted and interviewed consecutively after the first patient in the MBLM arm reached the 6-month follow-up (T2).
Sample
A total of 12 patients (11 = female; 1 = male) aged 30–69 years (mean = 54; SD = 11.23) were interviewed for the present qualitative analysis. Patients were diagnosed with depression according to ICD-10 criteria (mild = 2; moderate = 10). Nine patients (75%) had recurrent episodes of depression (mean number of episodes = 2.58; SD = 2.47), and three of these patients had psychiatric comorbidities (two patients with somatoform disorders, one patient with posttraumatic stress disorder). All patients had been diagnosed with depression for at least 1 year (mean = 9.67, SD = 10.65) and had received psychotherapy in the past (mean = 33.5 months; SD = 30.82). Six patients received regular antidepressant medication, and three of those also received neuroleptic medication. Seven patients reported irregular yoga practice in the past, and none of the patients reported practicing meditation in the past.
Intervention
The MBLM program 19 consists of eight consecutive, weekly group sessions of 180 min each, and 45 min of recommended, daily home practice. Each group session (as well as training at home) includes three domains of practice, based on the 8-fold path of classical yoga: ethical living, healthy lifestyle, and mantra meditation. In the first part, ethical living, the therapists present the major aspects of yoga practice regarding virtue-based ethics, including constraints (nonviolence, truthfulness, non-stealing, non-excess, and non-greed) and spiritual observances (purity, contentment, and transcendence). The topics change each week and the approach is educational and psychotherapeutic, with group discussion, considering participants' individual processes, and deepening them through mindful living exercises for home practice. During the second part, healthy lifestyle, the participants learn breathing exercises and gentle yoga postures that are suitable for people with depression and anxiety. 25,26 The therapist demonstrates all exercises and supports the participants by giving corrections if necessary. Participants also receive individualized healthy lifestyle advice based on basic Ayurvedic recommendations before the course. The third part of each group session is a mantra meditation period where participants silently recite a mantra, which they have chosen themselves from a list and learned to apply in an introductory session before the course.
Data collection
We created a semi-structured interview guideline, including topics that focused on subjectively perceived intra- and interpersonal outcomes of the participant's MBLM practice. The topics were inspired by the results of a previous feasibility study 20 and consensually developed by the research team. They referred to general perceptions about program-related changes in everyday life, depressive symptoms, and spirituality (Table 1). The topics were addressed in no specific order, but adapted to the individual course of the conversation, to create the most natural dialogue possible. Finally, the interviewees were offered space for any additional topics. Interviews typically lasted for about 45 min, were audiotaped, and were then transcribed.
Interview Guidelines
The opening questions were not necessarily asked verbatim or in that particular order. It was more important to address the topic of each question in general, following the natural flow of conversation as directed by the interviewees.
Data analysis plan
Data analysis was subjected to thematic analysis to extract overarching themes, guided by Braun and Clarke's methodology. 27 The approach consisted of six steps: (1) transcribing, multiple reading, and writing down of comments to familiarize oneself with the data; (2) generating initial codes through systematic identification of text passages (an inductive approach was used, since the aim was not to test a theoretical framework, but to describe the data comprehensively; (3) condensing by classifying codes into potential higher-level themes and collating all relevant data; (4) aligning the themes with individual coded text passages of an interview and then with the entire data set (in this phase, a thematic map was created to illustrate connections, groupings, and hierarchies); (5) naming and defining the themes; and (6) writing the analysis report, enriched with excerpts from the interviews.
The software f4analyse (version 2.5.4.0) was used to manage and analyze the data. JV and JG conducted the interviews and engaged in a recursive process of consensual coding to increase intercoder reliability. JV analyzed the first n = 6 (three conducted at T1 and three at T2) interviews and created an initial thematic map. Based on the code system of these interviews, HB analyzed the remaining n = 6 (three conducted at T1 and three at T2) interviews and created a final thematic map of the entire data set. In addition, JG checked the coding process with the first n = 6 interviews by recursive consensual coding to increase the intercoder reliability. Researchers experienced in qualitative data analysis (K.M. and P.S.) supervised and evaluated the process.
Results
Thematic analysis of the interviews with participants in the MBLM program revealed three key themes: (1) reappraisal, (2) serenity (3), and mindful living. All themes were further differentiated into subthemes (Fig. 2): (1.1) Recognizing past cognitive and behavioral patterns; (1.2) Recognizing new opportunities; (1.3) New values; (2.1) Experiencing calm; (2.2) Recognizing and setting boundaries; (2.3) Acceptance; (3.1) Self-awareness; (3.2) Being present; (3.3) Conscious interactions. Each theme is presented in turn next, and the frequencies with which they were mentioned are shown in Figure 2. At the times when the participants were interviewed, no different themes emerged at T2 compared with T1, but quantitative differences were evident (see Result section). In addition to the quotes in the results section, Table 2 contains statements from the participants to support each summary.
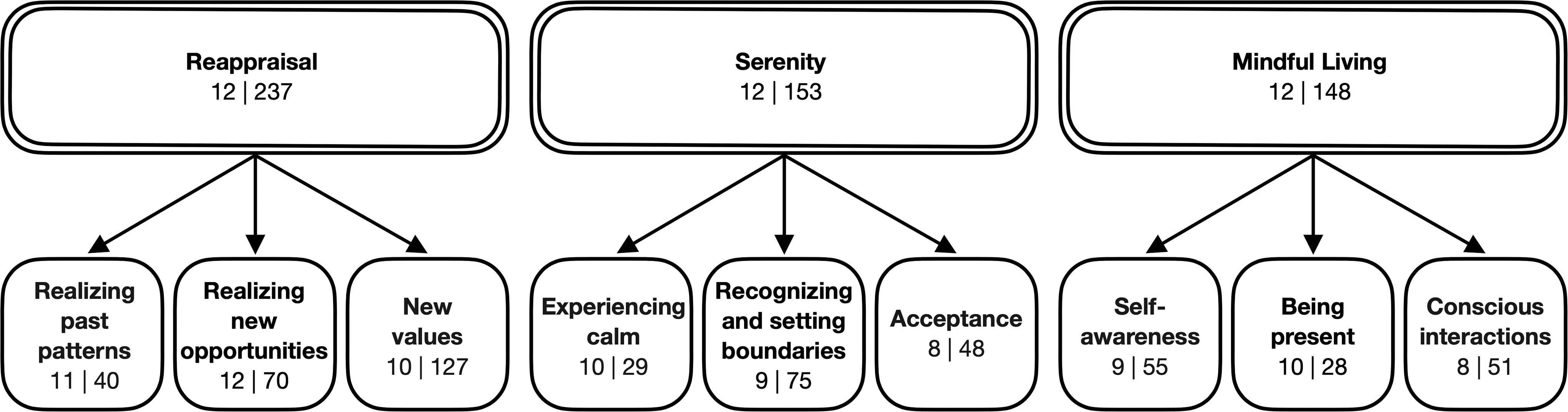
Themes (upper row) and corresponding subthemes (lower row). For each entry, two numbers n | s are given: n denotes the number of participants talking about that theme, and s denotes the total number of statements that have been assigned to that particular (sub)theme.
Example Statements
Reappraisal
Reappraisal was identified as the most dominant theme. All participants reported that the course stimulated them to engage with their lives, more precisely with ethical living, although this was more marked at T2. In doing so, they considered both their past and present lifestyles in terms of ethical living and reported on new opportunities and values that emerged for them.
“I have become aware of so many things about ethical living; I never paid attention to how important it is before.” (56 years old, T2)
Recognizing past cognitive and behavioral patterns
During the MBLM course, participants became aware of the basic behaviors and experiences that had caused suffering or difficulties in their previous lives. They mentioned low self-esteem, lack of self-congruence, feeling controlled by others, and aggressiveness toward others.
“My self-esteem and self-confidence had hit rock bottom. And I really had to face up to that here” (63 years old, T2)
The process of confronting one's own past was repeatedly experienced as painful: “First of all, THINKING about the fact that you did totally messed things up, that really did hurt a bit.” (53 years old, T2)
Instead of avoiding these uncomfortable issues, participants were intrinsically motivated to embrace this challenge to reflect beyond the 8 weeks of the course: “I also want to understand a lot of things and also, because of these questions I want to work on, […] where I tell myself that I can really calmly and consciously look at it, and think about it.” (59 years old, T1)
Participants continued to reflect in this way, as is confirmed by their statements at T2. Most of them stated that since taking part in the MBLM course they had become more aware not only of their own actions, but also those of the people around them, and would make decisions based on this, as one participant vividly expressed: “That wouldn't have occurred to me before, I used to go on holiday without thinking about it, but when I'm flying somewhere now, I wouldn't take this all-inclusive [last time we went] we sat there and said: ‘We don't even know what you need it for. We don't want to go on vacation and just eat our fill all day, do we?’ […] I wouldn't have thought like that last year even IN A DREAM and sometimes I think: ‘You've heard that here somehow.’” (48 years old, T2)
The only man and oldest participant in the sample pointed out that despite his advanced age, certain aspects of ethical living were new to him; these themes had helped him to sort things out and relate values better. At T1, although they had taken up the challenge to reflect on their past, some participants doubted whether a fundamental lifestyle change at an advanced age really made sense and whether applying the virtues in Western culture was utopian.
“I question a lot of things that now, that […] actually I've lived through my whole life like this, it's sometimes not all that good […] because, yes you question a lot, you've already gone a certain way and say […] Is it worth starting over?” (59 years old, T1)
In contrast, after 6 months, participants reported entirely positive effects of the reflection process.
Recognizing new opportunities
The course topics not only encouraged people to come to terms with the past, but they also led them to proactively reflect on their own behavior in everyday life.
“Yeah, so this self-study, that's something, yeah, when I lie in bed at night and think: ‘How could you have done it differently?’” (48 years old, T2)
This reflection led to more inner clarity and also the courage to take appropriate opportunities for change.
“It has changed that I […] that everything has become much clearer to me. I have to say.” (55 years old, T2)
During the course, most participants became aware of intra- and interpersonal mechanisms that can promote a lifestyle with greater eudaimonic well-being.
“the connection between gratitude and contentment, that's always the ‘aha,’ like a light going on in your head.” (61 years old, T1)
“And I notice that if I am more responsive to him [life partner], which I can do well at the moment, we quickly find the connection to each other.” (30 years old, T1)
The overall picture that emerged from the interviews at T2 was that participants' experiences had settled, deepened, and occupied a larger space in their own lives: “my way of life has completely changed.” (55 years old, T2)
New values
In response to the opening question on perceived changes in daily life, interviewees reported a number of intentional and motivational changes regarding their values at both T1 and T2. Half of the respondents described a desire for more congruence between lived and felt realities in life: “Yes, this coming to terms with myself, being at peace with myself, that is a very important […] life lesson for me. Being at peace with myself at last.” (59 years old, T1)
Some participants expressed gratitude for the opportunities and resources already available in their own lives: “You can be so grateful and, and, and sit down and smile and say ‘You don't really have anything to do. Do everything you enjoy, everything.’” (61 years old, T1)
Several participants mentioned satisfaction as a new value, noting in this context that material wealth no longer played such an important role in their hierarchy of values: “In the old days, that is, a few months ago, I would have been satisfied with a pile of money that meant I could afford anything. But that doesn't matter at all. And now, for the first time, this thinking has been stimulated.” (30 years old, T1)
Another common denominator that emerged was rediscovered value of interpersonal family relationships; coupled with this, domestic duties and media consumption were becoming less important.
“Spending more time with the family, not just cleaning, or cooking all the time.” (53 years old, T2)
“This togetherness, this listening, even if you just chat with each other for an hour, that's right, and not the other thing, this radio chatter all day or the TV that just drives you crazy, no, … and I always used to have something on somehow, even in the car.” (59 years old, T1)
Broader values, such as nonviolence, forgiveness, or truthfulness, were emphasized by individual participants, especially at T2. The overall impression was that the MBLM course turned participants' attention to new values: “This letting go and this forgiving. So now this, yes how can I put it, also this being more generous with each other, also the gratitude.” (63 years old, T2)
This interviewee was aware of this through changes in her lifestyle and generating hope for a better life, as she concludes: “I'll say this, it's my only lifeline. I'm relatively sure of that, only if I live that and the sense that I've always had inwardly anyway, which I've had confirmed here, if I live this serenity and calm, if I live this meditation, if I practice ethical living, I'll have a beautiful life.” (37 years old, T1)
Serenity
Engaging with the course content made all participants feel calmer. This was expressed through more balance and inner peace. Often, participants associated this greater composure with a higher level of acceptance on the one hand, and the ability to set boundaries on the other.
Experiencing calm
Feeling calmer was mentioned by almost all interviewees at both interview times and was expressed individually in different experiences. One-third of the participants reported experiencing more calm, especially related to mantra mediation: “the meditation makes me calmer. Takes me from problems to other issues, to other thoughts, other content.” (55 years old, T2)
Another third reported feeling more balanced, more stable, and less agitated in everyday situations: “the last few weeks I've had a really intense feeling that I've become much calmer, […] and that I also just don't get upset anymore.” (30 years old, T1)
Another comment on this topic concerned communication with other people; one interviewee noted being able to be more present and being less impulsive: “To just be present, stay calm […] I also behave differently toward others.” (59 years old, T1)
Recognizing and setting boundaries
Two-thirds of the participants addressed an awareness of their own limits and the ability to assert this in different contexts; the latter was more important for interviewees at T1: “But now I'm trying to set my boundaries a bit. … because I notice my own limits.” (64 years old, T1)
Besides recognizing their own (physical) limits, participants mentioned setting boundaries related to circumstances that could not be changed like their own past, the expectations and opinions of other people, and past or harmful relationships: “I can say now that we also have confrontations at times, I've learned that too. To stand by my opinion and not tell anyone what to say anymore.” (63 years old, T2) “He's just like that, but it's his [ex-partner's] issue though. I'll leave that with him.” (61 years old, T1)
Acceptance
At T2, more than half the interviewees expressed having achieved a higher level of acceptance. Some mentioned acceptance of the past, of the present, of the course of life, and, in general, of the things they could not change: “That's the way things are […] you just have to be prepared to accept the way things are and make the best of it. And that's what I think I've learned a little bit.” (48 years old, T2)
Other statements referred to accepting one's own subjective shortcomings or wrong decisions: “Oh God, I could be 5 minutes late. Yes, then that's how it is. My God, we're all just people.” (30 years old, T1)
However, reference was also made to allowing for other people's shortcomings: “I've been really very offended and hurt when sometimes he hasn't contacted me at all for weeks and months. In the end, now I see it in a different light, he has his job and he is self-employed.” (63 years old, T2)
Mindful living
All participants reported greater mindfulness in the broader sense, which was expressed in self-awareness, being present in the moment, and conscious interactions.
Self-awareness
The following citations range from a focus on their own person, to increased introspection, to regained perception of their own presence, including their physical presence: “that I can act from my center, according to my needs, which I first have to feel, the course also helped me with that.” (61 years old, T1) “I listen to myself even more now.” (59 years old, T1)
At T2, the associated gratitude and self-esteem were also addressed: “And there's various gifts that I've rediscovered, that I can use them for myself, and that bring me joy and I wouldn't have got there without the study.” (56 years old, T2)
Being present
Almost all participants stated that they were able to experience the present moment more consciously and be more present in it, especially at T1. On this topic, one-third of respondents reported being more focused on the task in hand and multitasking less: “I do things more thoughtfully now, that is, no longer at the same time, but […] I concentrate more on things and think about them.” (53 years old, T2)
For another third of the interviewees, conscious awareness of the present moment had become a source of pleasure: “well, you see nature quite differently when it awakens […] spring with the birds and the flowers, well, I never experienced that before.” (63 years old, T2)
More physicality, associated with the yoga exercises and slowing down, was experienced as positive, although this appeared especially in the T1 interviews: “these movements in yoga, that is such a physicality that I feel there. Where I used to just whizz over it.” (61 years old, T1)
Conscious interactions
All participants expressed more conscious behavior in social interactions at both interview times. In particular, more open and honest interaction with life partners and other family members was cited as leading to deeper relationships: “then we also have deeper conversations, […] that was not the case before, or very, very rarely, and now we take time out more often.” (53 years old, T2)
Almost all interviewees experienced taking a calmer, more respectful, and more considered approach. They said that communication was more attentive and receptive, so criticism and needs could also be heard, as the following examples illustrate, both in the context of the relationship and in their social circle: “And I notice that if I respond to him more, which I can do well at this moment, we can connect really quickly.” (30 years old, T1) “There are also situations […] where I now say ‘I'm listening, I'm listening to this.’ Don't say so much, just give him a hug and then I've already helped.” (61 years old, T1)
Differences between the interview times
No themes emerged at T2 that differed from those at T1. However, the frequencies with which some themes or subthemes were mentioned changed with time. Reappraisal remained the most dominant theme at T2 and, unlike the other themes, was mentioned by all interviewees in all subthemes. The largest increase in individual mentions was recorded for the theme serenity, whereas two subthemes gained importance: acceptance and “recognizing and setting boundaries.” The theme mindful living lost relevance in the subtheme “being present.” A detailed overview of the changes is presented in Table 3.
Differences in Frequency of (Sub-)Themes Between T1 and T2
Number of participants mentioning a theme (n) and total number of statements that have been assigned to that particular (sub)theme (s)—directly after 8 weeks on the MBLM program (T1) and 4 months later (T2). The last two columns on the right show the difference between T2 and T1 in number of participants (Δn) and statements (Δs).
MBLM, Meditation-Based Lifestyle Modification.
Discussion
In this study, we analyzed semi-structured interviews to explore subjectively experienced intra- and interpersonal effects of MBLM practice on 12 outpatients with mild-to-moderate depression.
The most prominent theme that emerged from analysis of these interviews was reappraisal: reflection on past and present life, leading to new health-promoting opportunities and values. Virtue-based ethics (yoga yamas and niyamas) were explicitly mentioned as a key factor and an inspiring source of reorientation. Individuals sometimes described their insights as shocking, and the ideal of life proposed by yoga was occasionally perceived as utopian. Nevertheless, overall, reappraisal led to individual empowerment and an appreciation of one's own strengths. These changes tended to become more manifest after 4 months (T2) and can be interpreted as an antidepressant factor according to positive psychology. 28 The theme of empowerment (found in the subthemes “realizing new opportunities,” “recognizing and setting boundaries,” and “conscious interactions”) has also been reported in qualitative studies of (primarily) body-oriented yoga for people with depression, 29,30 but it was less prominent and referred to with less explicit cognitive and motivational statements.
As expected, due to its emphasis in MBLM, the participants explicitly highlighted values and virtues, and described them as a source of new vitality, inspiration, and orientation in their lives. This is consistent with Koenig's well-known model of spirituality and health, in which spiritual practice leads to the development of virtues, which, in turn, promote mental health. 31
Reappraisal based on insights from virtue-based ethics also played an important role in interpersonal relationships and supported a more relaxed attitude in conflicts, a higher level of acceptance, and better ability to set boundaries and be more compassionate with others.
The centrality of ethical living in this study is in line with neurophysiological models of classical yoga 32,33 and supplements existing empirical models 9 with the explicitly cognitive components of MBLM's virtue-based ethics. Regarding the treatment of depression, developing healthier relationships has been shown to be effective and is one of the key factors in interpersonal psychotherapy. 34 Further, the subtheme “experiencing calm” expresses emotional stability and quieting of the mind as a mechanism of self-regulation, which is beneficial to symptoms of depression, such as mood changes, anxiety, intrusive thoughts, and rumination. States of calm, a key element in meditative movement and a recurring theme reported in yoga studies, 4,35 were mentioned by participants in the present study with regard to body postures, but above all related to the practice of mantra meditation.
In the aforementioned synthesis of qualitative studies on body-oriented yoga practice for people with mental health conditions 6 of 11 studies were conducted with patients with depression. 4 A comparison of the themes of these studies with the themes and subthemes identified in our study highlighted some differences. First, although the theme “healing as a process” (with the subthemes “overcoming obstacles” and “barriers to practicing”) was prominent in the synthesis, it was less so for the participants of this study. One reason for this could be our participants' inspiration from virtue-based ethics, which may have made the daily routine of yoga and meditation practice more varied and attractive. Further, although asked about it directly, our interviewees appeared less focused on their illness than is usually observed in patients with depression. 36 Instead of mere symptom relief, they commonly expressed a more global goal with phrases such as “being at peace” or “finding inner peace.” One possible explanation is that participants may have identified less as a “depressed person” after the MBLM program, which would be in line with its salutogenic and eudaimonic mechanisms of action and their effects on well-being. 37 Second, the key theme in the synthesis, “alleviation of suffering,” overlaps considerably with a key theme in this study, serenity, centering around emotional and cognitive stability. Although a subtheme in the synthesis, “physical health” was not raised by MBLM participants, they did report on specific psychological mechanisms to reduce suffering (namely, “recognizing and setting boundaries” and “acceptance”). Third, in the synthesis, the key theme of “self as an agent of change” showed a partial overlap with the MBLM study subthemes “realizing new opportunities” and “conscious interactions.” The synthesis subthemes of connectedness and “appreciating a holistic approach” were not explicit themes for the MBLM participants (although mentioned in some individual statements).
Finally, our participants made only sparse explicit statements about any change in spiritual experience or attitude. One possible explanation for this is the brevity of the intervention. Spiritual growth is a long-term and complex process. 38 Further, spirituality is a complex psychological construct, 39,40 to which limited reference was made in the interviewees. Conscious aspects of the human psyche were easier for the interviewees to access and changes could remain unconscious, but these were still visible in behavior. The theme of serenity, and the subthemes of acceptance and new values that we identified could be interpreted as spiritual components, as for example in acceptance and commitment therapy. 41 The MBLM also works well in a secular, humanistic context, however, and participants could have preferred this interpretation.
The study is not without its limitations. Due to the design and the sample size, no statements can be made about the specific effects regarding diagnosis, duration of illness, number of episodes, severity of depression, age or gender, or existing comorbidities. Further, the specific effects of the individual components of MBLM, as well as interactions with existing therapies (e.g., previous psychotherapy, which was highly variable in our sample) can hardly be distinguished. From a sociodemographic point of view, the sample shows a relatively realistic gender ratio, since women are significantly more likely to be affected by depression than men. 42 Future studies could focus more on male participants, especially at a younger age, to be more representative.
Although the sample size is appropriate for thematic analysis, future studies should replicate the results using a larger sample, ideally in a multi-center approach. Treatment-naive participants should also be examined to rule out any interactions with previous therapies.
The strengths of the study include the novelty of the program in the field of integrative treatment of depression and the in-depth insights we gained into participants' subjective theories on how (well) it worked.
Overall, the results of this qualitative study provide complementary evidence of the effects of MBLM in the treatment of mild-to-moderate depression examined in the MBLM-D study. In particular, the explicit therapeutic implementation of virtue-based ethics may offer a valuable addition to previous mind–body programs. Reflection on virtue ethics in one's life may lead to transient distress; hence, sensitive therapeutic support is required to respond appropriately to unfavorable psychopathological developments. Nonetheless, new resources could be activated in the therapeutic process, even for patients with a long history of therapy. This shows the power of an integrative approach, in which physical, cognitive–emotional, social, and spiritual aspects are combined in a setting of continuous practice.
Footnotes
Authors' Contributions
H.C.B. and P.S. conceptualized and designed the study. J.V., J.G. were involved in the acquisition of data. K.M. and P.S. supervised the data analysis. J.V., J.G., H.C.B., and K.M. contributed to qualitative analysis and reporting. H.C.B. wrote the first draft of the article. All authors worked on the final version of the article.
Ethical Approval
Granted by the Ethics Review Board of the University of Chemnitz University of Technology (V-276-15-PS-MBLM-D-14062018).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was funded by Karl and Veronica Carstens Foundation under Award Numbers KVC 0/098/2018.