
Abstract
Chronic joint or musculoskeletal pain is the leading cause of disability in the United States and worldwide. Current treatment options are limited in their ability to alter disease outcome. Recent studies are unequivocal about the inflammatory origins of musculoskeletal pain and prove that nutritional therapy can be a cost-effective option to improve patient outcomes in clinical care. This case study examines the effect of a nine-week nutritional intervention in a 47-year-old female with an eight-year chronic pain in her shoulders and knees. The nutritional program included a three-week Elimination Diet Food Plan, followed by a Detox Food Plan. Both diet plans followed guidelines offered by the Institute for Functional Medicine®. The client also had secondary complaints that included nausea, bloating, a foul taste in her mouth, and adult-onset acne. After nine weeks, the client achieved nearly full range of motion in her shoulders. Knee movements improved significantly, and the client was able pursue physical activities without pain. During this time, all digestive issues resolved and skin breakouts reduced, though skin lesions remained.
Introduction
Chronic joint or musculoskeletal pain is the leading cause of disability in the United States 1 and worldwide. 2 Musculoskeletal pain is a broad term used to describe specific diagnoses such as rheumatoid arthritis, osteoarthritis (OA), as well as symptomatic labels such as “joint pain” and “soft-tissue disorder.” 3 While there is much debate among physicians as to the diagnostic criteria for joint pain versus OA, 4 studies have shown that more than a quarter of patients with nonspecific joint pain of the hip, shoulder, knee, and hands receive a diagnosis of OA within six to eight years after initial consultation with a general practitioner. 5 Stiffness and pain may result in the inability to pursue leisure activities, perform household activities, or work, thus increasing personal and social economic burden. 6
Current treatment recommendations for managing arthritic pain follow a pyramidal scheme. First, education, including diet for weight management, and physical therapy are recommended. 7 Second, topical analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), intra-articular injections, opioids, and antidepressants are prescribed for pain management. Finally, invasive surgeries for joint replacements are considered in order to improve joint function. 7 Long-term use of NSAIDs is not without consequence and can lead to ulceration and perforation of the gastrointestinal tract. 8 Additionally, alternative therapies, such as acupuncture and transcutaneous electrical nerve stimulation (TENS), have shown some promise in alleviating pain. 7
As such, these treatment plans are palliative and focus on symptom reduction rather than treating the cause of inflammation. Previously, only some forms of arthritis were considered as truly inflammatory, but recent studies have shown that all forms of arthritis have similar etiologies. 9 Increasing evidence suggests that OA is not an isolated disease, but rather secondary to activation of the immune system, leading to high levels of inflammatory signaling chemicals, such as C-reactive protein (CRP), tumor necrosis factor α (TNF-α), cyclooxygenase-2 (COX-2), and prostaglandin E2 (PGE2), to name but a few. 9,10
In recent years, the role of foods has been highlighted as one of the causes for increasing systemic inflammation. 11 Paradoxically, nutrition is also one of the best measures for preventing as well as ameliorating the effects of inflammation. 12 Growing knowledge of the health-promoting constituents of foods has led to the rise of functional foods, which are defined as dietary substances in either whole or derived forms that provide benefits beyond basic nutrition. 13 However, are they enough to solve health problems that are on the rise?
Several functional foods have been considered for arthritic pain based on their effectiveness in reducing inflammation. For example, adding omega-3 fatty acids in the form of fish oil results in decreased cellular production of PGE2, a well-known pro-inflammatory eicosanoid. 14 Mouse models prove the actions of omega-3 for cartilage protection mechanistically, though very high amounts of omega-3 lead to structural irregularities. 15 The use of cod liver oil with NSAIDs in a short-term six-month randomized controlled trial did not change pain perception or movement in people with OA. 16 In a large meta-analysis on omega-3 oil supplementation, patients reported pain relief and reduced stiffness, while physician-assessed measurements did not find significant changes in pain. 17
In vitro research has shown that avocado and soybean oil unsaponifiables (ASU) have an anabolic effect on chondrocytes while downregulating the activity of PGE2 and interleukin-1 (IL-1). 18 However, while ASU are effective for short-term symptomatic arthritic pain relief in humans, long-term studies have not been quite as promising. 19
These trials demonstrate the usefulness of anti-inflammatory foods, but equivocal results may be due to the presence of pro-inflammatory foods in the diet that negate the beneficial effects of the functional foods. Therefore, it is essential to reduce consumption of foods that could promote inflammation while concomitantly increasing foods that promote long-term health.
The Western diet has an abundance of refined grains, sugars, vegetable oils that are high in omega-6 fatty acids, and processed foods such as deli meats that are high in trans-fats and preservatives and low in natural antioxidants. 11,20 Each of these promote inflammation through various means, including enhanced glycation and oxidative stress, decreased endothelial function and insulin sensitivity. 20 Removing these so-called modern foods is one of the primary goals of the elimination diet. 21 Another major goal of the diet is to avoid the intake of foods that activate the immune system in the gastrointestinal tract. These foods include wheat or gluten 22 and dairy. 23 A degree of personalization is also involved in the elimination diet, as foods such as nightshades may trigger or amplify immediate (or delayed) hypersensitivities in some individuals and thus may need to be eliminated. 24 Foods rich in histamine or salicylates may also cause similar reactions. 24 An often-overlooked objective of the elimination diet is to replace foods that are to be avoided with nutrient-dense foods, thereby promoting adequate calorie intake and not calorie restriction. 21
Methods
The following case presentation and findings are the outcome of an online Detox Program that was conducted under the mentorship of Dr. Deanna Minich, PhD, FACN, CNS. Selection criteria included being female between 35 and 65 years old, with no use of prescription medication, and no scheduled surgery during the time of the program (July 15, 2017, to September 15, 2017).
A total of 10 sessions were held with the client, including an initial consult and a weekly session for each of the nine weeks of the program. Initial intake and subsequent nutritional counseling were conducted via video conferencing using HIPAA-compliant healthcare software. The program was divided into three parts: (1) a three-week elimination phase, (2) two-week reintroductions, and (3) a four-week detox phase.
The client was provided with the following resources from the Institute for Functional Medicine® (IFM): Elimination Diet Comprehensive Guide, 21 Elimination Diet Food Plan, 25 Detox Food Plan Comprehensive Guide, 26 and Detox Food Plan. 27 A Medical Symptoms Questionnaire (MSQ) 28 was used weekly to assess the client's symptoms throughout the program. Food journals were collected at baseline, weeks 1 and 3 of the elimination phase, and weeks 6 and 8 of the detox phase. An online software program was used for macro- and micronutrient analysis.
Case Presentation
MH, a 47-year-old female of Caucasian descent living in South Africa, sought nutritional help for several long-term health problems. She had previously participated in online nutrition programs, which had helped her to lose nearly 10 lbs. in weight, but she felt she had fallen back into poor eating habits and was seeking guidance to start incorporating healthy meals. MH works for a large corporation, and because of her busy work schedule, she was interested in easy meal ideas that do not require a lot of preparation time. MH also wanted to increase the variety in her meals and to learn how to use spices to enhance the taste of her meals.
Chief Complaints
The client had three main complaints: (1) joint pain in her shoulders and knees that resulted in low range of motion and prevented participation in exercise; (2) upper digestive tract issues, which included bloating, nausea, and a foul taste in her mouth; (3) adult-onset acne on her face, cheeks, jaw, neckline, and arms. Minor complaints included rhinitis, skin rashes and itching, fatigue, headaches, and plateauing of weight loss.
Relevant Client History
MH's childhood meals consisted mostly of flour and sugar and little to no fruit and vegetables. MH disliked eating most foods and had an aversion to meat and high-protein food, which made her feel ill. Around the age of 14 years, her friends complained she had very bad breath. Additionally, she had heavy menstrual bleeding and cycles that lasted for about 7–10 days. She was diagnosed as being anemic and was given iron supplementation. She also had poor teeth, which required several mercury fillings, and abscessed gums, which required four or five rounds of antibiotics.
MH was diagnosed with endometriosis at 24 years of age by a gynecologist and eventually underwent a total hysterectomy at 34 years of age, but at the time of her evaluation, she was not on any hormone therapy (based on hormone lab results, per her physician). MH was also diagnosed with gestational diabetes and irritable bowel syndrome (IBS) during her first pregnancy. MH changed her diet to reduce added sugars and specifically eliminated soft drinks. Her physicians advised probiotics and olive leaf extract for IBS. Gestational diabetes resolved, and IBS diminished.
Between the ages of 40 and 43 years, MH underwent several operations: left knee surgery due to sports injuries, a hernia operation, and removal of polyps in the colon. Following her knee surgery, MH developed pain in both knees and both shoulders, but a bone mineral density scan did not show any signs of osteoporosis. At the same time, MH developed severe fatigue, brittle nails, and hair loss. She was diagnosed with vitamin B12 deficiency and was prescribed monthly vitamin B12 injections (5 mL), complete vitamin B complex, and biotin for hair loss. Fatigue improved with vitamin B12, while hair loss improved marginally. Further, MH developed acne in the form of painful pustules filled with clear discharge. Prescription medications for acne included cortisone and retinol creams, which provided little to no benefit.
Often, arthritic pain is familial, and it is important to ask for relevant family history. 29 Upon questioning, MH mentioned that her mother has been diagnosed with OA, while she had not received such a diagnosis, even though her pain rating for her left shoulder was about 8/10, and both shoulder and knee movements were highly restricted.
Significant events (Fig. 1) are shown using the IFM Timeline, 30 a tool that can help both clients and practitioners to look for underlying nutritional causes for disease manifestation.
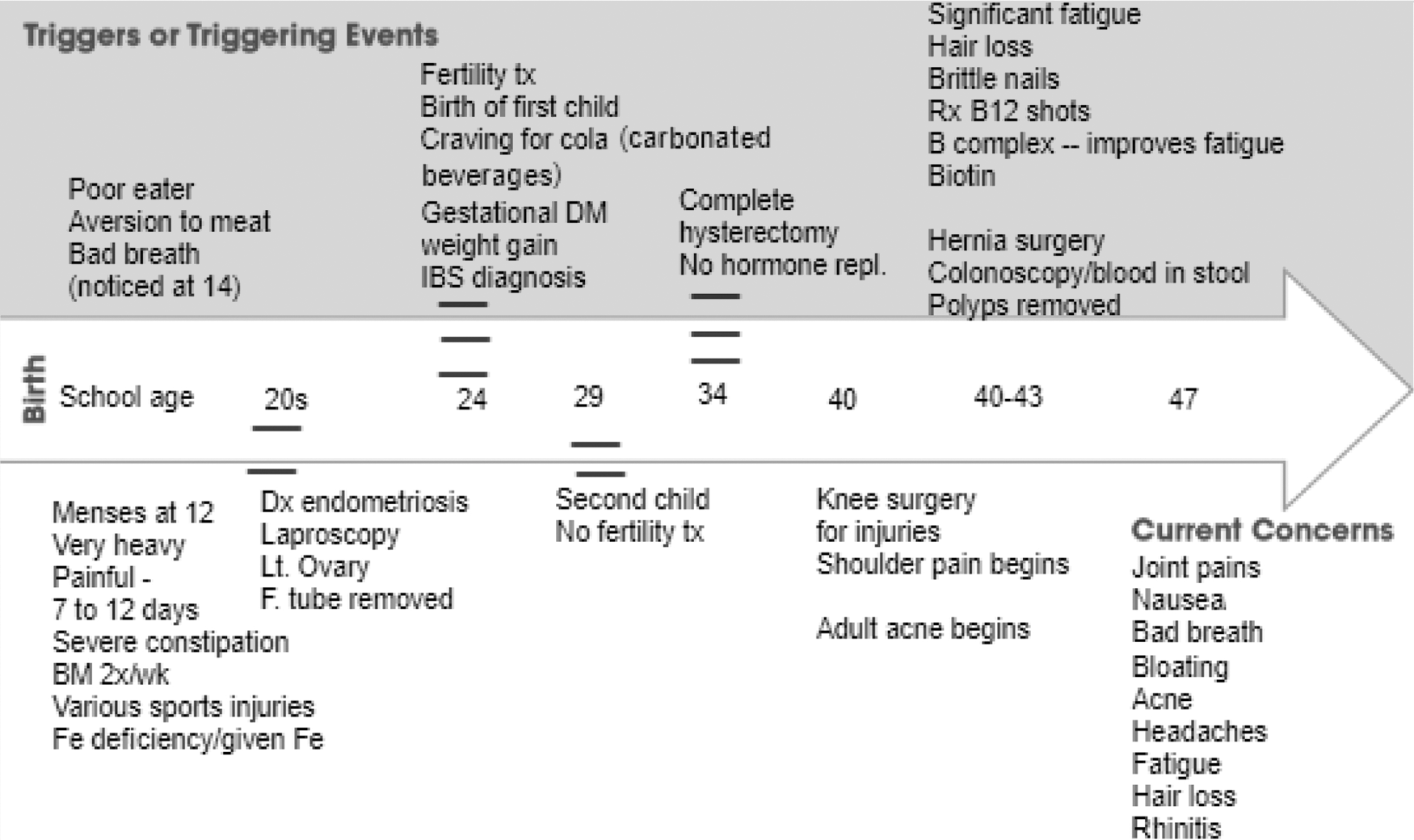
Institute for Functional Medicine® Timeline of significant events leading up to current conditions.
Diet
Her initial food journal revealed that several cups of coffee with milk and sugar (about six or seven cups) were consumed throughout the day, including coffee for dinner. Breakfast comprised of oats, bananas, milk, sugar, and coffee. The rest of her meals were in the form of small snacks, including lettuce, tomatoes, occasional packaged salmon, yogurt, milk, sugar, several tangerines, bananas, almonds, and occasional whey protein. Her diet was devoid of whole grains and legumes. Intake was low in calories, fat, fiber, and most minerals and vitamins, and high in added sugars. MH reported that she is not comfortable with cooking and tends to eat the same type of meals. She attributed her low intake to very low appetite and to a low desire to cook elaborate meals.
Supplements
The client was taking supplements prescribed by her physician, including a general multivitamin, iron (50 mg), folic acid (250 μg), vitamin B12 injection (1 mL monthly), biotin (300 μg), vitamin C (300 mg), and vitamin D (300 IU).
Lifestyle
MH is engaged in many creative pursuits and has the support of her family. She is a writer and a painter, and is aware of stress-management tools. MH reported sleeping seven hours each night and waking rested, though she mentioned headaches and nausea upon waking each day. She was unable to exercise due to joint pain.
Clinical Findings and Assessments
The client submitted a three-day food journal at baseline, and macro- and micronutrient analysis was conducted using online software. The Mifflin Jeor 31 equation was used to calculate resting metabolic rate (RMR). RMR was calculated at 1402 kcal, and activity levels approximated at about 280 kcal, accounting for a total of 1682 kcal of energy expenditure. Caloric intake from food was about 944 kcal, meeting only 56% of required energy intake. Chronic low calorie intake can lead to nutritional deficiencies 32 and fatigue. 33 Moreover, the food journal revealed little intake of vegetables, except for lettuce, tomato, and some bell peppers. Tangerine, a citrus fruit, featured prominently, with a maximum of five fruits eaten on one day.
Two possibilities emerged for her low calorie consumption: (1) excess caffeine intake, especially when taken between half an hour to four hours before a meal, can suppress the appetite 34 ; and (2) long-term nausea, leading to diminished hunger.
A herbal formulation, sometimes called Swedish bitters, typically including myrrh, gentian, zedoary, aloe, rhubarb, and saffron, was recommended to improve appetite and improve digestion. 35
A personalized diet is often used to address a client's food sensitivities, and in this case, food from the nightshade family and citrus fruits were considered for elimination for the following reasons. Some human studies attribute arthritic pain and inflammation to the presence of purportedly harmful glycoalkaloids in foods from the tobacco family, or Solanaceae, also called nightshades. 36 Commonly eaten nightshades include potatoes, tomatoes, bell peppers, and eggplants.
Citrus fruits are a common allergen 37,38 that increase the risk of atopic diseases and are often seen as a trigger for IBS. 39,40 Upon asking, MH mentioned that she noticed bloating on occasions after consuming tangerines. Seasonal winter fruits available in South Africa at this time were suggested as a replacement for tangerines. A combination of stewed apples with cinnamon was recommended to help relieve digestive complaints. 40 It was noted that both citrus fruits and nightshades could be added back into the diet if no reactions were noted upon reintroduction.
Taking all the above into consideration, the following dietary plan was created for the three-week elimination phase: Eliminate coffee, sugar, dairy, nightshades, and citrus. Green tea was suggested to help with headaches and other coffee withdrawal symptoms. Take Swedish bitters before meals. Eat three meals, including dinner, every day. Choose food from the list of allowed food (Table 1) and the Elimination Diet Food Plan.
25
Pay attention to hunger signals and digestive issues such as bloating and nausea. Take leftovers from dinner for lunch; several meal ideas for creating one-pot meals were provided to save time.
Foods to Avoid and Foods to Eat from the Institute for Functional Medicine® Elimination Diet Food Plan Guidelines
Case Progress and Results
The initial MSQ score was 51, indicating a wide range of symptoms, and the final score was 10 by the end of the nine-week program (Fig. 2). Adverse digestive scores fell from 8 to 0 by week 3, while joint pain decreased from 12 to 2, with occasional stiffness. Headaches and fatigue resolved with no incident after week 2. By week 3, skin rashes and itching disappeared, acne eruptions were minimized and less painful, and adverse skin score decreased from 10 to 4 by week 9, although the client was hoping for further improvements, given the overall success of the diet plan.
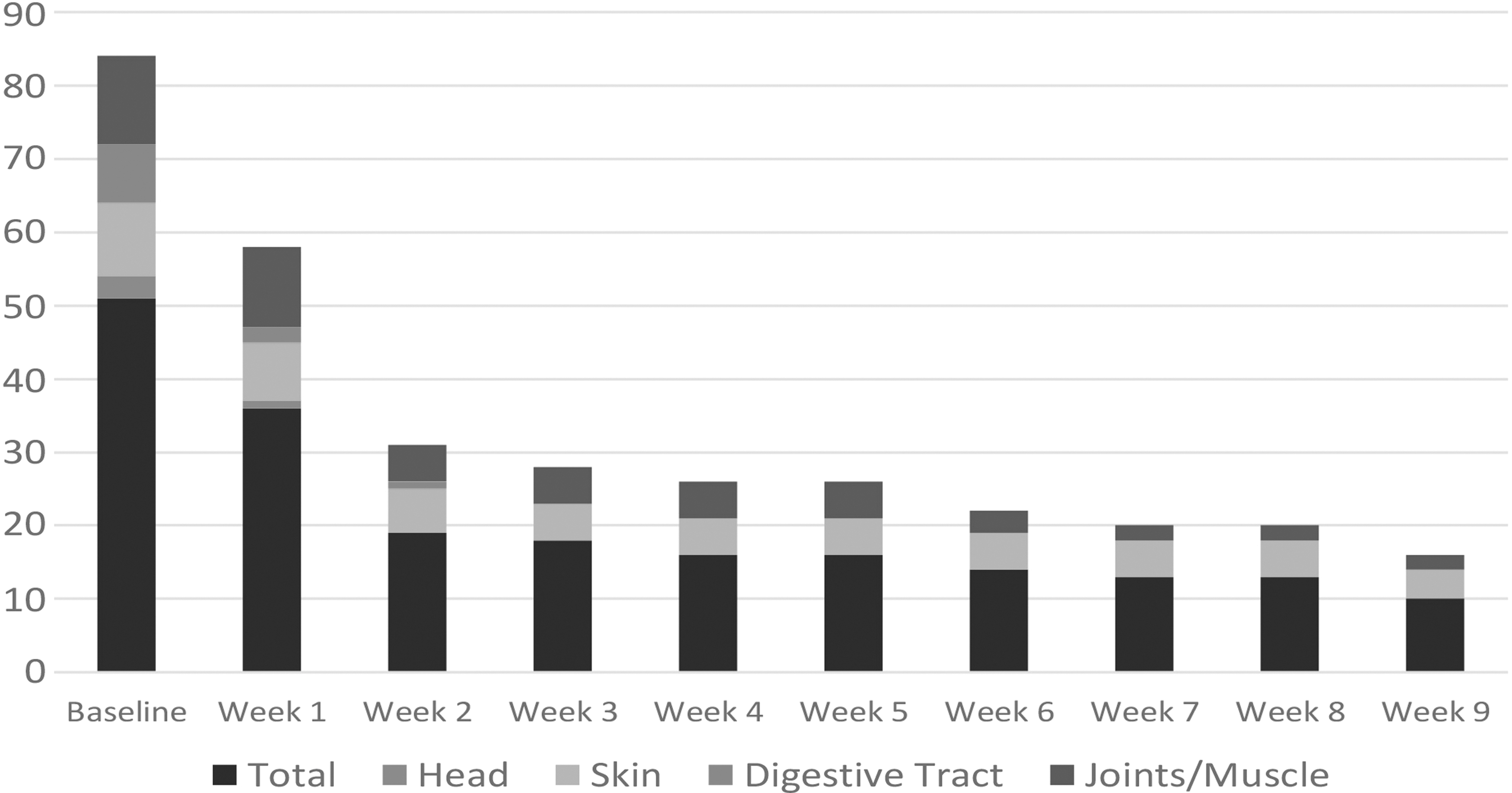
Change in total Medical Symptoms Questionnaire score and chief complaints scores.
The food frequency graph (Fig. 3) shows the change in food intake in a three-day timeframe between baseline and week 1 and week 3 of the elimination phase. The number of “foods to avoid” (Table 1) dropped significantly from baseline (53 counts) to week 1 (3 counts) and week 3 (1 count), while non-nightshade vegetables trended in the opposite direction, with portions nearly doubling in weeks 1 and 3 over the baseline intake. Vegetables included lettuce, spinach, carrots, broccoli, butternut squash, zucchini, sweet potatoes, and avocados. The reduction in the number of fruits is attributed to the decrease in tangerines, though the variety of fruits increased over baseline, and included apples, guavas, and pineapples. The reduction in protein foods in week 1 can be attributed to the client's increase in carbohydrates and vegetables, or the three-day log was not representative of the rest of the week. MH substituted coconut milk for cow's milk dairy and replaced white sugar with dates and honey. Spices added to meals included turmeric, cinnamon, oregano, fresh garlic, and coriander powder. Omega-6 to omega-3 fatty acid ratio stayed close to 4:1 from baseline through week 3. Carotenoids, vitamin K, and magnesium increased with vegetable intake. Olive oil, avocado, and nuts contributed to selenium and vitamin E increases.
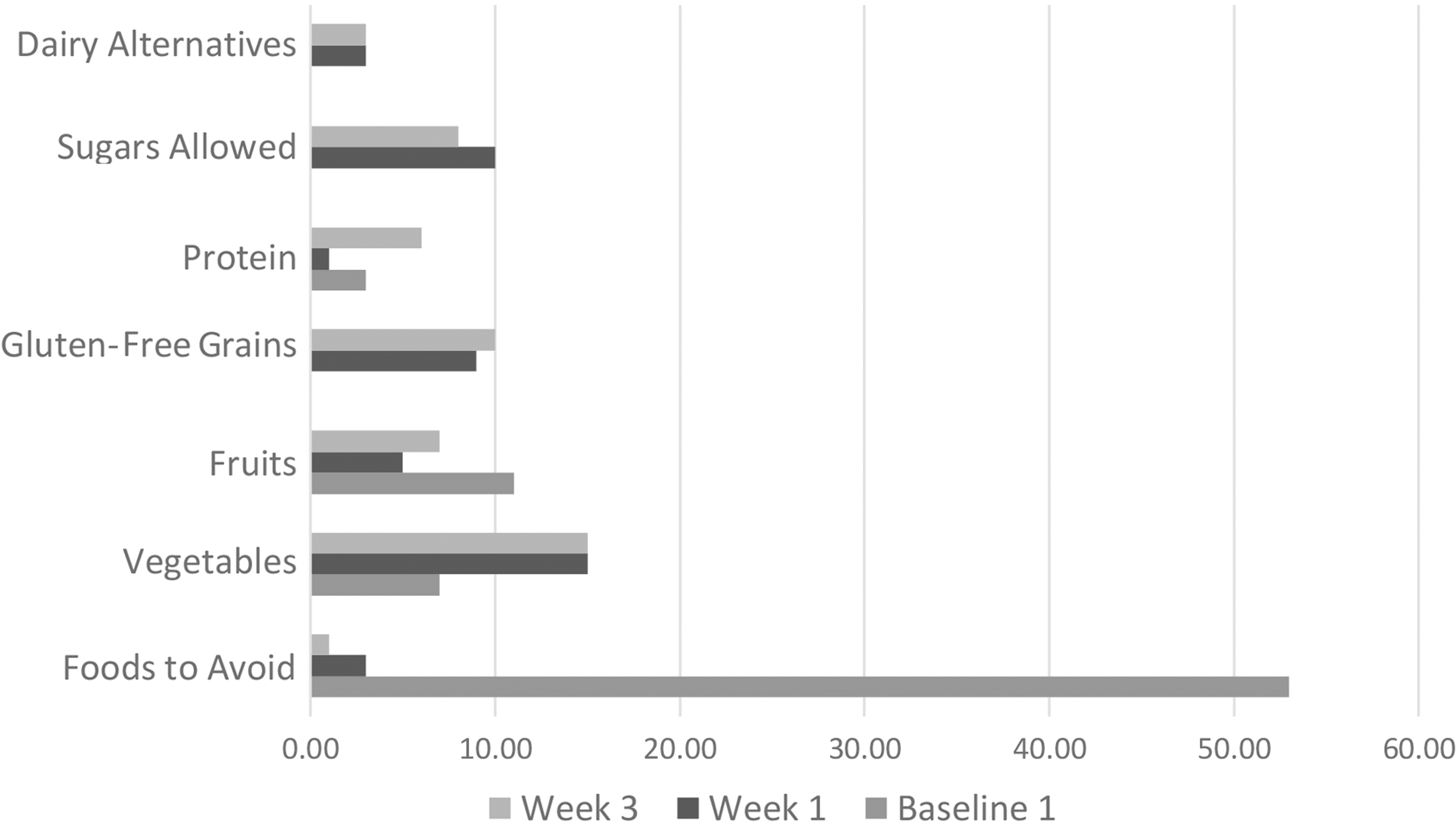
Servings of different types of foods over a three-day period at baseline, week 1, and week 3.
Bitters were stopped at week 3, as digestive problems had resolved. MH was anxious to try tomato, yogurt, and cheese. Food reintroductions did not go as planned, as MH fell sick with a viral infection, leading to cold and flu-like symptoms. Supplemental vitamin C (2000 mg) and zinc (15 mg) were added to support the immune system during the flu season in South Africa. Once the cold resolved, MH added whole-milk yogurt and noticed that it gave her loose bowels. It is unclear if the high fat content or if dairy alone provoked this reaction. Based on food journal entries, we discovered that high amounts of cashews (30 g) and mushrooms (two servings) eaten together resulted in watery eyes and blocked sinuses. These may have been due to the high levels of histamine in these foods. 25 MH also mentioned, “Since I started this nutrition journey with you, I am so much more aware of how foods can affect my body.” We decided that MH could try smaller portions of each food separately and watch for reactions.
Unfortunately, the Detox phase did not go as scheduled, as MH was involved with personal and professional projects that kept her busy. Weekly meetings were missed, though food journals were submitted. Her week 6 food journal showed a return to eating habits at baseline, with coffee, sugar, and milk, and very low calorie intake (800 kcal). MH talked about falling into old habits, as work tended to take priority over meal planning. Even so, joint pain improved, though skin scores did not. Dairy intake seemed to make her skin look worse, and MH decided to go back to coconut milk as a substitute.
At week 7, detailed instructions on the IFM detox food plan were provided, with an emphasis on spices, phytonutrients, and protein while avoiding dairy and gluten and reducing packaged gluten-free snacks such as rice cakes that featured prominently in the prior weeks. MH felt empowered to go back to healthier eating habits after this meeting, and her week 8 food journal resumed the patterns seen during the elimination phase. At the end of nine weeks, the pain in her shoulders dropped to about 1 on a scale of 1–10 (at baseline, her pain was 8/10), and the client said that she could sit on the floor with her legs folded: “I would not have tried this in the past, as it was painful to get into this position.” Additionally, the client was able to re-engage in aerobic and weight training exercises at week 3.
Following the conclusion of the program, MH summarized her progress in an email: “I was very frustrated with my joint stiffness, especially my left arm, which I could not lift above my shoulder or stretch in front of me. I can now lift my arm to full capacity. I found your approach gentle, supportive and encouraging, which made my education and journey back to health such a joy.”
Discussion
This case study demonstrates the utility of an elimination diet in resolving chronic joint pain in a 47-year-old female. The client had a long history of digestive problems, malnutrition, and poor appetite. Consequently, improving digestive function and absorption was an important consideration of this elimination diet.
Hypochlorhydria, or low stomach acid, was suspected at the outset of the elimination diet. Poor gastric function can cause low iron status and aversion to protein, as gastric pepsin is required for efficient digestion of protein. 41 Vitamin B12 deficiency can also be traced back to low stomach acid. 42 Overall, low stomach acid can lead to significant states of malnutrition, as energy from food is directed toward the bacterial overgrowth in the small intestine, which can also lead to digestive problems such as bloating. 41
The use of Swedish bitters helped to improve hunger sensations, as well as the ability to digest protein without causing nausea or digestive problems. While the exact physiological effects of bitters are unclear, there is some consensus that bitter herbs have holistic effects on the digestive system. First, oropharyngeal bitter receptors are said to stimulate saliva and the cephalic-vagal response, which increases appetite. Second, gastrointestinal bitter receptors locally enhance gastric secretions and emptying. Third, bitters increase superior mesenteric artery flow, which allows for better digestion in the intestines. 43
The reduction in coffee is noteworthy, as trigonelline, an alkaloid present in coffee, has been shown to have a deleterious effect on bone health and mechanical properties of bone in ovariectomized and estrogen-deficient rats. 44 While the client's estrogen levels were unknown during the time of the case study, the history of hysterectomy and ovariectomy supports the premise that caffeine may have a negative effect on her musculoskeletal health. Additionally, the client's diagnosis of endometriosis supports impaired estrogen detoxification, 45 while coffee consumption increases follicular phase estrogen production and circulation in a dose-dependent manner. 46 Therefore, her prior history of coffee consumption as well as her current high intake signaled a need for elimination.
Joint function is dependent on cartilage matrix integrity and elasticity, along with subchondral bone strength. 47 Basic nutrition for joint health includes protein, calcium, vitamin D3, phosphorus, and zinc. 48 However, as cartilage and joint destruction can occur due to a milieu of inflammatory signals, 9 nutrients that downregulate these chemicals are also essential. 49 Nutrients that are required for bone and joint health can be categorized based on metabolic activities they promote: (1) anti-inflammatory cytokines: omega-3 fatty acids, omega-6 gamma-linolenic acid (GLA), phytonutrients, pre/probiotics; (2) anti-inflammatory eicosanoids: omega-3 fatty acids, GLA, phytonutrients; (3) redox balance/antioxidants: phytonutrients, vitamins (C, D3, K2, and E); and (4) structural substrates: vitamins (C, D3, K2, and E), type-2 collagen, minerals (selenium, boron, zinc, and manganese). 49
It is important to recognize the contribution of fruit and vegetables in the prevention and reversal of chronic pain. Fruit and vegetables are a rich source of vitamins, minerals, and fiber, and they contain a long list of phytochemicals, such as polyphenols, terpenoids, resveratrol, flavonoids, isoflavonoids, carotenoids, glucosinolates, anthocyanins, and omega-3 fatty acids. 50 These provide strong antioxidant support and chemoprotection to our cells and tissues. 51
The strong free-radical quenching activity of fruit and vegetables is attributed to the synergistic action of the multiple polyphenols. One study showed that levels of antioxidant vitamin C in whole apples with skin contributed 0.4% of antioxidant protection, while the rest was attributable to the phenols and flavonoids in apples. 52 Other flavonoids such as quercetin, apigenin, and luteolin work directly on reducing the accumulation of leucocytes in cells and the synthesis of eicosanoids PGE2 and leukotriene B4 (LTB4). 53
Cruciferous vegetables such as Brussels sprouts, broccoli, and radishes are a rich source of sulforaphane (SFN), a glucosinolate derivative, which is a potent inducer of liver phase II enzymes prized for its protection against cancer. 51 In mouse models, SFN reduced synovial overgrowth and suppressed overactive T cells and autoantibodies to lessen arthritic scores significantly. 54
Limitations
The detox phase did not bring the same gains as the elimination phase. This can be attributed to the client's acute illness and personal plans that disrupted weekly meetings and discussions. As these circumstances are unavoidable, planned absences must be discussed ahead of time so that the client and nutritionist can implement meal strategies to cater for such situations. Vitamin D levels were not determined during the program, and it was unclear if supplementation was required. MH was asked to follow this up with her physician. Nightshades and citrus were not reintroduced, and hence it is uncertain if they were causative in mediating bone pain or IBS symptoms, but their removal improved both aspects of the client's health. Finally, the bitters formula made by a South African company may have had an independent anti-inflammatory effect that may need further investigation. It must be noted that joint function continued to improve more than six weeks after the bitters were stopped.
Conclusion
According to the latest projection, by 2040, the number of arthritic patients will increase by 40% in the United States alone, and the number of adults with arthritic pain will increase by 52%, leading to an estimated 113 million adults living in pain. 1
Public-health policies and clinical programs must consider nutrition as a novel adjunct for both the prevention and treatment of musculoskeletal, joint, or arthritic pain. Patients receiving nutritional support often have fewer complications and better outcomes, bringing down the overall cost of treatment plans. 55
This case study explores the relevant literature on the inflammatory pathogenesis of musculoskeletal joint pain, current treatment options, and the role of nutrition in stopping disease progression and improving joint function. Further, it sheds light on how nutritional counseling considers relevant client history to personalize nutrition therapy. One-on-one nutritional counseling is motivational and promotes adherence to diet plans, thus setting the stage for long-term healing and well-being.
Footnotes
Author Disclosure Statement
A.N. has no competing financial interests. D.M.M. is an independent contractor for the Institute for Functional Medicine and teaches as part of the Advanced Practice Module for Detoxification. ■