
Abstract
Background:
With healthcare costs steadily rising, cost-effective alternatives to traditional medical approaches are needed. Specifically, music therapy (MT), a form of complementary and alternative medicine (CAM), is shown to alleviate symptoms of an illness and improve overall well-being, as well as enhance allopathic treatment modalities, making it appropriate for use in various healthcare settings covered under many different payment schedules today. With interdisciplinary healthcare teams becoming the norm in practice, it is increasingly important that practitioners trained allopathically understand the importance of CAM and certain types of CAM practices such as MT that can provide important benefits for patients. Under the Patient Protection and Affordable Care Act of 2010 (PPACA), not only is wellness and well-being emphasized as part of overall healthcare goals, it is also reimbursable. Therefore, although some CAM practices such as MT require special licensure in order to serve clients specifically, any healthcare practitioner can understand and refer patients to MT services, as well as utilize aspects of MT within their own practice areas. Further, as the field of MT and appreciation for its benefits grows, evidence-based practice in MT is also essential. Therefore, research in CAM and MT furthers the overall acceptance over time by interdisciplinary teams, thereby increasing beneficial care approaches for patients. The purpose of this study was to identify and understand differences between physicians' (doctor of medicine [MD], doctor of osteopathic medicine [DO]) and non-physician practitioners' (nurse practitioners [NP], certified registered nurse anesthetists [CRNA], certified nurse midwives [CNM], physician assistants [PA], and clinical nurse specialists [CNS]) recommending practices, knowledge, and perspectives (attitudes, beliefs, and expectations) of MT as CAM. Clinically, understanding these differences is important to all practitioners so that they can better determine cost-effective means by which to enhance patient care within the confines of allopathic practice under the PPACA, Medicare, Medicaid, and private insurance payment structures today.
Materials and Methods:
A quantitative methodology with a descriptive, exploratory, cross-sectional, and correlational research design was used to measure recommending practices, knowledge, attitudes, beliefs, and expectations of physicians and non-physician practitioners utilizing a principal investigator-created valid and reliable tool entitled the Global Complementary/Alternative and Music Therapy Assessment (GCAMTA). A sample of 237 physician and 307 non-physician (total N = 544) practitioners participated. Data were continually collected electronically during a six-month period using various social media platforms: Facebook, Twitter, and LinkedIn. Additionally, access was provided to membership in several professional healthcare associations to recruit participants.
Results:
The GCAMTA revealed that 84.8% of physicians (MD/DO; n = 201/237) responded neutrally in their recommending practices, knowledge, attitudes, beliefs, and expectations toward MT as a CAM for their patients. Additionally, 86.6% of non-physician practitioners (NP, NA, CNM, CNS, PA; n = 266/307) responded more favorably toward MT as a CAM. For practitioners exhibiting higher knowledge of MT as a potential CAM (n = 207/307 [67.4%] non-physician practitioners vs. n = 36/237 [15.2%] MD/DO), favorability toward recommending MT as a CAM was also high. Results of the multivariate analysis of variance across all five dependent variables were statistically significant (p = 0.0001; α = 0.01).
Conclusion:
Educational curricula may contribute to the discrepancy in the views between physicians and non-physician practitioners. Traditional allopathic curricula may need to include teachings in holistic medicine in order to increase awareness of CAM such as MT. Additionally, further evidence-based research and longitudinal studies are needed for increased acceptance and eventual recommendation of these types of CAM approaches by healthcare practitioners in their practice. However, these types of revisions to curricula and practice take time. Recognizing this possible problem, practitioners need to become active healthcare providers and interdisciplinary healthcare team players by adopting evidence-based CAM approaches such as MT into their clinical practices, so that their patients have multiple cost-effective opportunities for care from which to select and achieve benefit.
Introduction
Overview of Healthcare Today, the Patient Protection and Affordable Care Act, and Complementary and Alternative Medicine
Healthcare today is very different from what it was, even just five short years ago. Today, practice in general is very team based and integrated. 1,2 Today's healthcare teams are interdisciplinary, meaning that they are comprised of several diverse healthcare practitioners (e.g., doctors of medicine [MDs], occupational therapists, physical therapists, nurse practitioners [NPs], physician assistants [PAs], and others) who work together collaboratively, depending on the needs of the patient. In order to obtain appropriate patient outcomes, varied degrees of collaboration and communication among the professionals is necessary. This integrated delivery of care is unique, and its success is based on effective information sharing among team members related to patient care, along with establishing an appropriate and comprehensive treatment plan to address the biological, psychological, and social needs of the patient. 1,2
Integrated delivery healthcare systems, or interdisciplinary healthcare delivery teams, are used across all different types of healthcare settings, from acute care to outpatient, subacute and homecare, just to name a few. Since the inception of the Patient Protection and Affordable Care Act of 2010 (the PPACA or “Obamacare”), numerous provisions of the Act are being aimed at resolving the problems in the United States' current system of healthcare delivery, cost, and payment. Particularly, changes are directed at developing, testing, and implementing new delivery models, reporting successes through publication, encouraging changes in payment from fee-for-service (FFS) to ones based on value of care provided, and access to resources directed specifically for system-wide improvements. 1,3
Although the true results of the PPACA are still being evaluated at the time of writing, the ACA has provided a clear commitment to testing and reporting on the successes and failures of new approaches to healthcare delivery and payment, with a clear acknowledgment that there is no one best single solution. 1,3 However, with this stated, the Act is providing an opportunity for the development of new and innovative delivery of healthcare, ergo the “interdisciplinary healthcare team approach,” and/or complementary and alternative medicine (CAM) approaches to patient care in conjunction with allopathic medicine approaches, all of which are being increasingly adopted and implemented across healthcare institutions today. As a matter of fact, the PPACA includes six separate sections specific to CAM practices in particular (s2706: Payment; s3502: Delivery; s4001: Health Promotion; s4206: Wellness Plans; s5101: Workforce; and s6301: Research). 4 However, with this adoption comes the responsibility of providing evidence of its successful implementation. To this extent, novel studies that explore and report on the success and/or failure of different allopathic and complementary approaches to patient care are within the realm of contemplation of patient care provided under the umbrella of the PPACA.
So ask yourself, do you believe that high-quality healthcare always has to come at a high cost, or is it possible to have directed quality care at a lower cost—one of the key goals of healthcare reform today? A rapidly increasing aging demographic, along with waiting to treat an illness until a person is sick, are both contributing to rising healthcare costs. 1 One way to reduce costs is to use preventive services, which are burgeoning in acceptance among leaders in healthcare, and this is becoming commonplace within the healthcare community of practitioners and their patients. Preventive services can include allopathic medical approaches complemented by CAM practices.
Under the umbrella of CAM, one readily available modality offered in hospitals and other medical establishments effective for both health and cost efficiency is music as therapy. 5 The prevalent use of music in healthcare to combat the problem of stress and anxiety, as well as assuage other mental health and physical states of care-receivers' well-being, is well documented in the literature. 6 –8
What Is Music Therapy?
Music is one of the CAM therapies—a group that includes massage, aromatherapy, acupuncture, and guided imagery—that are increasingly being offered in hospitals and other medical establishments. 5,9 Music therapy (MT) is the clinical and evidence-based use of music interventions to accomplish individualized goals within a therapeutic relationship. 10 MT interventions can be designed to promote wellness, manage stress, alleviate pain, express feelings, enhance memory, improve communication, and/or promote physical rehabilitation. 10 Music is a conduit that has the power to lift, transport, and engage attention and response. 11 As therapy, music can empower people to find their artistic selves and use their musical expression as a means for exploration and health; music provides the opportunity to communicate that which cannot be spoken. 12 Therapists seek to achieve patient goals with MT by recognizing the affective, cognitive, and sensory attributes of music. 13
What a MT Session Involves
Since the establishment of MT as a profession, therapists have been using a wide range of musical interventions to address the physiological, psychological, spiritual, and social needs of a variety of clinical populations. 14 Music can be passive, where individuals can listen to music for calming purposes or to evoke emotions. However, in the literature, the preference is for MT to be active. An active MT session deals with specific music selected for a specific patient. It is not limited to listening to live or recorded music, but rather can involve instrument playing, singing, songwriting, and improvisation. 15 Therefore, each MT session is tailored to the individual receiving the therapy and is dependent on his or her age, learning ability, attention span, as well as musical ability. An individual with little to no musical experience may receive the passive form before moving on to the active form of therapy once he or she has acquired enough musical training.
Additionally, it is possible for individuals with music capability to move between active and passive MT in order to accomplish a goal. 10 The instructor would determine this on a case-by-case basis when evaluating what will work best for the individual. Music therapists assess emotional well-being, physical health, social functioning, communication abilities, and cognitive skills through musical responses; design music sessions for individuals and groups based on client needs using music improvisation, receptive music listening, song writing, lyric discussion, music and imagery, music performance, and learning through music; and participate in interdisciplinary treatment planning, ongoing evaluation, and follow-up. 10 By continually assessing the patient's progress, greater outcomes can be achieved over a shorter period of time.
History and Evolution of MT
Music as a healing force affecting health and behavior dates back to the ancient writings of Aristotle and Plato. 10,16 The genesis of present MT began after World Wars I and II when community musicians played at veterans hospitals for veterans experiencing physical and mental trauma. Improvements in physical and emotional responses due to passive and active engagement of music with the veterans led hospital practitioners to hire musicians for further interventions. This led to the first MT degree program at Michigan State University in 1944. More recently, the American Music Therapy Association (AMTA) was founded in 1998. 10
Training and Licensure
Upon completing one of the approved college MT curricula, one is eligible to take the national examination offered by the Certification Board for Music Therapists (CBMT). Successful completion of this examination entitles one to the board-certified credential (MT-BC). The National Music Therapy Registry (NMTR) serves qualified MT professionals with the following designations: RMT, CMT, and ACMT.
Health Benefits of MT and Practical Recommendations and Relevance to Clinicians Who Are Not MT Licensed
Research supports the idea that music is healthy for the mind because it stimulates brain waves. 10 There is a relationship between music and brain waves, such that as stronger and faster rhythms make people more alert, slower music can help people meditate and relax. For clinicians with patients suffering stress, anxiety, and depression over a recent diagnosis or treatment plan, MT can be beneficial as a complementary therapy to improve mood and feelings of loss of control.
Practicing clinicians who believe that MT may be beneficial to their patients can provide access in several ways. One way to employ music within one's own practice is by playing recorded music in office waiting rooms or individualizing music through headphones, tailored to the preferences of the patient. If more formalized MT is required, clinicians can recommend patients to a certified, licensed music therapist through their healthcare institution, the AMTA, or the CBMT for structured and active MT sessions.
After evaluating their patient for what would be best for them, practitioners interested in using MT clinically would focus on patient goals by recognizing the affective, cognitive, and sensory attributes of music. 13 Areas where MT is particularly useful, effective, and reimbursed include: adult depression, anxiety and stress, pre- and postoperative surgical use, terminal illness and palliative care, cancer care, pain management, disabilities, geriatrics (particularly for improving quality of life involved with Alzheimer's disease and dementia for improvement of memory), autism spectrum disorder, and post-traumatic stress disorder. 1,2 –4,10 These health states along with MT benefits are more fully explained and referenced in Table 1.
Chan MF, Chan EA, Mok E, Kwan Tse FY. Effect of music on depression levels and physiological responses in community-based older adults. Int J Ment Health Nurs 2009;18:285–294; bMyskja A, Nord P. The day the music died. Nord J Music Ther 2008;17:30–40; cKorhan E, Khorshid L, Uyar M. The effect of MT on physiological signs of anxiety in patients receiving mechanical ventilatory support. J Clin Nurs 2011;20:1026–1034; dStuckey H, Nobel J. The connection between art, healing, and public health: A review of current literature. Am J Public Health 2010;100:254-263; eLai H, Li Y. The effect of music on biochemical markers and self-perceived stress among first-line nurses: A randomized controlled crossover trial. J Adv Nurs 2011;67:2414–2424; fPittman S, Kridli S. Music intervention and preoperative anxiety: An integrative review. Int Nurs Rev 2011;157–163; gLin P, Lin M, Huang L, et al. MT for patients receiving spine surgery. J Clin Nurs 2011;20:960–968; hWakim J, Smith S, Guinn C. The efficacy of MT. J Perianesth Nurs 2010;25:226–232; iNilsson U. Soothing music can increase oxytocin levels during bed rest after open-heart surgery: A randomised control trial. J Clin Nurs 2009;18:2153–2161; jGallagher M. Evaluating a protocol to train hospice staff in administering individualized music. Int J Palliat Nurs 2011;17:195–201; kThompson A, Grocke D. The effect of MT on anxiety in patients who are terminally ill. J Palliat Med 2008;11:582–588; lMagill L, Levin T, Spodek L. One session MT and CBT for critically ill cancer patients. Psychiatr Serv 2008;59:1216; mProtacio J. Patient-directed MT as an adjunct during burn wound care. Crit Care Nurse 2010;30:74–76; nNilsson U. The anxiety and pain reducing effects of music interventions. Aorn J 2008;87:780–805; oKemper KJ, Danhauer SC. Music as therapy. South Med J 2005;98:282–288; pHooper J, Wigram T, Carson D, Lindsay B. The practical implication of comparing how adults with and without intellectual disability respond to music. Br J Learn Disabil 2010;39:22–28; qMagee W, Bowen C. Using music in leisure to enhance social relationships with patients with complex disabilities. NeuroRehabilitation 2008;23:305–311; rLee YY, Chan MF, Mok E. Effectiveness of music intervention on the quality of life of older people. J Adv Nurs 2010;66;2677–2687; sSorrell J. Music as healing art for older adults. J Psychiatr Nurs 2008;46:21–24; tKim J, Wigram T, Gold C. Emotional, motivational and interpersonal responsiveness of children with autism in improv MT. Autism 2009;13:389–409.
MT, music therapy; CAM, complementary and alternative medicine.
Purpose of the Study
The literature is more heavily weighted on the positive side for using these services, suggesting that it would be advantageous to recommend using music as a CAM service, 5,6,8,17 but little is known about healthcare practitioners' encouragement of CAM and MT (or lack thereof) to care-receivers and their caregivers. Therefore, the purpose of this study was to understand physicians' and non-physician practitioners' recommending practices, knowledge, attitudes, beliefs, and expectations regarding MT as a cost-effective CAM. The aforementioned key terms are operationally defined in Table 2, and the key areas that are important for application of MT as CAM with clinical relevance for practitioners as cited in the literature currently are provided in Table 1.
American Music Therapy Association. Music Therapy Makes a Difference. 2017. Online document at:
Research Questions and Hypotheses
The research question driving this study is: What are the differences between physicians' (e.g., MDs, doctors of osteopathic medicine [DOs]), and non-physicians' (e.g., NPs, certified registered nurse anesthetists [CRNAs], certified nurse midwives [CNMs], PAs, and clinical nurse specialists [CNSs]) recommending practices, knowledge, attitudes, beliefs, and expectations regarding MT as a cost-effective CAM?
The corresponding hypotheses are as follows:
H1: As opposed to physicians, non-physicians have higher knowledge of MT as a CAM
and
H2: As opposed to physicians, non-physicians are more favorable toward recommending MT as a CAM based on their perspectives.
Materials and Methods
Design
This was a survey-based, descriptive, exploratory, cross-sectional, correlational study. Demographic characteristics of the sample were organized and summarized through a descriptive design. A correlational design was used to explore if a relationship existed between practitioners' knowledge of CAM and their recommending practices of CAM, specifically MT.
Participant Recruitment
Over a six-month period, two different approaches were used to achieve near-equal sample group sizes: purposive and non-purposive sampling. Upon achieving Institutional Review Board approval, healthcare practitioners meeting the inclusion criteria were recruited through national nursing and physician associations. Additionally, non-purposive snowball sampling was used through social media platforms (e.g., Facebook, Twitter, LinkedIn) to attract potential participants to a survey link, which was created on the SurveyMonkey host site. Inclusion and exclusion criteria are summarized in Table 3.
MD, doctor of medicine; DO, doctor of osteopathic medicine; NP, nurse practitioner; PA, physician assistant; CRNA, certified registered nurse anesthetist; CNM, certified nurse midwives; CNS, clinical nurse specialists.
Instrument Used
Although there are studies in the literature evidencing existing tools that measure perspectives of CAM therapies, 18 –22 until this study was conducted, no single consolidated survey instrument existed that comprehensively assessed all of the components of healthcare practitioners' recommending practices, knowledge, attitudes, beliefs, and expectations of MT as a CAM. Therefore, the authors created, developed, validated, and reliability-tested a new instrument entitled the Global Complementary/Alternative and Music Therapy Assessment (GCAMTA).
The GCAMTA has 64 survey statements based on a five-point Likert scale, ranging from “strongly agree” to “strongly disagree.” 23 Additional open-ended questions regarding practitioners' current and past referrals of individual CAM therapies such as MT are included. A high score on the total GCAMTA indicates higher favorability of MT as a potential recommended CAM by the practitioner. The tool is considered valid and reliable, and averages a 12-minute completion time.
Validity of the GCAMTA
A panel of five experts was used to obtain consensus on the construct variables, survey statements, and questions through a Delphi group facilitation technique. 24
Reliability of the GCAMTA
Cronbach's alpha for the GCAMTA with all five constructs combined is 0.944, which is considered excellent by George and Mallery. 25 Additionally, individual constructs obtained high reliability as well (Table 4), ranging from α = 0.806 (attitudes) to α = 0.924 (knowledge). All survey statements were appropriate to and consistent in their respective construct, evidenced by similar alpha levels (Table 5).
N = 544 participants.
George D, Mallery P. SPSS for Windows Step by Step: A Simple Guide and Reference. 18.0 Update (11th ed.). Boston, MA: Allyn & Bacon, 2011.
GCAMTA, Global Complementary/Alternative and Music Therapy Assessment.
This table only represents some of the survey statements that were present for each variable within the survey based on a Likert scale. The purpose of this table is to present the notion that statements were carefully prepared to measure the variable construct. The Cronbach's alpha score (if survey item was deleted) evidences the closeness of statements to the construct. Should one of the statements not have been representative of the variable, the deletion of such variable would result in α fluctuating away from the general range of scores present in the column from the other variables. Survey items not shown (for brevity purposes) presented an alpha similar to the other statements.
Data Collection
Survey research with physicians and other medical professionals is much different from research conducted on the general population due to demanding work schedules, leaving little time available for participation in surveys. 26 Additionally, physicians represent an elite group often asked to participate in survey research and have receptionists or other “gatekeepers,” which makes recruitment difficult, averaging ten percentage points lower than studies using the general population. 27 Therefore, paper-survey mailings and or fax mailings were avoided, and National Medical Association members were contacted electronically.
Social media acted as a direct conduit to physicians and non-physician practitioners in order to recruit them for participation in the study. Approval by Facebook closed group administrators was granted upon providing the parameters of the study. Invitations with the survey link were posted, resulting in Facebook users “liking” and commenting on the post and “snowballing” the link, yielding higher participant numbers. Similarly, survey links were shared on LinkedIn, and practitioners on Twitter were tweeted using appropriate hashtags (e.g., #physicianassistants).
Results
Demographics
An a priori G*Power analysis for F-test multivariate analysis of variance (MANOVA) global effects was calculated to determine the sample size, 28 requiring 220 healthcare practitioners. A sample size of 544 was achieved, consisting of 237 (43.6%) physicians and 307 (56.4%) non-physician practitioners.
If social media is strategically used, accompanied by U.S. National Medical Association members, then solicitation and engagement of participants nationally is attainable. GCAMTA participants came from every state except Nevada, Wyoming, and Iowa. The majority of licensed physicians were from New York, most likely due to the approval by a New York family physicians organization used by the authors to solicit members. Participants were also recruited from CNS and CNM associations across the United States. Additional demographic characteristics can be found in Table 6.
Physicians and non-physician practitioners.
License # refers to amount of practitioners who were licensed to practice within the state. Some participants were licensed to practice in more than one state.
Outcomes
Figures 1 and 2 represent an overall impression of MT as a CAM among physicians and non-physicians according to the five major constructs, revealing non-physicians holding positive perspectives of MT and physicians holding neutral perspectives.
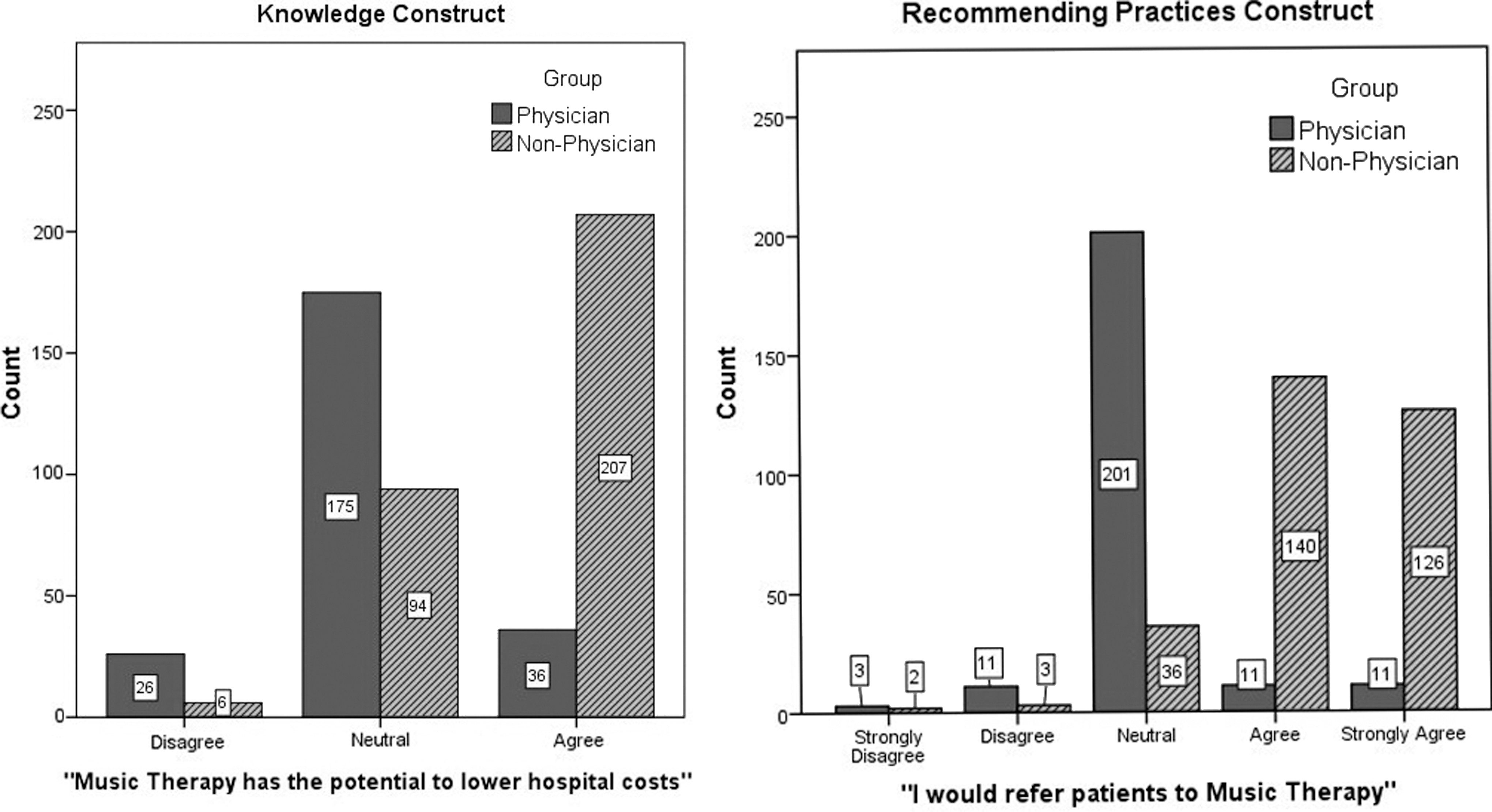
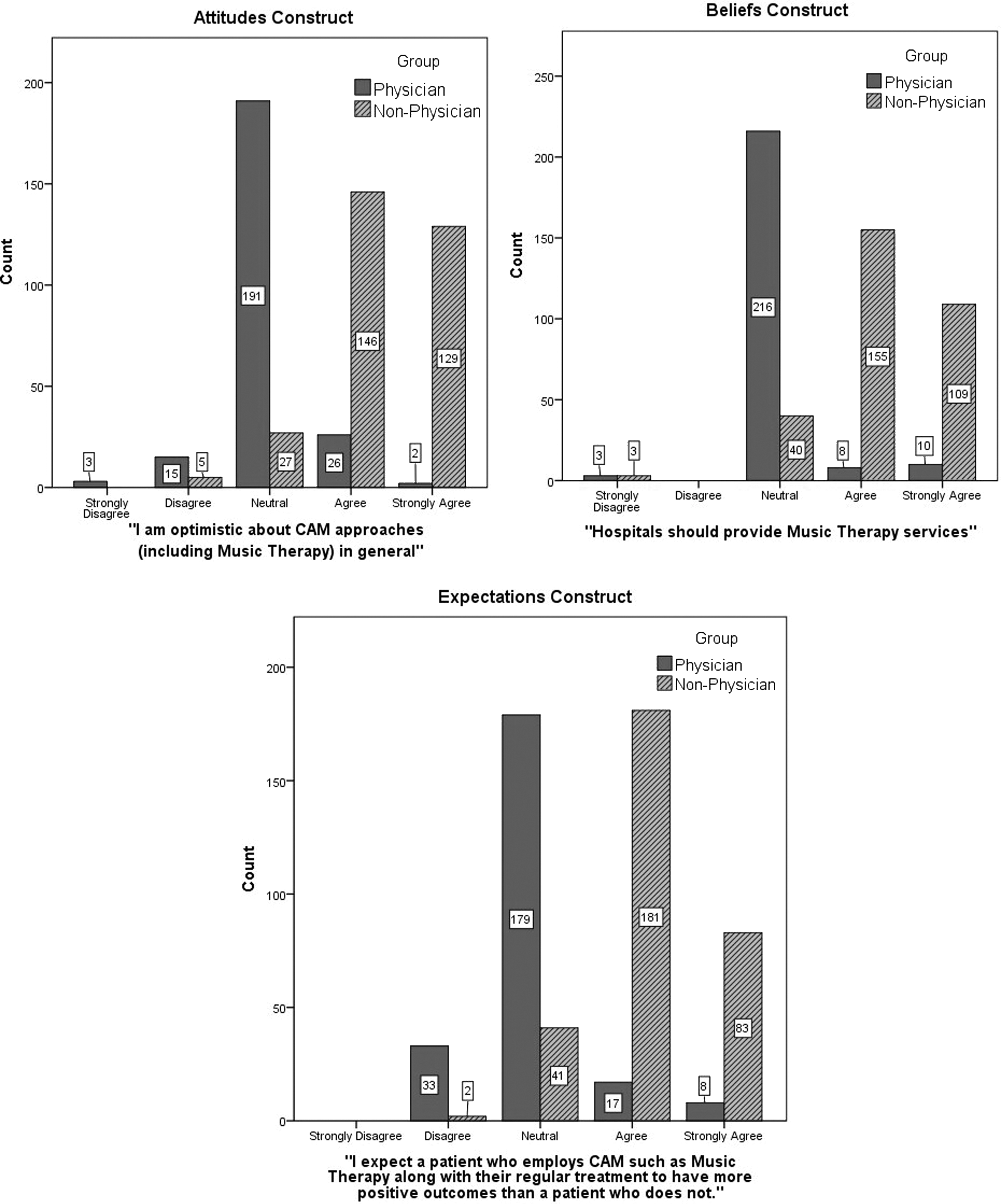
Non-physicians scored higher means on the GCAMTA for all five constructs regarding favorability to MT, CAM, and making potential recommendations to patients (Table 7). Correlational results revealed that as knowledge increased for a practitioner, so did his or her favorable MT and CAM recommending practices to patients (Fig. 3). Non-physician practitioners revealed higher knowledge and thus more favorability to recommending MT and CAM to patients.

SD, standard deviation
MANOVA was conducted on the GCAMTA data, revealing that the difference in means between the two groups (i.e., physicians and non-physicians) for each variable presented in Table 7 was indeed a significant difference (Table 8). Follow-up individual analysis of variance tests confirmed these findings on significance.
Results of MANOVA test of between-subjects effects revealing significance for all five dependent variables. Of particular note is the “Significance” column, evidencing p = 0.000 for differences between each dependent variable (0.05/# individual ANOVAs = 0.05/5 = 0.01 (above significance measured at 0.01 alpha level).
Significance equates to significant differences between two groups (i.e., physicians and non-physicians) per dependent variable.
Open-ended questions provided qualitative results that further allowed conclusions to be drawn supporting the quantitative results of the MANOVA. These questions revolved around exposure to CAM in educational background, training, and work environment; general amount of CAM recommendation during career; level of conservatism in practice; and amount of social media presence and activity.
Discussion
The Gender Gap
Females were the predominant responders in this study (Table 6). These results are consistent with the literature stating that the majority of U.S. non-physician practitioners are female and the majority of U.S. physicians are male. Specifically, 91% of nurses are female and 9% of nurses are male. 29 A 2014 U.S. census of actively licensed physicians revealed that 66% of physicians holding an active license to practice were male, 32% were female and 1.9% identified as other. 30
Recall that non-physician practitioners in this study were more favorable toward recommending CAM than physicians and that the majority of the non-physician practitioners were female. Based on these numbers, it might be concluded that female practitioners are more favorable than male practitioners in their recommendations of CAM. However, solely because a larger female population was present within this study does not mean that females are more apt to recommend MT than males. In order to make inferences on gender, further research is needed to balance out the gender groups, specifically, increasing the number of males. Results of this study may not be representative of practitioners across the board with regard to gender.
Discussion of the Five Construct Variables
Recommending practices
Recommending practices were categorized as favorable or unfavorable based on perspectives. For example, some practitioners prefer to spend more time with patients and engage in “small talk” and newsworthy health trends, while other practitioners are very succinct. Also, some practitioners may be inclined to recommend CAM, but may not have done so due to patients not inquiring about CAM or lack of applicability to their patients' illnesses. Results of this research study with regard to recommending practices suggest that practitioners who do not mind spending more time with patients are generally more favorable to recommending CAM to their patients.
Knowledge
Knowledge was categorized as high or low. Practitioners may perceive themselves to be informed about aspects of CAM but not as experts. For example, a physician may be aware about dietary supplements and nutritional counseling for patients, but may not be knowledgeable about meditation or hypnotherapy for patients. These practitioners may have a general sense that these types of CAM exist, but may not have sufficiently high knowledge of these modalities in order to recommend them to patients. Results of this study suggest that practitioners who have higher knowledge and awareness of CAM are more favorable to recommending CAM.
Attitudes
Attitudes were categorized as favorable or unfavorable and vary depending on the type of CAM. For example, a practitioner may have a favorable attitude toward chiropractic because he or she has had or knows someone who has had chiropractic treatments or due to the higher acceptance of chiropractic as an effective CAM treatment as opposed to acupuncture. Additionally, practitioners may view CAM as distractions in the healthcare setting. Some practitioners felt that silence is more effective for calming purposes than MT or that bed rest is more effective than prayer or massage therapy. Therefore, results with regard to attitudes suggest that practitioners who have been exposed to some form of CAM are more favorable to recommending CAM to patients.
The particular statement “I am a lover of music” was strategically placed within the GCAMTA attitudes construct to understand if practitioners would abandon their own personal attitudes toward MT and still recommend it to patients if they felt MT was beneficial for their patients. The results show that this might have indeed been effective. Some practitioners said that they are a lover of music and had favorable recommending practices of MT. This is not surprising because if an individual is inclined to use music personally, then he or she will probably suggest it for others as therapy.
Surprisingly though, some practitioners said that they are a lover of music but had unfavorable recommending practices of MT, possibly due to lower knowledge of MT, bad experiences with MT, fear of risk of emotional harm to the patient, reluctance to recommend until more evidence-based research emerges or until more education and/or exposure on the modality becomes available.
Expectedly, some practitioners said that they are not a lover of music and do not recommend MT for therapeutic purposes. Surprisingly though, some practitioners said that they are not a lover of music but would recommend MT, possibly attributable to higher knowledge of MT, positive experiences with MT, or pressure from work or peers to recommend CAM.
Beliefs
Beliefs were categorized as favorable or unfavorable. Practitioners may believe that certain CAM therapies such as MT are only appropriate for particular age groups or illnesses, that it is too expensive, and or that positive effects are due to placebo effect. 31 Results suggest that practitioners who have witnessed positive effects of CAM or had patients with successful CAM outcomes are likely to recommend CAM.
Expectations
Expectations were categorized as favorable or unfavorable regarding acceptance or non-acceptance of CAM. Expectations of lowered healthcare costs due to CAM appear to affect the recommending practices of practitioners greatly. Additionally, practitioners may have favorable expectations of CAM, but do not have high expectations of patients utilizing CAM on a continual basis for the required duration of treatment. Finally, practitioners may expect CAM to grow in acceptance by patients but not by other healthcare practitioners or, conversely, to grow in acceptance by healthcare practitioners but not by patients. Overall, results suggest that most practitioners expect CAM to become more widely sought after by patients, but not necessarily accepted by practitioners.
Influence of Social Media
The authors discovered that non-physician practitioners have a larger presence on social media than physicians, specifically on Facebook closed group pages, which are used by members to share new information, ask advice of fellow practitioners, and/or to express frustrations about their practice. Physicians were mostly discovered on Twitter and LinkedIn for promotion of their practice, with little to no presence on Facebook closed group pages, which may explain why the majority of study respondents were pro-CAM non-physician practitioners.
Conceptual Framework
Based on the aforementioned five constructs and taking into account educational background and social media exposure, a conceptual framework was developed to understand and evaluate the practitioners' responses further. The conceptual framework is understood through a series of five steps, as represented by an inverted pyramid (Fig. 4).
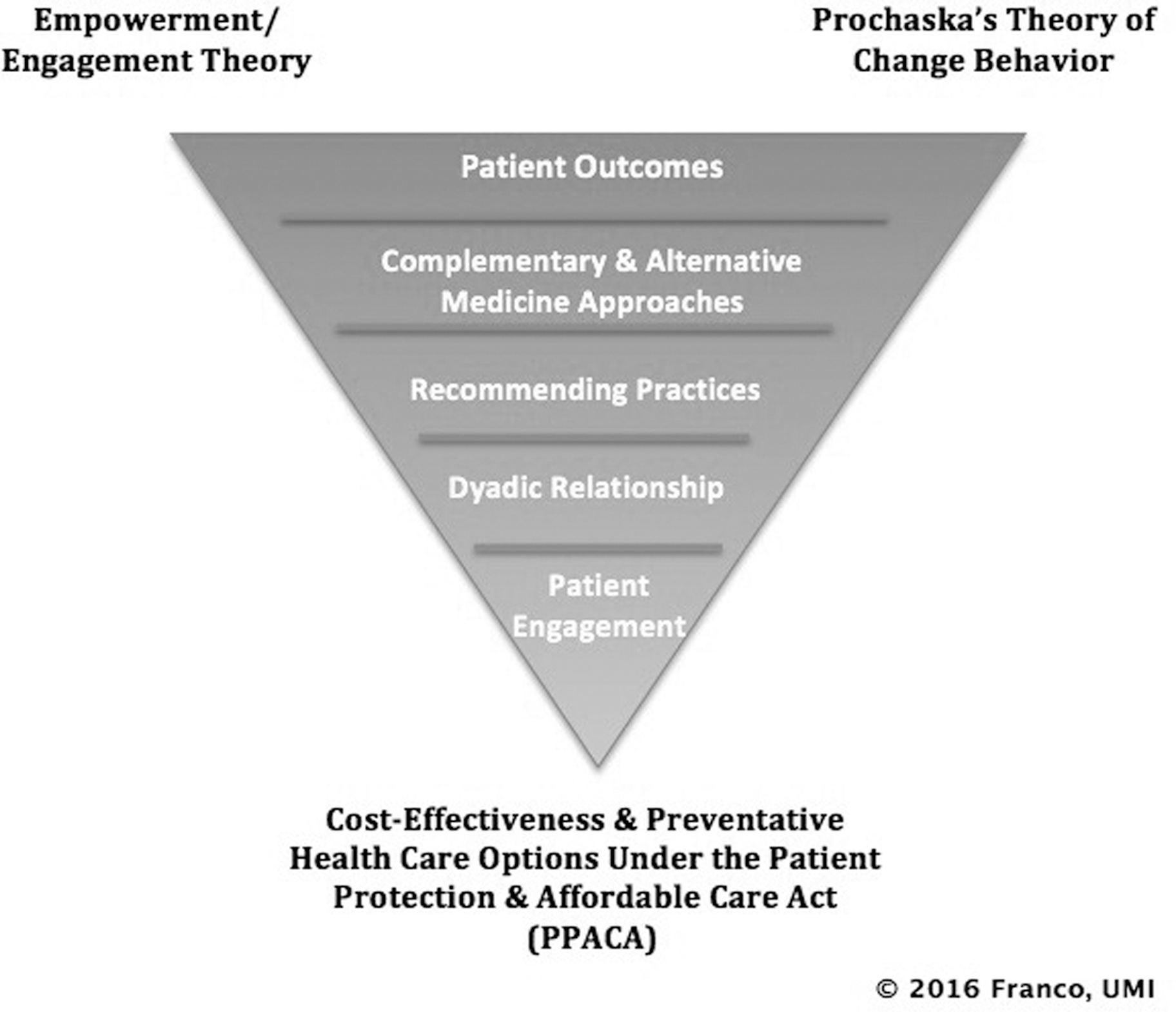
A driving force grounding this study and supporting the five key constructs is Cost-Effectiveness and Preventative Health Care Options under the PPACA, which focuses on CAM to prevent illness before costs rise from treating diseases that are in late stages. Waiting to treat illness until a person is sick, instead of focusing on prevention, has had a direct effect on the rising healthcare costs in the United States and has caused many Americans to put off seeing a doctor until it is too late due to cost. 1
Prochaska's Change Theory (i.e., Transtheoretical Model of Health Behavior Change) combined with Empowerment/Engagement Theory explain how a patient or practitioner makes a decision about accepting (changing routine treatment) or rejecting CAM. 32 The framework suggests that when approached with a relatively new factor (e.g., CAM), the practitioner decides to remain unchanged or adopt a new recommending practice. A perfect storm is created that ultimately sways the practitioner to decide whether to recommend or avoid recommending CAM to patients (Fig. 5).

Practical Recommendations and Clinical Focus
Why proactive adoption of MT and CAM by practitioners into clinical practice is important today
The results of this study support the initial hypotheses. Although the results were not surprising overall, curiously, why did the non-physician practitioners have higher knowledge about and express more liberal recommending of CAM than the physicians? One obvious suggestion is that this may be due to the educational backgrounds of the groups. In general, non-physician practitioners have a more holistic approach to patient care, taking the whole mind–body into account in practice, 33 partly because they are more exposed to CAM during their academic studies than their physician counterparts. 34
As stated at the outset of this article, educational curricula may contribute to the discrepancy in the views between physicians and non-physician practitioners as found in this research. Traditional allopathic curricula may need to include teachings in holistic medicine in order to increase awareness of CAM such as MT. 33 –35 Additionally, further evidence-based research and longitudinal studies are needed for increased acceptance and eventual recommendation of these types of CAM approaches by healthcare practitioners in their practice. However, these types of revisions to curricula take time. Relying on historical teaching and attitudes about CAM cannot be used as a “crutch” for why CAM should not be further researched and incorporated into practice by practitioners. Furthermore, these curricula or attitudes about CAM should not be relied upon unchallenged as “unknown or unproven” by practitioners reluctant to incorporate CAM into their practice or offer it to their patients. This research study is just one step of many to show the benefit of evidence-based approaches to justify incorporating CAM approaches into healthcare practice today. Cost-effective approaches to healthcare and wellness are provided for in the PPACA, Medicare, Medicaid, and private insurance already, even if it is somewhat limited to specific areas of CAM, as discussed previously herein. It is time for practitioners to become active participants in the clinical application of CAM approaches such as MT in healthcare. Active research about CAM is how any practitioner can make a relatively unknown, nontraditional healthcare approach “mainstream” over time.
Recognizing this possible problem of slow-to-adapt educational approaches in healthcare curricula, today's healthcare practitioners need to become active healthcare providers. Practitioners can begin this process, for example by adopting evidence-based CAM approaches such as MT into their clinical practices, so that their patients have multiple cost-effective opportunities for care from which to select and achieve benefit. While enhancing the knowledge base about CAM and MT, so that change can be brought about effectively across practice areas, overall patient care and cost-effectiveness of care over time is enhanced.
Future Directions for Research
Not all CAM therapies will be viewed the same or accepted at the same time. Additionally, generational differences may exist that affect recommendations (or lack thereof) of CAM. Younger generations may be more inclined to recommend certain types of CAM due to more exposure from social media. Furthermore, a longitudinal study, where a cohort of practitioners are tracked to see if their recommending practices and perspectives change, may prove to be beneficial in addition to future research on gender disparities.
Finally, because social media outlets are a burgeoning resource for patients as well as practitioners to seek out the latest information related to health, more research is necessary to examine the amount of time and degree to which healthcare professionals and patients use social media to obtain information related to CAM.
Conclusion
The state of healthcare is constantly changing. New modalities that lower costs and provide relief from pain and/or illness while increasing wellness are essential. Time will tell if practitioners adhere to the initial tenets of healthcare as contemplated in the PPACA, such as to continue recommending preventive medicine techniques such as MT for overall cost-reduction and improved health. It is clear that physicians must be educated and made aware of the health benefits of CAM, such as MT, and their role in recommending these therapies to their patients.
Interdisciplinary healthcare teams, the backbone of care today, also need to become aware of, or in some cases, more accepting of CAM practices, especially since the tenets of the PPACA provide for reimbursement and encourage the use of these strategies, such as MT, in patient care. However, as part of their responsible practice guidelines, they must have a basis of support for engaging in a CAM practice, or recommending a patient to a CAM provider, such as a MT, and that support comes from evidence-based practice and reporting in the literature on the successes and failures involved in such methodologies. Hopefully, practitioners reading this article understand that MT has a beneficial place today in practice in general and can be incorporated into their practice, and that this study based on the GCAMTA is one of several steps fulfilling the PPACA research initiatives to improve the provisions of healthcare in the United States.
Although individuals are exposed daily to music for entertainment, the strategic use of music as a healing agent is not as commonly understood. In the demanding work environment of the healthcare practitioner, there is a great amount of chaos and noise. If the goal of healthcare and medicine is to heal and improve the physical and mental health of our patients, then as practitioners, it is vitally important to open our eyes to look through the noise, open our ears to the sounds of music around us, and from this, improve the lives of our patients as well as ourselves.
Footnotes
Acknowledgments
We gratefully acknowledge the healthcare practitioners who donated their time, knowledge, and expertise to the honest completion of the GCAMTA survey instrument. Additionally, we are grateful to the professional medical associations and Facebook closed group administrators who granted access to their members for recruitment of participants.
Author Disclosure Statement
No competing financial conflicts exist. ■