
Abstract
Herbs used to prevent and treat gouty arthritis are reviewed in depth. Colchicum autumnale (autumn crocus) along with other sources of colchicine, including Gloriosa superba (flame lily), are described, both for their historical significance and relevance to the drug colchicine and also for their use as whole herbs. The reasons for considering whole herbs versus only isolated constituents in the context of Colchicum and colchicine are highlighted. Three herbal foods that are helpful for gout are then discussed: Apium graveolens (celery); Prunus avium (sweet cherry) and P. cerasus (tart cherry); and Coffea arabica (coffee). Various Chinese herbal formulas traditionally used for gout and now the subject of modern research are presented, notably Chuanhu antigout mixture, Er Miao Wan/San (Two Marvel Decoction/Powder), and Si Miao Wan (Four Marvels Teapills).
Introduction
The ancient malady of gout, while certainly never gone, is making a huge comeback in modern times. This condition is particularly prevalent in countries bordering the Pacific Ocean, but is generally common in all developed nations. 1,2 Research in China has shown a dramatic increase in gout incidence associated with rapid industrialization and westernization, with much higher rates in developed cities, compared to less-developed cities or rural areas. 3 Gout is far more common in adult men and postmenopausal women, and is almost never seen prior to adolescence in men or in premenopausal women.
Classic gouty arthritis (also known as podagra) is recognized easily, with a sudden onset of excruciating pain and erythema in the metatarsophalangeal joint of the large toe. However, gout also can present as acute bursitis or with atypical features (such as affecting other joints, affecting multiple joints at once, less-severe pain, or absence of erythema). An online calculator is available to help clinicians diagnose acute gouty arthritis correctly (see Gout Diagnostic Criteria).
Gout is clearly the result of people with certain genetic predispositions being placed in environmental conditions that result in precipitation of uric-acid crystals. Mutations that resulted in the inactivation of the uricase gene in modern humans, some primates, and some New World monkeys accrued 13–24 million years ago. 4 This has left the average, healthy adult male with an average serum uric-acid level of around 6 mg/dL, compared to <1 for most other mammals. 5 It appears that this evolutionary change was beneficial because uric acid is a powerful antioxidant, accounting for >50% of the antioxidant capacity in the blood. 6 This may have been particularly important and beneficial in light of the much-earlier (40–50 million years ago) loss of the ability for the hominid line to make vitamin C, which, at the time, was harmless because of the very high levels of vitamin C in the diets of human ancestors. 7 As vitamin C levels fell in the diets of subsequent evolutionary lines, the need for greater antioxidant protection was present and the chance loss of uricase may have filled this role. It is also possible that uricase loss was beneficial because it helped human ancestors maintain blood pressure despite extremely low saltlevels. 8 Whatever the reasons might be, it is clear now that some people suffer severely because of these ancient genetic changes.
A free online calculator that enables clinicians to apply moderately effective (with a positive predictive value of 64% and a negative predictive value of 87%) evidence-based diagnostic criteria quickly is available at:
This website provides entry to the ACR-EULAR Gout Classification Criteria table, which is downloadable as a pdf.
No superior criteria have yet been developed. The concomitant presence of gouty tophi in this study raised the diagnostic accuracy to 100%; their presence are essentially pathognomonic for gout.
_________________
Source: ACR-EULAR Gout Classification Criteria Calculator. The University of Auckland New Zealand, Medical and Health Sciences. Accessed September 7, 2016.
ACR-EULAR, American College of Rheumatology-European League Against Rheumatism.
The balance between intake and production of the precursors of uric acid, purines, and renal excretion of uric acid is crucial in whether or not someone will develop gout. The kidneys excrete 66%–75% of uric acid, with the gut removing the rest. Most (>90%) of patients with gout have trouble excreting enough uric acid (and are termed “underexcretors”). The URAT1 transporter is critical in the almost-complete reabsorption of uric acid filtered by the kidneys. The common gout drug probenecid blocks this transporter, leaving more uric acid in the urine to be excreted. Amlodipine, atorvastatin, fenofibrate, losartan, and corticosteroids have also all been shown to be uricosuric. This uricosuric effect results in a greater risk of uric-acid kidney stone formation, however. Note that aspirin, diclofenac, and loop and thiazide diuretics have an antiuricosuric action and increase the risk of gout. 9 Approximately 10% of patients with gout are overproducers of uric acid however, with the most extreme cases being in patients with secondary hyperuricemia caused by chemotherapy or hemolytic diseases that cause sudden massive releases of purines from cells.
The mainstay of all gout treatment is reduction of dietary purine intake, which primarily means reducing intakes of meats and seafoods. 10 Yet, higher intakes of vegetable sources high in purines, particularly mushrooms, do not increase the risk of gout. Overall, vegetable intake reduces the risk of gout mildly, as do dairy products. Thus, most patients who are prone to gout should primarily eat a vegetarian diet. Alcohol and fructose should also be avoided, particularly beer, as these substances increase the risk of gout significantly. Increased water intake can assist uric-acid excretion and will help prevent uric-acid kidney stone formation. Weight loss is also recommended for patients who are obese, as there is a strong correlation between obesity and gout risk. 10
Herbal therapies that help prevent and that can be used to treat acute gout can be used to augment the dietary approach to gout. While some patients will require medication to stop acute attacks or prevent future ones, many can do away with these by using a combination of lifestyle modification and herbal medicine. Specific useful herbs are discussed in detail in this article.
Autumn Crocus
The Eurasian native plant Colchicum autumnale (autumn crocus)—in the Colchicaceae family, which is related to the lily family—is the source of the first and still widely used effective drug for acute gout, colchicine. It is not clear when autumn crocus's medicinal properties were first recognized. Although many sources claim that this herb was mentioned in the ancient Egyptian Ebers Papyrus, one of the oldest, if not the oldest extant books that happens to be an herbal formulary, this appears to be caused by confusion of this plant with Citrullus colocynthis (colocynth). Dioscorides mentioned autumn crocus in his materia medica (written circa 60
There were many other unclear accounts of autumn crocus–like medicines used throughout antiquity, and it was not until the French military officer Nicolas Husson (who was not a physician) introduced his “Eau Médicinale” (a tea of the corm of autumn crocus) circa 1783 that indisputable accounts of use of C. autumnale for gout emerged. 12 This treatment became quite established in the 1800s as did research showing that it did not work by increasing excretion of uric acid in the urine or changing serum levels of uric acid. 13 As of the completion of the 2014 Cochrane meta-analysis, there were still only two small, low-quality published clinical trials, both supporting the efficacy of pure colchicine for addressing acute gout. 14 Low-dose colchicine (0.5 mg every 20 minutes for 1 hour) was just as effective as high-dose colchicine (up to 4.8 mg over 6 hours). However, high-dose colchicine caused high rates of adverse effects, with diarrhea, nausea, and vomiting occurring in ∼50% of test subjects (a statistically significantly higher rate than in placebo or low-dose colchicine groups), while low-dose colchicine did not cause any more adverse effects than placebo.
Colchicine, a major active compound in autumn crocus, was isolated in 1820 by Joseph Bienaimé Caventou (1795–1877
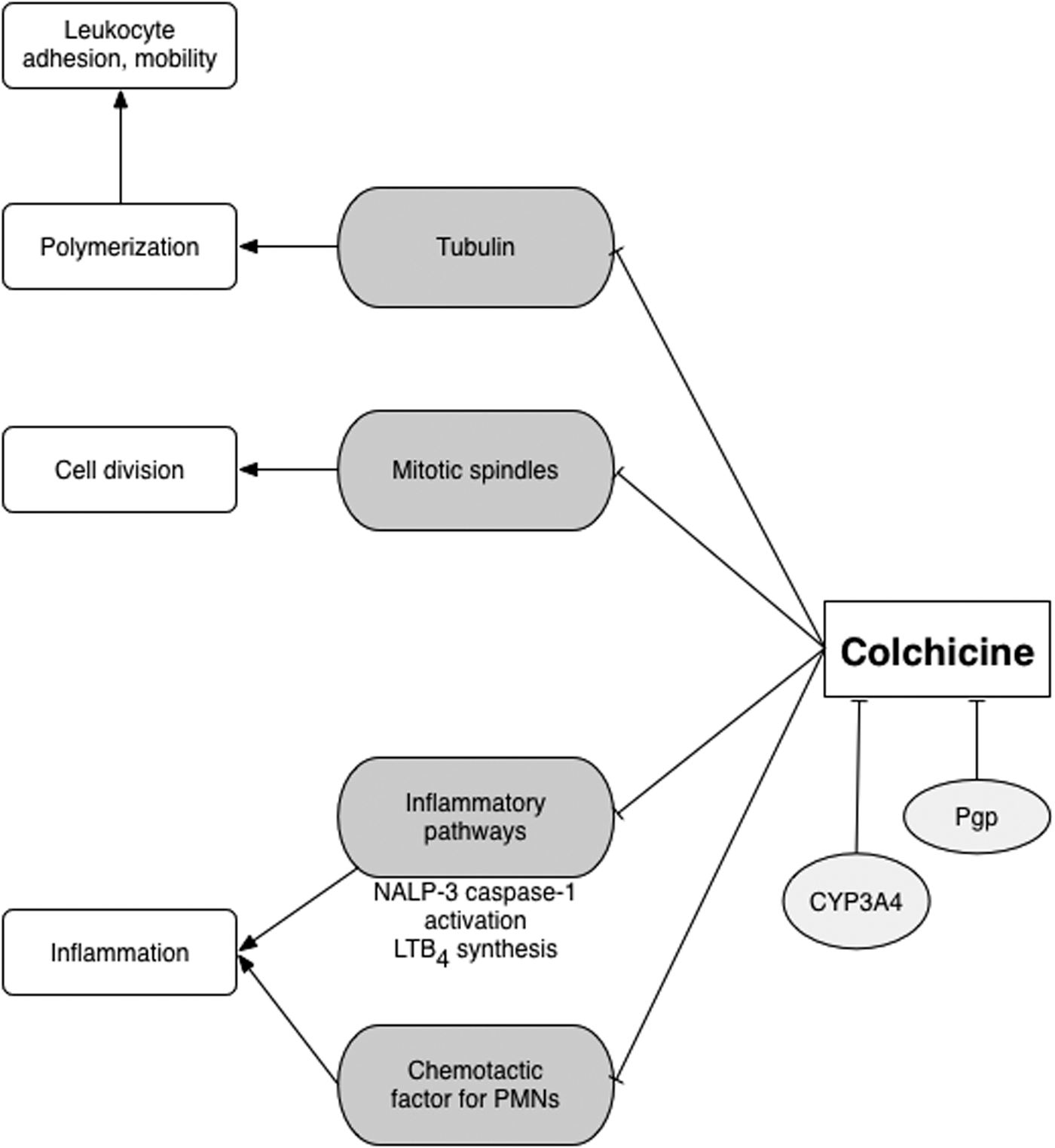
Mechanisms of action and metabolism of colchicine. NALP-3, NACHT, LRR and PYD domains-containing protein 3; LTB4, leukotriene B4; PMN, polymorphonuclear leukocytes.
The history of autumn crocus and colchicine is a familiar one in herbal medicine. A powerful herb has an “active constituent” isolated, which is then presumed to be the only active compound in the plant. This single molecule is then turned into a drug with its attendant increased toxicity, while the rest of the plant or use of the whole herb is then practically ignored. A growing body of research suggests that this is an error, and that the whole plant has activity not accounted for by colchicine alone.
Colchicine was in wide use prior to the existence of the U.S. Food and Drug Administration. When the FDA was created and regulation of the U.S. pharmaceutical market began, colchicine remained available as an inexpensive generic. However, the FDA had noted the lack of rigorous trials for this and many other pre-1962 generic pharmaceuticals. In the mid-2000s, the company URL Pharma did conduct trials and, in 2009, obtained FDA approval to sell branded colchicine under the name Colcrys.® The company received 3-year exclusive rights to sell Colcrys for treating gout and 7-year rights for treating familial Mediterranean fever—at a substantial price markup, compared to the previously available generics (which the FDA forced off the market). URL Pharma did not prove anything not previously known about the drug or find anything novel, yet the FDA received the desired proof and rewarded the company. There is evidence that the FDA's actions resulted in a decline of use of colchicine and a significant increase in patient expenditures among those who were prescribed the medication, suggesting a net decrease in patient well-being.a In a different, more patient-centered and less drug company–focused model, the U.S. government would have paid for trials to prove that the drug was effective and thus validated the ongoing use of the inexpensive generics already on the market.
_________________
Source: aKesselheim AS, Franklin JM, Kim SC, et al. Reductions in use of colchicine after FDA enforcement of market exclusivity in a commercially insured population. J Gen Intern Med 2015;30:1633–1638.
A study in rabbits found that whole autumn crocus corm powder at a dose of 2.5 mg/kg/day was as effective as allopurinol for lowering serum uric-acid levels, an effect not seen with isolated colchicine. 16 There are other pseudoalkaloids in autumn crocus in addition to colchicine, including colchicoside and 3-demethylcolchicine, which have shown interesting effects in vitro. 17 –19 The semisynthetic drug thiocolchicoside has been approved in some countries as a muscle relaxant, which has proven to be effective for treating low-back pain and other similar problems. 20 The semisynthetic colchicine-based drug demecolcine is used to treat some cancers. Another Colchicaceae family, colchicine-containing herb is Gloriosa superba (flame lily), which is native to Asia and Africa. Crude extracts of this herb have been shown to treat pancreatic cancer in mice. 21 Flame lily is also used to treat gout in crude form. 22 All of this suggests the potential of other aspects of autumn crocus in addition to its colchicine content for patients with gout. There is a need to avoid treating autumn crocus with such reductionism if its true potential is to be realized. These facts also support that crude autumn crocus extracts have a place in medicine, although this needs to be defined better in modern clinical trials.
The U.S. Pharmacopeia, in the late 1800s and early 1900s, included a 1:10 wt:v tincture of colchicum seed, extracted using 55% ethanol. The recommended dose was 10–30 minim (1–2 mL) every 4 hours until pain was relieved or nausea/mild purgation occurred. It is now more common to use a tincture of the corm, 1:5 wt:v, at a dose of 3–5 drops twice per day (or less if diarrhea or vomiting occur). This tincture should be used with great caution, if at all, in patients with renal failure and bone-marrow damage. There is no known antidote for autumn crocus or colchicine overdose.
Colchicine is a CYP3A4 and Pgp substrate. Concomitant use with CYP3A4 inhibitors (such as the antibiotic clarithromycin or grapefruit) can lead to significant increases in absorption of colchicine and death unless the dose is decreased. 23 It is unknown to what degree this causes problems with whole autumn crocus, but caution is warranted. Grapefruit could possibly be used intentionally to reduce colchicine or autumn crocus use, but the exact doses needed to achieve this have not been determined.
Antigout C Foods: Celery, Cherry, and Coffee
Another food/medicine that has proven very helpful clinically for patients with gout is common celery (Apium graveolens). This Apiaceae family vegetable is also known as a diuretic and inflammation modulator. Sadly, it has received little research attention. Phthalides, furanocoumarins, and terpenoids are believed to contribute to this food's clinical activity. Celery extract inhibited xanthine oxidase in vitro in one study, and celery's prominent flavonoid constituent luteolin did the same in another. 24,25 In mice treated with doxorubicin, celery root and leaf juice reduced xanthine oxidase. 26 Celery was historically used as a diuretic, and so might simultaneously increase urinary excretion of uric acid while inhibiting its synthesis. A traditional Uighur formula known as Karapxa Decoction, which contains primarily celery root and seed along with Cuscuta chinensis (dodder) seed, Cichorium glandulosum (chicory) root and seed, and Foeniculum vulgare (fennel) fruit was shown to inhibit xanthine oxidase and reduce serum uric acid in mice with induced gout. 27
The current author became aware of this property of celery after hearing the esteemed herbalist and retired scientist from the U.S. Department of Agriculture, James Duke, PhD, openly discussing how he was able to stop using medication for his gout because he used celery. Subsequently, many patients with gouty arthritis or uric-acid kidney stones have been able to decrease or eliminate these problems by eating 3–5 stalks of celery a day. Clinical trials are warranted.
Celery is generally extremely safe. There is a low risk of photodermatitis in patients with very light skin and high sun exposure. Some patients are supersensitive to this problem and will already know it from getting rashes just brushing up against plants in the Apiaceae family. Using sunscreen and wearing protective clothing while avoiding direct sun can help prevent this reaction in sensitive patients.
Back in 1950, a report was published showing that patients with gout who ate 0.5 lb of fresh, canned, or frozen (but not sweetened) cherries daily had lower serum uric-acid levels and fewer acute gout attacks. 28 Based on this single case series, cherries became a popular gout treatment in alternative medicine circles. It was not until 2003 that the next published report was published. In this study, 10 healthy women ate 2 servings of 280 g (∼ 8 oz) of sweet Bing cherries after an overnight fast. 29 Average serum uric-acid levels fell in these women over the 5 hours after cherry consumption to a level that was significantly below baseline. Uric-acid levels did not fall in historical control subjects who consumed grapes, strawberries, or kiwi at similar or higher amounts. This study is of dubious relevance to patients with gout, but is important, as many internet sites claim that only tart cherries are worthwhile, while this study showed clearly that sweet cherries produced activity (see Two Types of Cherries).
In 2007, Naomi Schlesinger, MD—then chief of the division of rheumatology and connective tissue research at Robert Wood Johnson Medical School in New Brunswick, NJ—and colleagues published an abstract describing a randomized trial of tart cherry juice concentrate. 30 Subjects took either 1 tbsp of tart cherry juice concentrate twice daily or pomegranate concentrate at the same dose. After 4 months of treatment, the subjects in the cherry-juice group had a significant reduction in acute gout attacks, compared to what occurred in the control group. Fully 55% of the cherry group had no gout attacks and were able to discontinue use of nonsteroidal anti-inflammatory drugs (compared to none of subjects in the control group). This research was funded by the maker of the cherry juice product, FruitFast/Brownwood Acres of Eastport, Michigan. In vitro, Schlesinger reportedly found that the cherry juice inhibited inflammatory compounds produced in response to uric-acid crystals. The researchers did not find any lowering of serum uric acid. The lack of full publication of these results requires a good deal of skepticism about their validity.
This same doctor and other researchers subsequently published information about retrospective studies suggesting that tart cherry juice concentrate reduced gout attack frequency without reducing serum uric acid levels. 31,32 In vitro work from Dr. Schlesinger's laboratory suggested that cherry juice may work by inhibiting interleukin-1 production by white blood cells in response to uric acid. 33 In most cases, these studies were not presented in detail but only in abstracts, limiting the ability to assess their methodological rigor.
A cross-sectional study of 633 American adults with gout conducted via the internet found that self-reported intake of cherries reduced the risk of a gout attack by 35% compared to no intake, and intake of cherry extract conferred 45% reduction in risk compared to no intake. 34 Respondents who reported allopurinol use along with cherry intake had a 75% reduction in gout attacks, compared to respondents not taking either. A similar internet study of 293 American adult visitors to the Gout and Uric Acid Education Society website found a correlation between self-reported cherry use and lower numbers of acute gout flares. 35
None of the research on cherry products for gout is sufficiently rigorous to determine if these products are effective. Given cherry's incredible safety, however, most patients will have little to lose other than money from trying it. This is particularly indicated if other therapies are not working.
Coffee (Coffea arabica), from the Rubiaceae family, has been studied extensively for coffee's effects on gout. A meta-analysis of eleven epidemiologic studies concluded that, despite having no effect on serum uric-acid levels, coffee consumption reduced the incidence of gout significantly in a dose-dependent manner. 36 A separate analysis of nine epidemiologic trials found that coffee did lower serum uric acid, although it took substantially more to do so in women than men (4–6 cups versus 1–3 cups, respectively). 37 This analysis also found an inverse relationship between intake of coffee and incidence of gout. Caffeine does not seem important to the antigout effects of coffee, as decaffeinated coffee was as effective as caffeinated coffee in these studies. In vitro, an aqueous extract of roasted coffee beans inhibited xanthine oxidase and crypto- and neochlorogenic lactones were found to be largely responsible for this activity. 38 These compounds are isomers of chlorogenic acid, an abundant lignan derivative found in green coffee, formed principally during roasting. More research is needed to determine coffee's mechanism of action, and randomized trials are also warranted to assess the clinical role of coffee fully in preventing and treating gout.
Chinese Herbal Formulas
A combination of herbs known as Chuanhu Anti-Gout Mixture (CAGM) has been studied in at least two clinical trials in patients suffering from podagra. The complete set of herbs in this formula could not be identified, but Lonicera japonica (Japanese honeysuckle, rěn dōng téng) stem, Polygonum cuspidatum=Fallopia japonica (Japanese knotweed, hǔ zhàng) root, whose Mandarin Chinese name translates literally as the evocative “tiger sticks,” and Dioscorea nipponica (Japanese yam, chuān shān long) rhizome are three of the apparently nine herbs included in CAGM.
In one double-blinded trial, 176 patients with acute gouty arthritis were randomized to 250 mL daily of a liquid extract of CAGM or 0.5 mg of colchicine b.i.d. 39 In each group, a placebo of the alternative medicine was also given. All patients were instructed to eat a low purine diet and to drink 2–3 L of water daily, given 1 g sodium bicarbonate t.i.d. to alkalinize the urine, and treated with 60 mg of etoricoxib q.d. for acute pain. After 12 weeks of treatment, recurrence of pain was no different between the groups. Acute joint pain was significantly less in the CAGM group, compared to what occurred in the colchicine group, while reduction of erythema and improvement in function of the affected joint was the same between these groups. Significantly more patients in the colchicine group suffered adverse effects than the patients in the CAGM group. Only 2 patients in the CAGM group dropped out of the trial because of adverse effects (diarrhea, bitter taste), whereas 8 patients in the colchicine group dropped out (diarrhea, liver damage). A similar clinical trial (reported in English only as an abstract) with 144 patients resulted in the same conclusions. 40
Èr Miāo Sǎn (Two Marvel Powder), containing 9–12 g of Phellodendron amurense (Amur corktree, huáng bǎi) bark and 6–9 g of Atractylodes chinensis (black atractylodes, cāng zhú) prepared root, is a traditional formula used to treat gout in Chinese medicine. This formula is often mixed with Zingiber officinale (ginger) juice while it is being prepared. It was first documented in Dàn Xī Xīn Fǎ (Essential Teaching of Zhu Danxi) written by Zhū Dān-Xī in 1481. * The formula was traditionally prepared as a decoction (and would be then called Èr Miāo Wán, Two Marvel Decoction), with the amounts cited above being divided into 3 doses per day in water.
In a mouse model of gout, Two Marvel Decoction was as effective as allopurinol for lowering serum uric acid. 41 The formula and Amur corktree alone inhibited xanthine oxidase, albeit not as potently as allopurinol, while black atractylodes had no such effect. This suggests that this herb has other effects—in addition to inhibiting xanthine oxidase—that contribute synergistically to a superior clinical effect. Two Marvel Powder, but not its ingredients in isolation, inhibited a range of inflammatory pathways relevant to gout in vitro. 42 A study in vitro found that the alkaloids berberine and palmatine and the glycoside obaculactone accounted for much of the xanthine oxidase-inhibiting effects of Amur corktree. 43
A combination of Two Marvel Powder and Sì Wù Tāng (Four Substances for Women) formula, containing Rehmannia glutinosa (Chinese foxglove, shú dì huáng) prepared root, Paeonia lactiflora (white peony, bái sháo) root without bark, Angelica sinensis (dong quai, dāng guī) prepared root, and Ligusticum striatum (Chinese osha, chuān xiōng) root, were studied in mice with induced gout. 44 The two formulas combined were superior to Four Substances for Women by itself for lowering serum uric acid and improving kidney function. The combination of the two formulae also seemed particularly effective for upregulating organic ion transporters 1 and 3 in the kidney, both of which are crucial in excretion of uric acid.
Two clinical studies that were published in Chinese used formulas that contained part or all of Two Marvel Powder. Details were not available, and these reports were presented only as parts of a systematic review of Chinese herbal formulas for gout. 45 One study compared Two Marvel Powder with several additional herbs to colchicine and allopurinol in 216 patients with gout for 30 days and found both approaches equally effective for treating acute attacks. The other study looked at Two Marvel Powder with yet a different set of additional herbs in 76 adults with gout, compared to colchicine, allopurinol, and indomethacin, this time taken for 7–21 days. Again, these approaches were similarly effective for resolving acute attacks, but, overall, both treatment groups had far lower efficacy than reported in the other trial. This provides some preliminary evidence that Two Marvel Powder and various combinations with it are clinically effective. More rigorous trials are warranted. The meta-analysis cited found a total of 17 trials of herbal formulas for gout, and concluded that they are similar in efficacy to antigout drugs but with far fewer adverse effects. The extreme variability between these herbal formulas and study methodologies calls the validity of such a meta-analysis into question, but it appears that there is preliminary support for Chinese herbs for treating patients who have gout.
Sì Miào Wán (Four Marvels Teapills) is a variant of Two Marvel Powder first documented in 1904 in the book Chéng Fāng Biàn Dú (Convenient Reader of Established Formulas) by Zhāng Bǐng-Chéng. Four Marvels Teapills contain Two Marvel Powder plus Achyranthes bidentata (ox knee, niú xī) root and Coix lachryma-jobi var ma-yuen (Job's tears, yì yǐ rén) seed. In this formula, all the ingredients are generally combined in equal amounts and the dose is 6–9 g t.i.d. The formula can also be prepared as a decoction. In a clinical trial (blinding not described), 207 patients with gout having acute attacks were randomized to one of three versions of Four Marvels Teapills or indomethacin with benzbromarone, a xanthine oxidase–inhibiting drug little used in the U.S. 46 Symptomatic improvement was significantly greater in all the herbal formula groups, compared to the drug controls. All groups had significant declines in serum uric acid, compared to baseline; no group was superior to another in efficacy with respect to this parameter. This lends further evidence to the efficacy of Two Marvel Powder and the additional herbs included here.
Conclusion
Many herbal medicines and medicinal foods appear to be helpful or potentially helpful for patients with gout, both to prevent and treat attacks. Several of the most promising have been reviewed in this article. Other herbs showing promise in preclinical research are outlined in Table 1. Clearly, much more work needs to be done to fully develop herbs for gout, but the groundwork is in place.
Misidentified as Panax japlcus in the article, but no such species exists and this is fairly clearly a typographical error.
Tung YT, Lin LC, Liu YL, et al. Antioxidative phytochemicals from Rhododendron oldhamii Maxim. leaf extracts reduce serum uric acid levels in potassium oxonate-induced hyperuricemic mice. BMC Complement Altern Med 2015;15:423; cCheng LC, Murugaiyah V, Chan KL. In vitro xanthine oxidase inhibitory studies of Lippia nodiflora and isolated flavonoids and phenylethanoid glycosides as potential uric acid-lowering agents. Nat Prod Commun 2015;10:945–948; dWu XH, Yu CH, Zhang CF, et al. Smilax riparia reduces hyperuricemia in mice as a potential treatment of gout. Am J Chin Med 2014;42:257–259; eWu XH, Wang CZ, Wang SQ, et al. Anti-hyperuricemia effects of allopurinol are improved by Smilax riparia, a traditional Chinese herbal medicine. J Ethnopharmacol 2015;162:362–368; fLi S, Tang Y, Liu C, et al. Development of a method to screen and isolate potential xanthine oxidase inhibitors from Panax japlcus [sic] var via ultrafiltration liquid chromatography combined with counter-current chromatography. Talanta 2015;134:665–673; gLin WQ, Xie JX, Wu XM, et al. Inhibition of xanthine oxidase activity by gnaphalium affine extract. Chin Med Sci J 2014;29:225–230; hLiu LM, Cheng SF, Shieh PC, et al. The methanol extract of Euonymus laxiflorus, Rubia lanceolata and Gardenia jasminoides inhibits xanthine oxidase and reduce serum uric acid level in rats. Food Chem Toxicol 2014;70:179–184; iSong HP, Zhang H, Fu Y, et al. Screening for selective inhibitors of xanthine oxidase from Flos Chrysanthemum using ultrafiltration LC-MS combined with enzyme channel blocking. J Chromatogr B Analyt Technol Biomed Life Sci 2014;961:56–61; jChen GL, Zhu LR, Na S, Li L. Effect of total saponin of Dioscorea on chronic hyperuricemia and expression of URAT1 in rats [in Chinese]. Zhongguo Zhong Yao Za Zhi 2013;38:2348–2353; kChen Y, Chen XL, Xiang T, et al. Total saponins from Dioscorea septemloba Thunb. reduce serum uric acid levels in rats with hyperuricemia through OATP1A1 up-regulation. J Huazhong Univ Sci Technolog Med Sci 2016;36:237–242; lMurunikkara V, Rasool M. Trikatu, a herbal compound that suppresses monosodium urate crystal-induced inflammation in rats, an experimental model for acute gouty arthritis. Cell Biochem Funct 2014;32:106–114.
OAT, organic anion transporter; URAT, urate transporter.