
Abstract

Introduction
Acupuncture has the ability to modulate nervous system processes to treat chronic pain conditions. 1 Part of the benefit of acupuncture as a treatment modality is its potential to encompass holistic person-centered therapy. 2 This is critical for the treatment of chronic pain because pain is such a multidimensional experience. 3
Chronic pain is defined as pain that persists past normal healing time and presents for more than three months. 4 It affects sensory and emotional perception, particularly if previous injuries and experiences influence affective and cognitive susceptibilities to pain. 1,3,5 From a medical perspective, chronic pain is hallmarked by central sensitization. 6 Central sensitization is a mechanism whereby repeated bombardment of peripheral pain-related (nociceptive) stimuli causes spinal activity-dependent synaptic changes, generating post-pain hypersensitivity. This phenomenon indicates dysregulation of normal inhibition and facilitation of nociception, which can potentially lead to persistent neuroplastic reorganization and adaptation of somatosensory, motor, autonomic, affective, and cognitive functions. 3,5,6
Central autonomic control involves all levels of the neuroaxis, from the spine and brainstem to the forebrain, and there is extensive network overlap where integration in pain perception and autonomic function are shared to enable subtle adjustment to executive and attentional functions. 7 Examples include reduction of central hypothalamic β-endorphin production in chronic pain. This endogenous opioid has a regulatory role, including autonomic function, as well as mediating pain and nociceptive inhibitory systems. 2
As a consequence of these mechanisms, chronic pain causes a disturbance in the normal homeostatic ability of the body to regulate the balance between autonomic nervous system (ANS) sympathetic and parasympathetic control. 7 Such disruption can be measured through changes in heart rate variability (HRV), which may be decreased in chronic pain. This signifies a probable decrease in parasympathetic drive in those with chronic pain in comparison with healthy individuals. Reviews of chronic pain acupuncture studies present multiple trials where HRV increases are demonstrated after acupuncture, particularly when parasympathetically related treatments are provided. 7 –9
The sympathetic nervous system typically suppresses pain. However, even subtle changes in pathophysiology can dramatically change sympathetic outflow. Normally, norepinephrine, the primary sympathetic postganglionic neurotransmitter, inhibits pro-inflammatory cytokine activity. However, chronic inflammation can induce dendritic cells in the skin to express α1-adrenoreceptors, which in turn increases production of pro-inflammatory cytokines. 10 Thus, sympathetic dysfunction can increase inflammation, swelling, and pain by activating, increasing the numbers of, and increasing responsiveness of immune cells. 10 This may further contribute to nociceptor sensitization via β2-adrenergic receptors on skin cells, which may release prostaglandins, nerve growth factor, and other neurogenic inflammatory mediators, thus potentiating sympathetically maintained pain states. 10
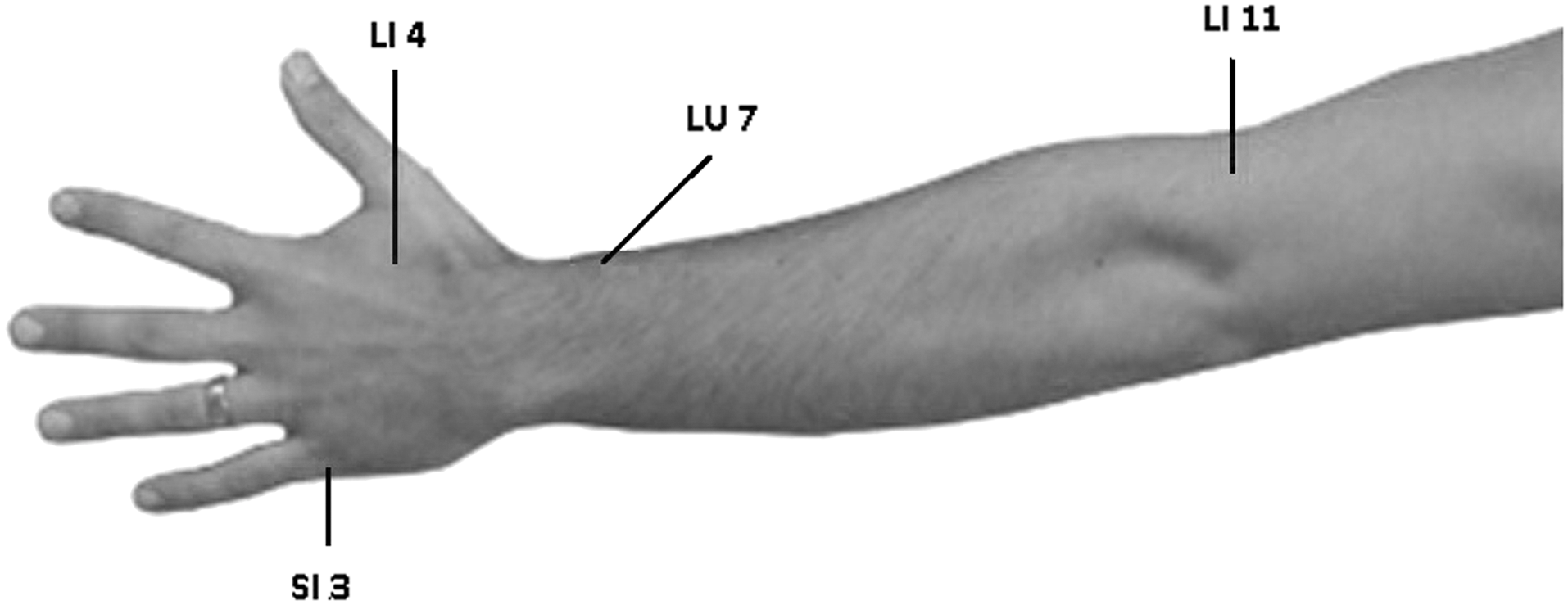
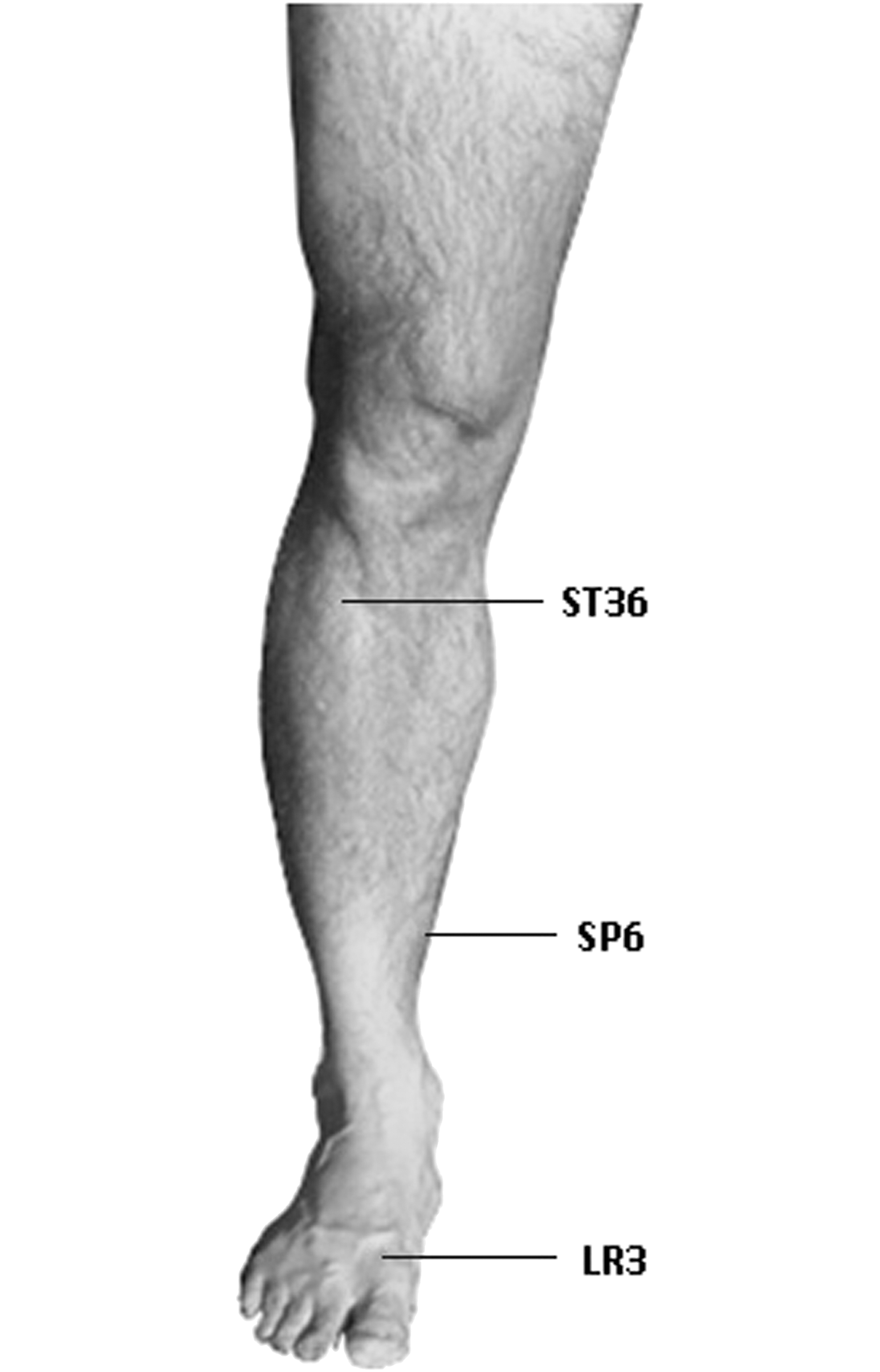
In sympathetically mediated pain, the treatment objective is to decrease and deplete noradrenaline at the postganglionic sympathetic axon. 11 In studies of acupuncture and chronic pain, ANS-mediated reductions in heart rate and blood pressure are demonstrated, suggesting shifts in sympatho-vagal balance toward vagal predominance. 12 Acupuncture needling at points in the periphery, which have a neural relationship to autonomic outflow, such as LI4, LR3, SP6, and SI3 (Figs. 1 and 2), 13 along with points near lymphatic and vascular structures can have a beneficial effect on the ANS. 14,15 High-intensity manual or electrical stimulation of acupuncture needles increases sympathetic outflow to tissues supplied by that particular segment in the short term, followed by a longer-term decrease in outflow. Low-intensity stimulation downregulates sympathetic activity, encouraging a parasympathetic state. 14,15
Case Presentation
An 85-year-old female fractured her left distal radius. She was referred for rehabilitation eight weeks after conservative management in a plaster of Paris splint. She was now wearing a supportive brace over the wrist and hand, but was continuing to suffer from pain (4/10 Visual Analogue Scale [VAS] at rest and up to 8/10 VAS after activity). The pain was allodynic in nature, so she was reluctant to use the wrist and hand. The hand and distal forearm were swollen, but not discolored, with normal skin temperature. She was medically well, but had short-term memory loss, and was not regularly taking the amitryptiline and analgesic medication prescribed by her physician.
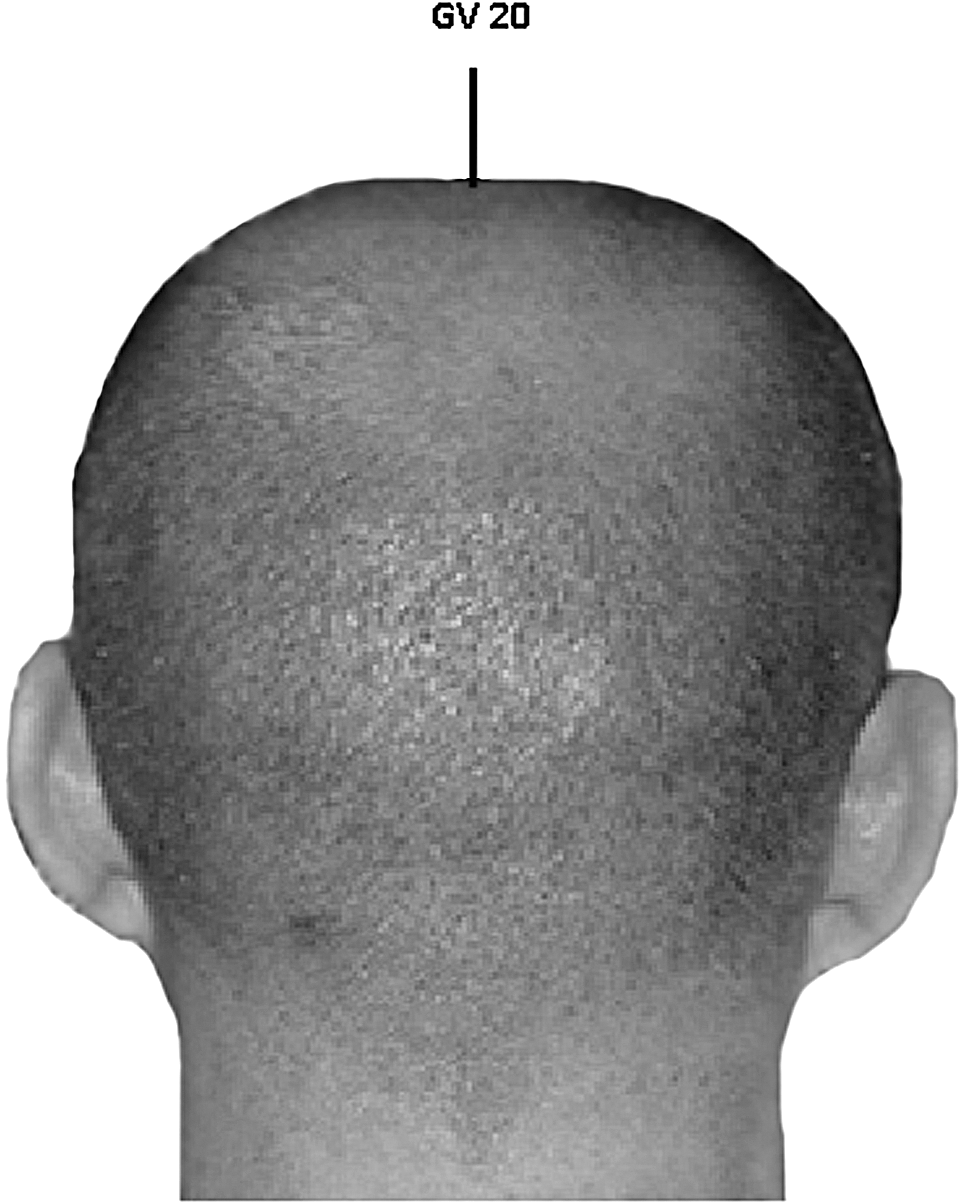
Treatment objectives were to reduce pain and improve movement, strength, and functional ability of the wrist and hand. This included acupuncture on the left side at LI11, LI4, and LU7 (Fig. 1) with 0.25 mm×30 mm needles for 20 minutes, with 5 second needle bidirectional rotation (de qi) after needle insertion and, at 10 minutes, exercise, soft-tissue massage, and gentle manual therapy. After four treatments, range of motion and functional activities had improved. Pain was now 5/10 at worst and 1/10 at best. Weaning her reliance off the wrist brace was difficult, and exercises were progressed. Mechanical allodynia was still present over the distal radius, swelling had reduced, but grip strength was not improving. She was referred for further assessment and was found to have a mal-union of the radial fracture, with some bony sclerosis probably from non-use. A week later, the patient presented with swelling. The forearm, wrist, and hand were warm to the touch, and allodynia and hyperalgesia had increased, with VAS 8–9/10. At this stage, touching the affected forearm was not an option for treatment. Acupuncture was continued, but to the right side at LI11, LI4, and LU7, and to the left side at ST36 (Figs. 1 and 2) and GV20 (Fig. 3) for 25 minutes, with de qi twice each needle. All points were sterile swabbed and were left for two minutes to dry before needling. Four days later, the difference in presentation was remarkable. The skin temperature was normal, the swelling had reduced, the pain had reduced to 4/10, and the patient allowed her hand and arm to be touched. The treatment was repeated, adding in LI11 on the right. Suffice to say, acupuncture using autonomic points “turned” the presentation, pain quickly reduced, and rehabilitation of mobility and strength progressed to a functional status.
Auckland University of Technology
Private Bag 92006
Auckland
New Zealand
Phone: 64 9 473 5055
E-mail:
Discussion
The patient appears to have been heading down the path of developing a regional pain syndrome. Acute autonomic dysfunction is characterized by a change of skin color, temperature, and perfusion because of enhanced sensitivity of sympathetic postganglionic adrenergic receptors. 9 The acupuncture treatment mediated autonomic effects through needling points with a contralateral segmental neural approach to the condition to not exacerbate an autonomically and centrally sensitized state. 1 The addition of GV20 enhanced parasympathetic properties, 16 as did ST36. 17,18
Treatment of sympathetically mediated pain could have been via acupuncture of Bladder or Huato-Jiaji points. Preganglionic sympathetic neurons mediating sympathetic outflow to the upper limb are located in the lateral autonomic horn of the spinal cord between the levels T5 and T9. 19 Alternatively, auricular therapy, which has strong vagal innervation, could have been utilized to downregulate sympathetic outflow. 8,9
Finally, whenever treating a patient with chronic pain, it is vital they do not perceive treatment as a threat. 10 Pain is modulated somatically and psychologically. 3 Thus, positive patient expectation decreases the emotional impact on the ANS, therefore limiting exacerbation of sympathetic effects. ■