
Abstract
Objectives:
Chronic, neuropathic pain is a severe physically and emotionally disabling condition that often responds poorly to standard pain treatment. Alternative and complementary treatment approaches may be useful. The current authors sought to investigate the potential efficacy of Accelerated Resolution Therapy (ART) for treating chronic neuropathic pain.
Materials and Methods:
Design: A prospective cohort pilot study was conducted. Setting: Sessions of ART were delivered by licensed mental health professionals at a public university in Florida. Subjects: Ten adult patients (mean age 64.5 years, 60% female) with chronic neuropathic pain received an average of 3.1 sessions of ART. Interventions: All patients were treated with ART, a mind–body psychotherapeutic approach that is evidence-based for treatment of psychologic trauma and depression. Outcome Measures: Self-reported measures of pain and comorbidities were obtained pre-ART, post-ART, and at a 1-month follow-up.
Results:
For 31 sessions of ART delivered, the mean patient rating on the 0–10 Subjective Units of Distress Scale was 6.8±2.1 at each session's beginning, compared to 2.9±2.0 at each session's end (t=7.91; P<0.0001). For the full treatment period, the mean score on the Pain Outcomes Questionnaire was 76.2±30.2 before ART versus 61.2±29.9 after ART (treatment effect size=0.66; P=0.07). Mean score on the Bodily Pain subscale of the Medical Outcomes Study Short Form–36 improved significantly from 34.5±20.1 before ART to 49.8±25.4 after ART (effect size=0.79; P=0.03). There were suggestions of improved mobility, emotional health, and sleep quality after treatment with ART, as well as reduced pain and improved energy/fatigue at the 1-month follow-up.
Conclusions:
While preliminary, results of this uncontrolled pilot study suggested that ART may be a useful treatment for chronic moderate–to–severe neuropathic pain. Future controlled studies are warranted.
Introduction
One in 15 Americans suffers with peripheral neuropathy, including 60%–70% of people with diabetes, 20%–50% of people with human immunodeficiency virus, and 30% of cancer survivors. 1 Approximately 30% of neuropathies are idiopathic. Neuropathic pain is among the most common symptoms of peripheral neuropathy, and is associated with increased disability, depression, sleep disturbances, and diminished quality of life (QoL). 2,3 Additional consequences of neuropathic pain on society include increased medical costs and loss of productivity. 4
Neuropathic pain is often severe and refractory to medical management. Pharmacologic management of neuropathic pain includes anticonvulsants and antidepressants as first-line therapies, and opioid analgesics may provide additional relief. 5 Few patients with neuropathic pain obtain adequate pain control with pharmacologic approaches, which often require multiple medications and frequent dose escalations, as well as causing intolerable side-effects. 6 While medications have the potential to control neuropathic pain, patients often experience excess sedation, weight gain, headaches, and cognitive difficulties that limit these patients' willingness to adhere to prescribed treatment regimens. These pharmaceuticals also affect physical and emotional functioning as well as QoL negatively.
Nonpharmacologic approaches to supplement pharmaceutical management are desirable because they have fewer side-effects, allow patients to participate actively in their pain management, and can enhance emotional well-being. 7 The efficacy of nonpharmacologic techniques for adjuvant use in neuropathic, nociceptive, and mixed pain syndromes has not been evaluated thoroughly. This lack of definitive evidence exists in the context of several nonpharmacologic approaches that have been explored for neuropathic pain. These approaches include interventions for alleviating sensory aspects of pain, such as transcutaneous electrical nerve stimulation 8 as well as some interventions for modifying the cognitive/emotional aspects of pain.
The underlying premise of nonpharmacologic mind–body therapies is that they offer considerable promise for potentially being able to alleviate painful neuropathy, 9,10 reduce symptom distress, improve function, and increase postural control. 11 –13 Catastrophic thinking, anxiety, and depression are common in people with neuropathy and are associated with increased pain 14 and symptom distress, 15 which can be responsive to mind–body therapies, such as mindfulness-based stress reduction, meditation, 10 yoga, 16 and guided imagery. 17 More conventional cognitive–behavioral (CBT) therapy has also been shown to decrease pain and interference in persons with diabetic neuropathy. 9 In aggregate, while some research supports the use of mind–body therapies for chronic neuropathic pain, the rigor and size of the studies to date are insufficient to support specific recommendations for clinical practice. 7 This represents an area in need of greater scientific inquiry.
Accelerated Resolution Therapy (ART) is a nonpharmacologic mind–body intervention that is typically delivered in just 1–5 sessions. It was developed in 2008, with formal research initiated in 2010, as a brief trauma-focused therapy for treatment of symptoms of post-traumatic stress disorder (PTSD). For treating PTSD, the ART protocol is delivered using the four core elements found in most A-level trauma-focused psychotherapies. 18 This includes a narrative element that is related to the trauma/distressing experience, in vivo and/or imaginal exposure, cognitive restructuring, and relaxation/stress modulation. Training in the Basic ART protocol includes theoretical and experiential components that are conducted over a 3-day period, with formal certification and additional information available through an established training 19 and professional organization. 20
From the research evidence amassed since 2010, ART is now classified as evidence-based for treating PTSD and depression, 21 –24 and, secondarily, has been shown to reduce pain and improve mobility associated with pain in veterans treated with ART for PTSD, the majority of whose description of pain was consistent with characteristics of neuropathic pain. 25 While this is intriguing, it is unknown if ART can be used to improve pain relief in persons with neuropathic pain who do not suffer from PTSD. This pilot study investigated the effects of ART on moderate-to-severe neuropathic pain and related comorbidities in community dwelling adults.
Materials and Methods
Sample and Setting
Participants were recruited from a peripheral neuropathy support group in West Central Florida. Individuals on a list-serv for the support group received an e-mail with information about the study. Persons attending support-group meetings were also given information about the study. Persons who expressed interest and met eligibility criteria according to self-reports were given appointments with a research assistant, wherein eligibility was verified and informed consent was obtained. Institutional review board protocol approval was obtained through the University of South Florida. Delivery of treatment with ART was conducted by 2 licensed mental health therapists at the University of South Florida, College of Nursing.
Eligibility for enrollment required: (1) history of neuropathic pain for 3 or more months; (2) average pain rating over the last week of 6 or higher on a 0–10 scale; (3) ability to read, write, and comprehend English; and (4) currently under the care of a neurologist, primary care provider, or pain-management specialist. Exclusion criteria included: (1) prior surgery or invasive medical procedure in the past 6 weeks; (2) having experienced major physical trauma in the past 6 weeks; (3); having an implanted pain device (nerve stimulator, pain pump, etc.); or (4) having severe depression. Depression was considered as severe if all of the following conditions were met: (A) a score of 30 or higher on the Centers for Epidemiologic Study–Depression (CES–D) scale; (B) a positive response to item #6 on the CES–D (“I felt depressed”) with a rating of “3” corresponding to “most or all of the time”; and (C) a score of 7 or higher on the 0–10 scale for the specific depression question on the Pain Outcomes Questionnaire (“How would you rate your feelings of depression today?”).
Data Collection
After consent, determination of eligibility, and enrollment into the study, a battery of self-report questionnaires was completed by each participant. Prior to the first ART session, each participant completed a brief demographic and medical history form, the Pain Outcomes Questionnaire (POQ)–Short Form to measure key domains of pain, 26 the CES–D to measure depressive symptoms, 27 36-item Short Form Health Survey (SF–36) to measure mental and physical health-related QoL (HRQoL), 28 and the Pittsburgh Sleep Quality Index (PSQI) to measure sleep quality. 29 The same instruments were completed 3–5 days following completion of ART treatment and at a 1-month follow-up. In addition, participants reported their levels of distress on a 0–10 scale at the beginning and end of each ART session, using the Subjective Units of Distress Scale (SUDS).
Clinical Intervention
Detailed descriptions of the ART protocol for treating psychologic trauma have been published. 21,22,30 In brief, ART first uses the technique of imaginal exposure to elicit physiologic reactions associated with patient recall (verbally or nonverbally) of a traumatic/distressing experience. As reactions are invoked, the patient is directed to focus attention on the specific physiologic reaction(s) while laterally performing smooth pursuit eye movements. 31 These movements are achieved by tracking the clinician's hand, which oscillates from left to right at a short distance from the patient's eyes. After two full courses of processing (reducing) physiologic reactions that are induced by imaginal exposure, the technique of imagery rescripting 32 is used. In this phase, the patient is directed to imagine a positive way in which he or she prefers to recall the experience, including emphasis on “replacing” negative images with positive images upon recall. This technique is based on the process of memory reconsolidation, which allows for “adding” positive material to the recall of negative past experiences. 33
Given that the patients might or might not have had histories of psychologic trauma, a first step was to inquire whether each patient could identify any traumatic memories that related specifically to his or her pain. If so, these memories would be selected for use of imaginal exposure and imagery rescripting, as described above. If no pain-related traumatic memories were identified, the patient was directed to imagine a “typical” (distressing) day, including the circumstances and time of day in which shifts in pain tended to occur (e.g., after physical activity or stressful situations). In essence, this very distressing typical day and circumstances of heightened pain would serve as a “trauma” to be treated with the ART protocol. The goal was to alter the visual and sensory recollection of the typical day by the use of imagery rescripting. Pictoral metaphors could be suggested by the clinician, such as having the patient imagine being tied up with ropes to describe how it felt or having the patient imagine being pricked by pins. The sensations (neuropathic) would be processed with ART's eye movements, and then the patient would be asked to correct (change) the picture.
One patient in the current study, an aeronautical engineer, imagined his nervous system as circuitry and then imagined turning neurons up or down based on pain levels.
Each ART session ended by having a patient visualize going over a bridge and leaving his or her pain behind. In addition, for potential maintenance effects, patients were taught how to perform sets of eye movements on their own as a way to minimize pain sensations and anxiety.
Instruments
Pain
The 20-item POQ–Short Form 26 was used to measure pain. It is a reliable and valid instrument that contains 19 primary pain items rated on an 11-point (0–10) Likert-type scale and 1 demographic question. In addition to a total pain score, six subscale scores can be calculated that correspond to pain intensity (1 item), pain-related impairment in mobility (4 items), pain-related impairment in performing activities of daily living (ADLs; 4 items), sense of impairment in activity and energy levels (3 items), dysphoric affect and associated symptoms (5 items), and pain-related fear and avoidance (2 items).
Depressive symptoms
Depressive symptoms were measured using the 20-item CES–D. The CES–D 27 is a widely used 20-item scale that has proven useful both as a screening instrument to detect individuals at risk for depression and to measure symptoms of depression. The CES–D has demonstrated impressive reliability, validity, sensitivity, and specificity. 34
Sleep quality
The 15-item PSQI 29 was used to measure sleep quality. A global PSQI score >5 has a diagnostic sensitivity of 89.6% and a specificity of 86.5% (κ=0.75) for distinguishing good sleepers from poor sleepers. Internal consistency reliability has been estimated to range from 0.77 to 0.81.
HRQoL
The 36-item SF-36 is an established, widely used measure for HRQoL. This scale includes 8 subscales that are scored from 0 to 100, with a higher score indicating more favorable health status. Estimates of internal consistency reliability range from 0.62 to 0.94. Factor analysis indicates two dimensions comprised of physical and mental health status and that account for 82% of the reliable variance. 35
Statistical Analysis
Descriptive statistics for demographic and clinical characteristics are presented in this article as means±standard deviation (SD) for continuous variables and as percentages for categorical variables. Pre- and post-treatment outcome scores for selected measures were compared, using a paired t-test with standardized effect sizes for outcomes calculated as:
([mean before ART−mean after ART]/SD of treatment difference scores). 36
P-values<0.05 were considered to be statistically significant.
Results
The mean age of the 10 study participants was 64.5±7.3 years, 60% were female, all were white, non-Hispanic race/ethnicity, and 70% were married. The mean years of education was 15.9±2.4, and 30% of participants were employed full-time. Three participants (30%) had idiopathic neuropathy, 2 (20%) had neuropathy as a result of previous chemotherapy, 2 had diabetic neuropathy (20%), 1 (10%) had fibromyalgia, 1 (10%) had Charcot-Marie-Tooth (a hereditary cause of neuropathy), and 1 (10%) had neuropathy as a result of long-term side-effects of radiation therapy. Thus, the etiology of neuropathic pain was heterogeneous in this pilot sample.
Clinical Presentation at Entry Compared to 1-Month Follow-Up After ART
According to study inclusion criteria, all participants reported having histories of neuropathic pain for at least 3 months and an average pain rating over the past week of 6 or higher on a 0–10 scale. Self-report prevalence of medical conditions included muscle or bone problems (10%), neurologic problems (80%), diabetes (20%), high blood pressure (40%), hearing problems (20%), and vision problems (30%). Prior treatment history, in addition to pharmacotherapy, was highly variable and included acupuncture (30%), massage (50%), physical therapy (60%), and yoga (30%). In aggregate, 70% of participants reported previous use of nonpharmacologic (nondrug) treatment for pain control. The mean number of prescription medications being taken at entry was 4.4±3.2.
For the 10 participants, types of prescription medications associated with pain control were distributed as follows prior to treatment with ART: 50% were taking anticonvulsants; 30% were taking opioid analgesics; 20% were taking antidepressants; and 10% were taking sleep medications. Thirty percent were not taking any medications specifically for treatment of pain or pain-related symptoms. At a 1-month follow-up after ART, 1 person had discontinued opioids and anticonvulsants, another had discontinued two antidepressants, and a third had started on a prescription sleep medication. No other changes in neuropathic pain related medications were reported.
Intervention Delivery
The 10 participants received a mean of 3.1±1.5 sessions of ART (range: 1–5) delivered by 2 clinicians who were proficient in ART (Y.H. and L.R.) during the period July–October, 2015. The mean duration of treatment was 24.5±25.1 days. For the 31 sessions of ART delivered, the mean rating on the 0–10 SUDS at the beginning of the session was 6.8±2.1 (range: 3–10). This compared to a significantly reduced mean SUDS rating at the end of the ART session (mean: 2.9±2.0; range: 0–7; P<0.0001). Thus, the participants reported, on average, acute positive reductions in distress after receiving one session of ART.
Acute Outcome Results
The mean score on the POQ at study entry was 76.2±30.2 and was reduced by an average of −15.0±22.8 points after treatment completion with ART (Table 1; Fig 1A). This corresponded to a “medium” effect size of 0.66 that approached—yet did not achieve—statistical significance (P=0.07). As a second measure of pain, the mean score on the Bodily Pain subscale of the SF-36 increased significantly from 34.5±20.1 before ART to 49.8±25.4 after ART (effect size=0.79; P=0.03; Table 1, Fig. 1C).
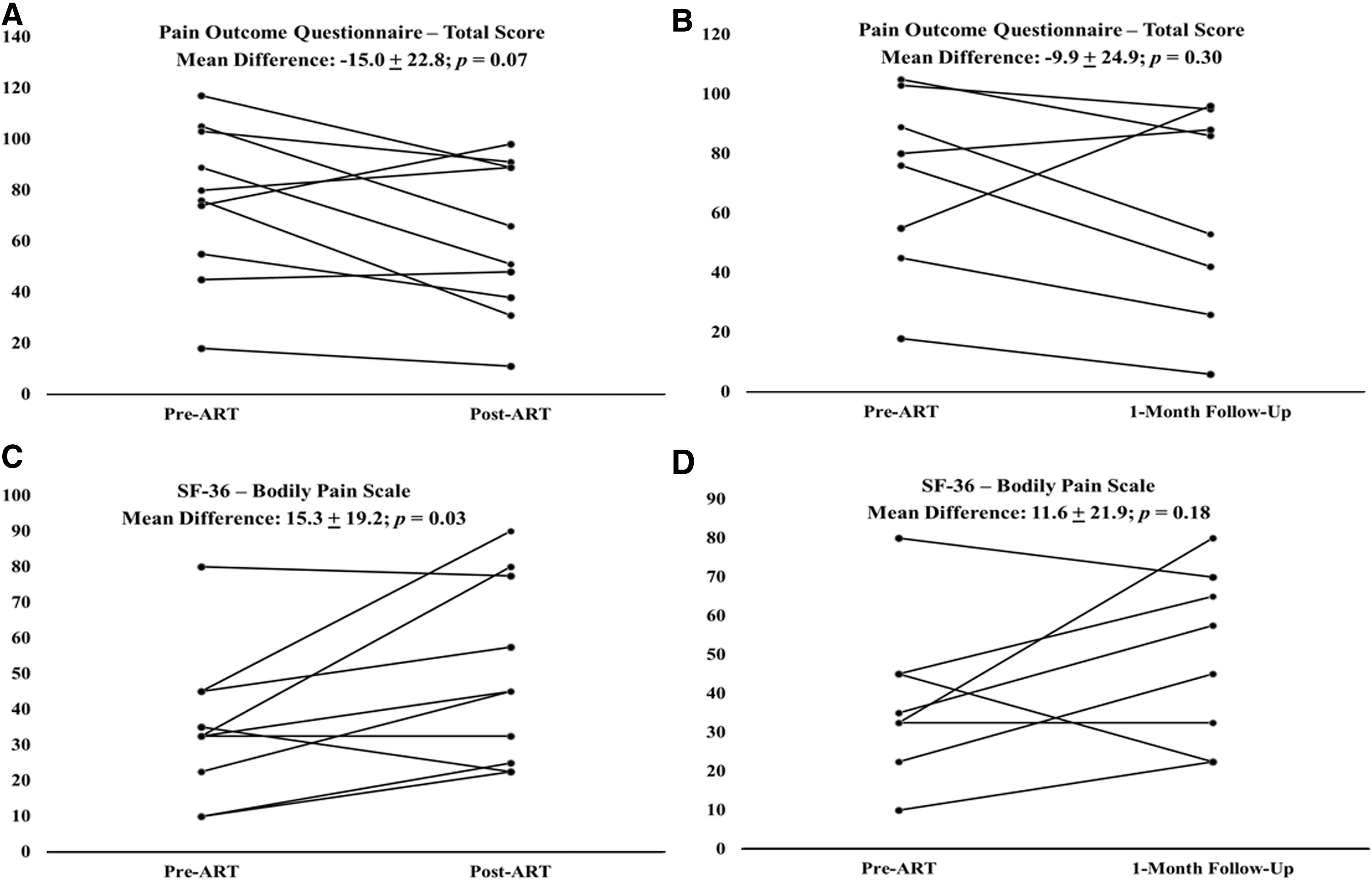
Plot of pain treatment response before and after ART ([A] Pain Outcome Questionnaire; [B] Bodily Pain scale of the SF-36 instrument) and before ART and at 1-month follow-up ([C] Pain Outcome Questionnaire; [D] Bodily Pain scale of the SF-36 instrument). Horizontal lines represent the treatment response of individual patients.
ART, Accelerated Resolution Therapy; SD, standard deviation; POQ, Pain Outcomes Questionnaire; ADLs, activities of daily living; CES–D, Centers for Epidemiologic Study–Depression; SF–36, Short Form–36; PSQI, Pittsburgh Sleep Quality Index.
Of note, the mean SF-36 Bodily Pain Scale score of 49.8 after treatment with ART was essentially equivalent to the age-standardized mean of 50 in the general population. There was also significant treatment improvement reported for the Mobility subscale of the POQ (effect size=1.20; P=0.005). In terms of acute response, virtually all effects reported were in the direction of improved symptom status, with measures of ADLs, physical functioning, emotional role limitations, aggregate mental health, sleep duration, and sleep latency all suggestive of medium-to-large positive effects.
Follow-Up Results
Eight of the 10 participants (80%) provided 1-month follow-up data. For these participants, the mean pre-ART score on the POQ of 76.2±30.2 was nonsignificantly reduced to 61.5±34.7 at the 1-month follow-up (effect size=0.59; P=0.30, Table 2, Fig. 1B). A significant mean reduction on the POQ pain subscale was reported from pre-ART (6.5±1.3) to 1-month follow-up (4.6±1.9; effect size=0.92; P=0.04), and there was also a trend suggestive of improved mobility at 1-month follow-up (effect size=0.71; P=0.08). One-month follow-up results on the SF-36 were more variable, with an apparent significant improvement in reported energy/fatigue (effect size=1.20; P=0.01), yet little-to-no effect for the remaining subscales with the exception of a nominal reduction in bodily pain (effect size=0.53; P=0.18; Table 2, Fig. 1D). There was also a nonsignificant suggestion of improved sleep quality at 1-month follow-up (effect size=0.69; P=0.09).
ART, Accelerated Resolution Therapy; SD, standard deviation; POQ, Pain Outcomes Questionnaire; ADLs, activities of daily living; CES–D, Centers for Epidemiologic Study–Depression; SF–36, Short Form–36; PSQI, Pittsburgh Sleep Quality Index.
Discussion
This is the first study to suggest evidence of potential benefits of delivery of ART specifically for reduction of pain and pain-associated symptoms in a sample of 10 individuals with chronic moderate-to-severe neuropathic pain. The current study results indicated that a course of one to five sessions of ART appears to reduce pain and mitigate emotional distress in the short-term and that some of these apparent positive effects may continue for at least 1 month following treatment. As an exploratory study, it was generally underpowered to detect modest, yet clinically important, statistically significant effects of ART. Nonetheless, medium-to-large effect sizes were observed consistently in the direction of improved symptom status.
Effects on Pain, Pain-Associated Symptoms, and QoL
Compared to a previous study of ART, wherein reductions in pain in veterans with PTSD were observed, 25 the results in the broader (non-PTSD) setting of chronic neuropathic pain suggested similar improvements in pain intensity, in pain-related impairment in mobility, and in dysphoric affect and associated symptoms subscales of the POQ, as well as in overall POQ scores, following treatment with ART. Consistent with a 2015 Cochrane review, 7 few studies evaluating any type of psychologic treatment effects on neuropathic pain were identified in the current authors' review of the literature. However, a Cochrane review of psychologic treatments for chronic pain described some immediate reductions in pain while using CBT, that, unfortunately, were not sustained at follow-up. 37
ART through the use of imagery rescripting has the theoretical potential to alter negative emotions associated with pain permanently. Specifically, it has been theorized that, when remembering something that is highly emotional (i.e., pain in the current study), the memory is likely to be in the form of an image. 38 The memory reconsolidation that is sought with the imaginal exposure and imagery rescripting components of the ART protocol are believed to be sustained and perhaps permanent in nature. 39 Whether or not this memory reconsolidation process may affect long-term neuropathic pain is unknown.
Article: Accelerated Resolution Therapy: Program Description
Website:
Article: What is ART?
Website:
Article: Treating Trauma
Website:
To the current authors' knowledge, there is no other psychotherapy research indicating reductions of pain-associated symptoms and QoL in persons with neuropathic pain who do not have PTSD. ART and other psychologic therapies have been theorized to reduce neuropathic pain-associated symptoms and improve QoL, in part, because of the strong relationship between pain and emotional distress. 40 Chronic neuropathic pain influences every aspect of QoL. Depressed mood, physical disability, social isolation, and difficulty with sleep are just some of the physical and emotional issues that persons with chronic painful peripheral neuropathy face, 41 and reductions in one or more of these symptoms may lead to improvements in other symptoms. Interventions, such as ART, that address psychologic aspects of pain, warrant continued investigation so that patients with neuropathic pain could have more treatment options available.
Strengths and Limitations
The results of this exploratory study suggest a need for future studies to evaluate efficacy of ART as an integrative therapy for persons with neuropathic pain. The small sample size, lack of racial and ethnic diversity, and lack of a control group limit generalizability of these findings. In addition, given the exploratory nature of the study, no statistical correction was made for multiple comparisons. Future studies should not only address these limitations but should also include an attempt to identify individual characteristics that are associated with response to treatment with ART. As reflected in the current study population, persons with neuropathic pain comprise a diverse group, and responses may vary based on individual differences, demographic characteristics, symptom severity, or underlying causes of the neuropathy.
Participants in this study reported acute, substantial decreases in self-reported distress after each treatment session. The changes in pain and other symptoms that were observed could largely be a result of distress reduction associated with ART. Previous research incorporating biologic markers of stress responses along with self-reported symptoms has demonstrated reductions in stress markers in association with nonpharmacologic therapies. 42 Future studies should incorporate biologic and physiologic measures to help explain possible underlying mechanisms for improvements in symptoms.
Conclusion
This exploratory study suggests potential benefits of ART, an innovative psychologic treatment that, until now, has only been evaluated in persons suffering from severe emotional trauma and comorbid moderate-to-severe pain. Current pharmacologic approaches to management of peripheral neuropathy are inadequate to address the complex physical and psychologic burdens of pain and disability. Evidence-based integrative therapies to reduce pain and other symptoms in people with peripheral neuropathy are needed. Findings from this preliminary study suggest immediate and 1-month reductions in pain that warrant further study.
Footnotes
Author Disclosure Statement
No external funding was provided for the conduct of this study. Ms. Rosenzweig is the developer of Accelerated Resolution Therapy (ART) and has a commercial interest in its dissemination. ■