
Abstract
Background:
Complementary and alternative medicine (CAM) could be one option to address perceived insufficient milk (PIM), but there are few data comparing the effectiveness, acceptability, and safety of various CAM therapies. The purpose of this study was to describe and compare, among women delivering at 34–376/7 weeks, the feasibility and acceptability of two CAM interventions for treatment of PIM: (1) a meditation/relaxation intervention via an MP3 (Apple iPod Shuffle©) player and (2) a commercially available combination-blend herbal supplement (Motherlove: More Milk Plus Alcohol Free®).
Materials and Methods:
After randomization, over 9 days, women received three home visits from a lactation consultant, recorded pre/post intervention test weights and expressed milk volume, tracked daily breastfeeding behavior, and completed an end-of-study interview about the interventions. Women in each group were offered the other group's intervention on study day 9. Breastfeeding status and intervention continuation were assessed at 2 months.
Results:
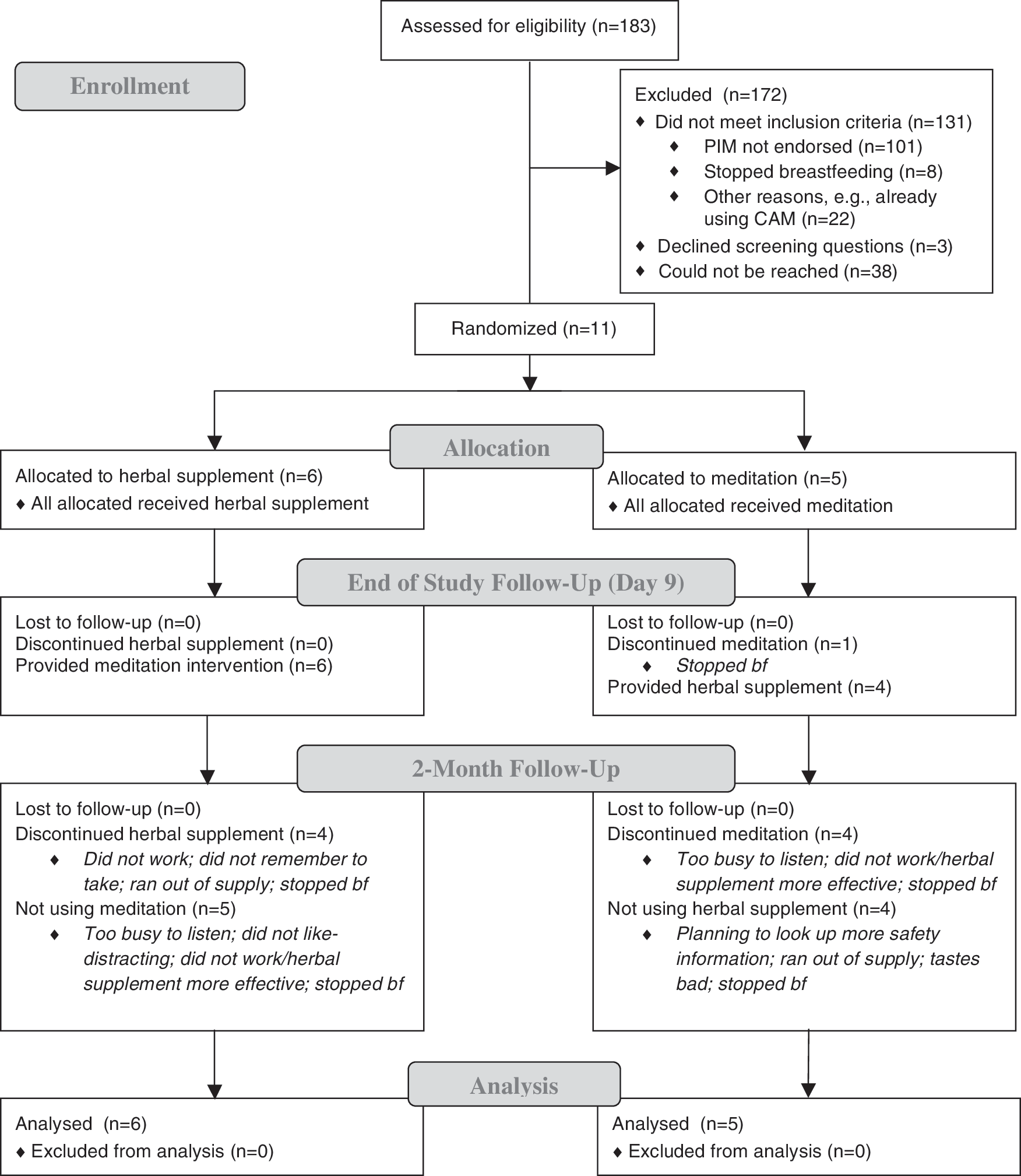
Of 183 women screened, 11 were eligible, enrolled into, and completed the 9-day trial. Six women were randomized to the herbal supplement and 5 to meditation. One participant (meditation) stopped breastfeeding on study day 8. At 2 months, 3 of 6 women assigned to the herbal supplement and 3 of 5 women assigned to meditation were still breastfeeding; 1 (herbal supplement) was exclusively breastfeeding. Most participants were adherent to the prescribed protocols for both interventions. Interventions were generally perceived as safe, with benefits not necessarily related to increased milk supply.
Conclusion:
Mothers of late preterm and early term infants who had PIM found the CAM interventions acceptable and safe. The effect of CAM therapies on breastfeeding outcomes, with and without in-home lactation assistance, requires further investigation.
Introduction
Perceived insufficient milk (PIM) is among the most frequently cited reasons for formula supplementation and early breastfeeding cessation throughout the postpartum course. 1 –3 Mothers of infants born in the late preterm or early term period (i.e., 34–386/7 weeks of gestation) are at particular risk for PIM and shortened breastfeeding duration. 4 Reasons include maternal health conditions associated with preterm births that also affect milk supply (e.g., type I diabetes) and infant physiologic immaturities contributing to insufficient milk transfer. Often, a cascade effect is observed involving insufficient milk removal, formula supplementation, decreasing milk supply, and breastfeeding cessation. 5 Anxiety and depressed mood, potentially related to a difficult peripartum course, may also contribute to PIM in mothers of preterm infants. 6 –9 Anxiety affects milk availability through oxytocin inhibition and possibly through other hormonal pathways. 10,11 Psychologic disturbance may also decrease maternal morale and breastfeeding or milk expression at regular intervals. 12
Use of complementary and alternative medicine (CAM) to address a variety of health conditions, including PIM, is increasing worldwide. 13,14 Compared to pharmacotherapies used to increase milk supply (e.g., metoclopramide, domperidone), the use of CAM for PIM treatment is attractive because of fewer presumed health risks and lower administration costs. However, there remains an overall lack of evidence regarding the effectiveness, safety, and acceptability of many CAM therapies for PIM, including acupuncture, herbal supplements, and relaxation/visual imagery techniques. 15 –17 Despite this, herbal supplements are widely used and recommended by lactation consultants. Meditation and other cognitively based relaxation techniques have also emerged as noninvasive, potentially effective interventions for PIM affected by stress or anxiety. 18,19 While management of underlying physiologic, mechanical, or hormonal problems remains the appropriate first-line step for correcting PIM, these strategies do not account for PIM that is psychologically based or slow to improve with conventional treatment approaches.
A pilot feasibility study was conducted to compare, within a late preterm/early term infant population, the feasibility and acceptability of two CAM interventions for treatment of PIM without a definitive physiologic or mechanical cause: (1) a meditation/relaxation intervention and (2) a combination-blend herbal supplement, the components of which are purported to enhance the milk ejection reflex and increase milk flow. 17,20
Materials and Methods
This study was approved by the University of Pittsburgh's institutional review board. Between April 2013 and August 2014, 183 postpartum women who delivered between 34 and 376/7 weeks of gestation and intended to breastfeed for at least 2 months were screened for participation in a pilot intervention trial addressing PIM. Infants 380/7–386/7 weeks were not included in this study, as enrollment commenced prior to The American Congress of Obstetricians and Gynecologists' expansion of the “early term” designation and associated risk for feeding problems to infants born at 37–386/7 weeks. 21
Women were approached during their postpartum hospitalization at a large regional obstetrical hospital or referred from a community-based primary care pediatric clinic. After obtaining the women's written informed consent, initial eligibility criteria were assessed, including currently providing any breast milk, intention to provide breast milk exclusively for at least 2 months, and absence of conditions with potential to affect milk supply (e.g., hypothyroidism, polycystic ovarian syndrome). Women meeting these criteria received a telephone call at 1–2 weeks postpartum to assess additional eligibility parameters, including breastfeeding or pumping at least six times per day and perception of low or insufficient milk supply; 1–2 follow-up calls were made to reach women, up to 3 weeks postpartum. Enrollment within the first 3 weeks was designed to capture women in the peak period for PIM development related to misinformation and anxiety, 22,23 and prior to breastfeeding cessation. Although milk removal at least eight times per day is the recommended minimum to ensure adequate milk supply, women who might have reduced breastfeeding efforts recently because of difficulties, including PIM, were included.
Women meeting all eligibility criteria were enrolled into the 9-day study and randomized to receive a meditation intervention on an MP3 player (Apple iPod Shuffle©) or a commercially available herbal supplement (Motherlove: More Milk Plus Alcohol Free®) containing fenugreek (Trigonella foenum-graecum), blessed thistle (Cnicus benedictus), nettle (Urtica dioica), and fennel (Foeniculum vulgare). Women in one intervention group were offered the other group's intervention at the last study visit. Computer-generated block randomization was used to ensure near-equal allocation to each group in this small sample. To estimate feasibility parameters, the goal was to enroll a convenience sample of 20–25 women.
Participants received three home visits with a lactation consultant, which included infant-weight measurement and breastfeeding assistance. Women also recorded study intervention use and side-effects, infant feeding (proportion of breast milk feeds, volume of expressed milk), and concern about milk supply (on an investigator-created 7-point Likert scale) daily in a written breastfeeding diary. The women also completed pre- and post-intervention infant test weights to measure volume of milk transfer and participated in a study-end interview about their experiences with PIM and the interventions. Women were called at 2 months to assess feeding status (Fig. 1). Each woman was compensated up to $50 and received the herbal supplement and MP3 player to keep.
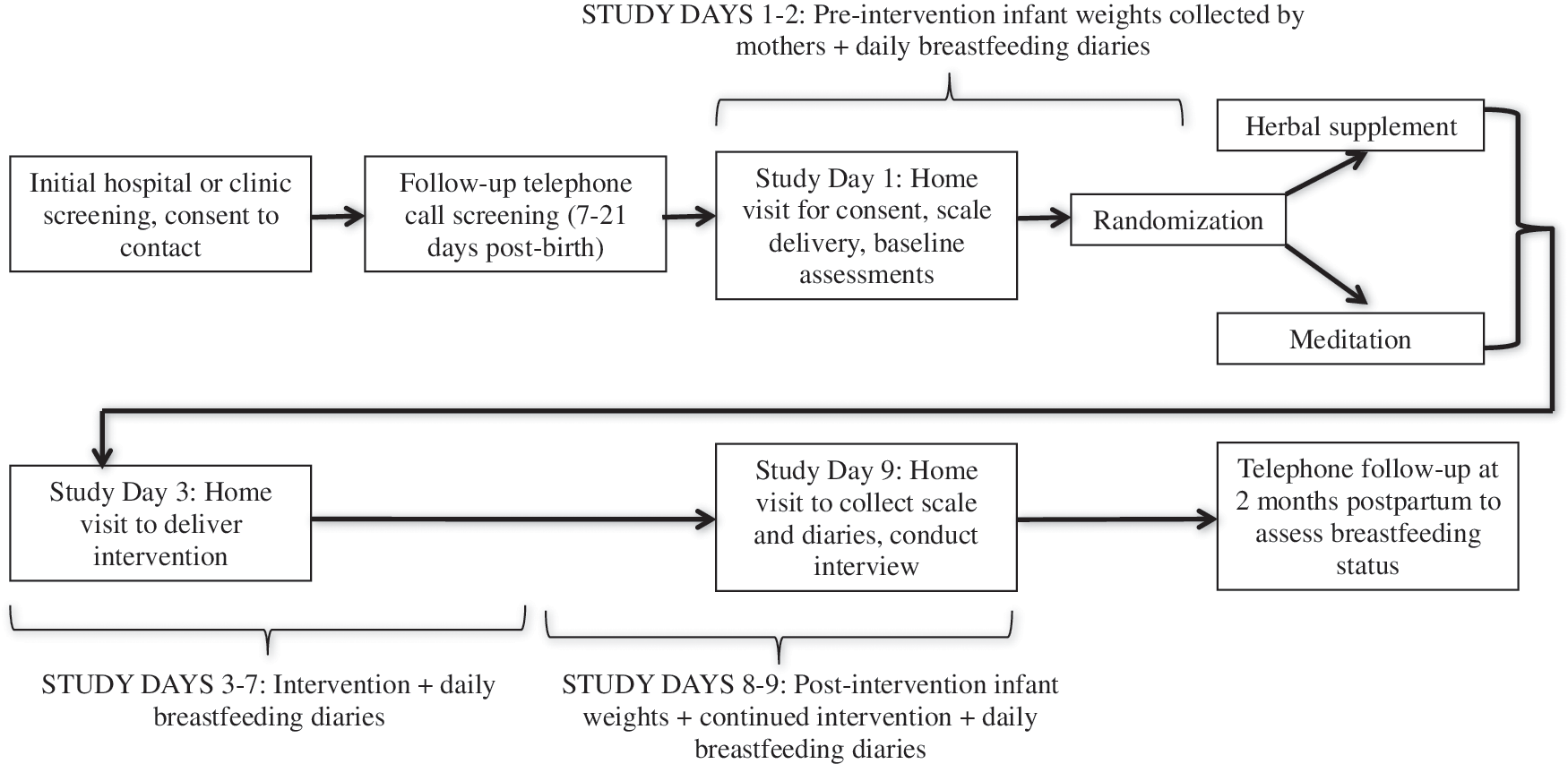
Participants were loaned Seca-334 portable infant scales and instructed in the procedure for obtaining in-home infant test weights to assess at-breast milk volume transfer. This scale is reported to be accurate to within 5 g for infants up to 10 kg. Mothers recorded prefeed and postfeed weights on study days 1–2 (preintervention) and 8–9 (postintervention), two times per day, when milk supply was perceived as being most abundant. Mothers weighed their infants obtaining two consecutive weights within 5 g. By subtracting the average postfeed weight from the prefeed weight, volume of milk transfer was obtained for a single at-breast feed. Mothers who also pumped/expressed breast milk recorded volume of expressed milk two times per day (plus largest volume expressed per day) when milk supply was perceived as being most abundant.
Participant mothers who were randomized to the meditation intervention received the MP3 player with three guided meditations modeled on mindfulness-based stress reduction 24 and recorded by a study investigator trained in the technique. The meditations were 5–8 minutes each and included a guided-imagery recording specific to breastfeeding, a guided thankfulness meditation (Loving–Kindness), and a guided relaxation (body scan). Participants were instructed to listen to the meditations of their choice at least twice each day, preferably when breastfeeding or expressing breast milk.
Mothers assigned to the herbal supplement were instructed to add the oral tincture to a palatable liquid<1 oz and drink it 3–4 times per day. Timing and dosage of the supplement were based upon the mother's current weight, as advised by the manufacturer. The product is reported by the manufacturer to be effective for increasing milk volume within 1–2 days. 25
Audio-recorded qualitative interviews were transcribed verbatim and a content analysis, utilizing Atlas.ti software v. 6.2 (Berlin, 2015) was conducted to identify major themes regarding perceptions of the interventions. Summary statistics were calculated for quantitative data using SPSS v. 21 (2012; IBM Corporation, Armonk, NY).
Results
Recruitment and Retention Feasibility, and Sample Characteristics
Of 183 women screened, 11 met all eligibility criteria and completed the 9-day study in its entirety (Fig. 2). Enrollment ceased at 11 participants because of the slow accrual of subjects. Five women were randomized to meditation and 6 to the herbal supplement. All participants who were still breastfeeding at study day 9 (n=10) responded to and completed the 2-month follow-up telephone call.
Participants ranged in age from 23 to 35 years, all were non-Hispanic, and 73% identified as white, 2 as black, and 1 as “other” race. All of the women were at least high-school graduates, with 4 college graduates. Six women were married, 4 were living with partners, and 1 was single. Five women delivered between 36 and 366/7 weeks, and 6 delivered between 37–376/7 weeks. Eight women were primiparas and had never previously breastfed. The 3 women with other children all had previously attempted breastfeeding. All participants made the decision to breastfeed during their pregnancies. One participant was taking methadone for chronic pain symptoms, and her infant had a 9-day neonatal intensive care unit (NICU) stay for withdrawal symptoms. Timing of study entry ranged from 9 to 16 days postpartum.
Breastfeeding Status and Perceived and Actual Milk Supply
All participants continued to breastfeed or provide some breast milk until the end of the study (study day 9), with the exception of 1 participant in the meditation group who stopped breastfeeding/providing breast milk on study day 8 because of her perception of inadequate milk. Three women breastfed/provided breast milk exclusively during the study: 2 in the herbal-supplement group; 1 in the meditation group. At the 2-month postpartum follow-up, 3 of the 6 women assigned to the herbal-supplement group were still breastfeeding or providing breast milk, and 3 of 5 women assigned to the meditation intervention were doing so; only 1 participant (in the herbal supplement group) was breastfeeding/providing breast milk without formula supplementation at 2 months.
Two participants—1 from each intervention group—believed they had enough breast milk to satisfy their babies at study day 9. On the 1–7 Likert scale for concern about milk supply, participants in the herbal-supplement group averaged 4.5 at study day 1 and 3 at study day 9; participants in the meditation group averaged 5 at study day 1 and 4 at study day 9. See Table 1 for pre- and postintervention milk volumes, proportion of breast milk feeds, and infant weights.
Average over 4 separate test weights during study days 1 & 2.
Average over 4 separate test weights during study days 8 & 9 (study intervention provided on study day 3).
Average over 4–6 separate pumping/expressing sessions during study days 1 & 2.
Average over 4–6 separate pumping/expressing sessions during study days 8 & 9.
Average of participant-reported daily proportion of breast milk feeds on study days 1 & 2.
Average of participant-reported daily proportion of breast milk feeds on study days 8 & 9.
Researcher measured weight at study day 1 (except P1, which was measured on study day 3 because of late change in study protocol).
Researcher measured weight at last home visit (study days 8–10).
Breastfed or provided breast milk exclusively throughout study.
N/A, data not available.
Maternal reasons for (and volume of) formula supplementation varied by time postpartum and included recommendation by pediatric providers for hypoglycemia, hyperbilirubinemia, and/or excessive weight loss; latching difficulties; insufficient milk output with electric or manual pumps; and perceived decrease in or inadequate milk supply related to an unknown or suspected physiologic or mechanical cause (e.g., retained placenta, infrequent breastfeeding or milk expression attempts).
Intervention Feasibility
According to the daily breastfeeding diaries, all women randomized to the herbal supplement took the recommended dose at the recommended frequency for the duration of the study (with the exception of single missed doses for 2 participants). All women randomized to the meditation listened to the recordings at least twice per day, typically when pumping or breastfeeding, as recommended (except for 1 participant who missed 3 recordings).
At 9 days, all but 1 participant accepted the offer to try the other intervention. At 2 months postpartum, 2 participants originally allocated to the herbal-supplement group continued to use the herbal supplement, and a third participant in the herbal-supplement group was still using the meditation intervention. All other participants had ceased using both interventions (Fig. 2).
Perceptions of the Herbal Supplement
Women discussed perceived efficacy, drawbacks, side-effects, and benefits of the supplement. Regarding efficacy, women were divided in feeling that the supplement: (1) decreased supply (n=1); (2) had no effect (n=1); (3) required additional time for evaluation (n=1); or (4) might have increased supply (n=3; versus natural increase in milk production over time or a placebo effect—i.e., “me wanting it to work”). The participant who felt the supplement decreased her supply revealed that she was mixing it with more than 2 oz of liquid, contrary to the manufacturer's recommendations.
One participant attributed a faster let-down reflex to the supplement, and 1 felt that the supplement sweetened her breast milk such that her baby enjoyed breastfeeding more. Perceived drawbacks of the supplement included the taste; perceived potential for infant side-effects (n=1); and maternal side-effects, including headache (n=1), nausea (n=1), maple-syrup smell to bodily secretions (n=2), and increased perspiration (n=1).
Perceptions of Meditation
Only 1 participant attributed an increase in milk volume to meditation. Other participants reported that meditation had little or no effect on milk supply, but did find it to be a “pleasant experience,” “peaceful,” “relaxing,” or helped to clear and/or focus the mind. One participant reported that the intervention was “too relaxing” to the point where she became drowsy and worried about dropping her infant. Other barriers to listening included dividing attention between the baby and meditation (n=1) and headphone wires touching the baby (n=1). As a result, some women listened to meditations only when pumping or apart from their infant. One participant mentally practiced meditations while breastfeeding or pumping instead of listening with headphones. Women generally found the MP3 player easy to use.
Other Study Components: Test Weights and Home Visits
In general, women found the test weights easy to obtain. However, only 1 participant used the test weights for their intended purpose—to determine milk transfer in a breastfeeding session. Others found the test weights “reassuring” as a visual gauge that the baby was indeed “getting something” and to observe overall trends in weight gain. Participants generally found the home visits by the board-certified lactation consultant helpful and convenient. One participant stated that access to the lactation consultant was her incentive for study participation.
Discussion
Mothers were willing to participate in this pilot feasibility CAM trial, adherent to prescribed CAM regimens, and reported few side-effects in themselves or in their infants. Breastfeeding continuation in the study at 2 months was 55%, which is 10% higher than reported in similar gestational cohorts around 1 month of age. 26 The effect of the tested CAM interventions, with and without the addition of in-home lactation assistance, on milk supply, breastfeeding duration, and formula use requires further study with an adequately powered sample.
Despite adding new recruitment locations and increasing recruitment time, it was not possible to reach the goal of randomizing 20 women. This was likely because of the variable onset of PIM and the asynchronous timing of the screening calls. Indeed, PIM is among the most frequently cited reason for formula supplementation and early cessation of breastfeeding. In a 2003 cohort study including 1163 mother–infant dyads, the most common reason for breastfeeding discontinuation through 6 weeks postpartum was belief that the infant was still hungry after breastfeeding or that there was not enough breast milk. 2 Similarly, Odom and colleagues found that, in their sample of>1100 women who completed monthly surveys about breastfeeding from 2 to 12 months postpartum, 60% of the women did not breastfeed as long as they intended. 1 The top reasons given for early breastfeeding cessation were not having enough milk and feeling that breast milk alone did not satisfy the baby. 1
It remains difficult to identify and address milk supply issues in a timely manner (actual or perceived), largely because: 1) “diagnosis” is typically based on subjective interpretation rather than objective measurement (i.e., volume of expressed milk is not always indicative of actual milk supply); 2) etiology is multifactorial and could include a primary physiologic problem (e.g., maternal endocrine disorder), misinterpretation of normal feeding patterns, inadequate breast stimulation, and/or behavioral or psychologic response to a perceived supply problem 27 ; and 3) the problem evolves rapidly (e.g., women decide to stop breastfeeding before receiving help). As such, PIM may be best addressed through a prophylactic, rather than post-hoc, care model. For example, provision of anticipatory education during pregnancy and/or throughout the early postpartum period could be an effective counter to the rapid escalation of PIM and its consequences. 28
Another novel potential strategy to prevent development of PIM is antenatal milk expression (AME). AME capitalizes on milk production beginning in mid-pregnancy by teaching women how to hand-express, collect, and store milk in the third trimester. Milk can be used if needed after birth instead of formula. Women also develop confidence in their milk production, handling breasts, and expressing milk prior to delivery, when they may be more receptive to learning. There is some evidence suggesting that AME contributes to a larger postpartum milk supply and improved breastfeeding duration and exclusivity. 29 –31
Despite the difficulty the current authors had in identifying potentially eligible women, the study demonstrated acceptability of the tested post-hoc CAM treatments for PIM in a group of late preterm and early term mothers. This is consistent with recent population survey data in Western Australia indicating that 60% of postpartum mothers used herbal supplements while breastfeeding, with the majority believing that these supplements were effective for increasing milk and 43% citing them as safer than conventional medicines while breastfeeding. 14 With the exception of the current study, there is a lack of comparable research documenting the acceptability of herbal and nonherbal CAM treatments for PIM in the United States. While women were not convinced of the effect of tested CAM interventions on actual milk supply, these participants noted alternate benefits including relaxation, which may have other health benefits for mothers and infants. As the women indicated, it is possible that a longer observation period with CAM would result in improved perception of milk supply.
Reviews of herbal supplements for increasing milk production have been inconclusive because of small sample sizes and lack of randomization, blinding, and control groups. 16,20 According to the Academy of Breastfeeding Medicine's clinical protocol for galactogogues, 32 “the mechanism(s) of action for most herbals are unknown. Most of them have not been scientifically evaluated, but traditional use suggests safety and possible efficacy.” Herbals for increasing milk supply come in a variety of preparations, including capsules, liquid tinctures, and teas. Most are available for over-the-counter purchase in drugstores, health and nutrition stores, and other retailers across the United States. Many preparations, such as the one used in the study, contain multiple purported galactogogues, rather than a single herb alone.
One of the most common herbal supplements available as a single- and multi-ingredient preparation is fenugreek. Although the mechanism by which fenugreek may increase milk supply is unknown, it is reported to have antianxiety effects 33 which have the potential to positively affect milk production. Fenugreek is GRAS [“generally recognized as safe”] by the U.S. Food and Drug Administration. There are no data on maternal or infant drug levels of fenugreek, or on its transfer into human milk. One study examining the effects of single-ingredient fenugreek in mothers delivering at<31 weeks of gestation (3 capsules, three times daily, for 21 days) found no significant difference in milk production between mothers receiving the fenugreek versus a placebo. 34 Conversely, another placebo-controlled trial found that mothers drinking a multi-ingredient herbal tea containing fenugreek three times per day had a significantly greater milk supply on the third postpartum day and their infants had a more rapid return to birthweight; the individual effect of fenugreek in this study could not be determined, however. 35 Other herbal supplements with some evidence of a positive singular effect on milk supply include wild asparagus (Asparagus racemosus), 36 garlic (Allium sativum), 37 and micronized silymarin (Silybum marianum). 38
Domperidone and metoclopramide are two alternative prescription medications that have frequently been used off-label as galactogogues. Because of maternal safety concerns (reports of arrhythmias from intravenous use in patients receiving chemotherapy), domperidone is not routinely prescribed in the United States, although data indicate that it may be highly effective for increasing milk volume. 32,39 –41 There have been multiple randomized, placebo-controlled blinded studies that found essentially no differences in milk volumes produced between women given metoclopramide and a placebo. 42 –46 Metoclopramide may cause serious maternal side-effects, including depression with long-term use and extrapyramidal symptoms. 47
The efficacy of other CAM therapies for addressing PIM, including relaxation/visual imagery, meditation, massage, and acupuncture also remains understudied. One small study (N=63) demonstrated a substantial increase in expressed breast milk volume in NICU mothers who listened to a relaxation/guided imagery intervention before each milk expression, compared to a control group. 18 More recently, a larger randomized trial (N=162) found that, among mothers with infants in the NICU, those who listened to music-based audio-recordings incorporating progressive relaxation and guided imagery had significantly more milk production, compared to a control group at 14 days postpartum. 19 Acupressure and acupuncture have also been associated with increased milk supply and improved breastfeeding duration compared to routine care or breastfeeding education alone, 48,49 but results have yet to be replicated in placebo-controlled or comparison group studies.
In most cases, it is unlikely that CAM would have a significant impact on milk supply as a stand-alone therapy for women with primary mechanical or physiologic causes of PIM. Rather, meditation and the herbal supplement tested should be considered reasonably safe and acceptable adjuvant therapies, along with lactation education, breastfeeding assistance from peers or healthcare professionals, and correction of underlying physiologic issues affecting milk supply. Professional clinical judgment should be exercised prudently when recommending CAM for treating PIM, weighing the preferences of the breastfeeding mother, the expense and availability of CAM, any drug-to-herb interactions, and the expected benefit. 32
The current study was limited by a number of factors. There was an underpowered sample, which did not permit testing for statistically significant between-group differences in outcomes. Related to the small sample, it was not possible to account for potentially confounding variables in the results, including adherence to interventions, other lactation assistance received, intensity of breastfeeding efforts (e.g., frequency of breastfeeding or milk expression), suspected etiology of PIM, and maternal or infant conditions or medications. Recruitment was also restricted to late preterm and early-term infants from a single hospital system, limiting generalizability to the larger population of women who may experience PIM.
Conclusion
Mothers of late preterm or early term infants endorsing a milk supply problem found the CAM interventions tested acceptable, safe, and potentially beneficial for increasing milk supply (herbal supplement) and/or promoting an overall sense of well-being (meditation). Future work should aim to study the efficacy of the interventions in an adequately powered sample, accounting for PIM etiology, breastfeeding intensity, adherence to interventions, and other lactation assistance received.
Footnotes
Acknowledgments
This study was funded by: the Ruth Perkins Kuehn Research Award-University of Pittsburgh School of Nursing, in Pittsburgh, Pennsylvania; the Ruth L. Kirschstein National Research Service Award Institutional Research Training Grant (T32HP22240 HRSA NRSA for Primary Medical Care); and the National Institutes of Health Pathway to Independence Award (NINR 1K99NR015106-01). The authors thank Maris Parker, MSW, for her help with data collection and Briana Deer, BS, for editorial assistance.
Author Disclosure Statement
The authors have no conflicts of interest to disclose. ■