
Abstract

Introduction
It is relatively well documented within the literature that corticosteroid therapy can induce symptoms of mood lability, irritability, and some symptoms consistent with depression. Generally, these symptoms are dose dependent and will resolve on their own with dosage lowering or discontinuation. If this is not a feasible or immediate option, patients can be treated for the psychiatric symptoms using methods similar to how one would treat a psychiatric disorder in the absence of corticosteroid therapy. 1
S-adenosyl methionine (SAM-e) is believed to have antidepressant properties due to its ability to increase serotonin turnover through enhanced methylation of catecholamines, as well as promoting dopaminergic activity. SAM-e has also been shown to increase the body's ability to convert phosphatidylcholine into a usable form, which may improve mood and cognition deficits associated with the experience of depressive symptoms. 2
A high-quality NIH-funded study showed a significant improvement in mood and depressive symptoms in patients taking SAM-e compared with those in the control group. 3 It is known that monoamines such as serotonin—which plays a major role in mood regulation—are dependent at least partially on the presence of SAM-e. 4 Several studies have shown SAM-e to positively impact monoamine neurotransmission related to symptoms characteristic of mood disorders. 5 Several randomized controlled trials have supported the finding that the antidepressant efficacy of SAM-e in monotherapy is superior to placebo and tricyclic antidepressants. 5 Animal studies have also shown a reduction in aggression in rats exposed to doses of SAM-e. 6
Case Presentation
Background
L.C. was a 28-year-old female who was engaged in psychiatric treatment with this practitioner for chronic and moderate symptoms of anxiety and intermittent, mild depressive symptoms for several months prior to this intervention. These symptoms began in her mid-teenage years and vacillated in severity and frequency over the past decade, responding generally well to nonpharmacologic treatment modalities such as psychotherapy and mindfulness.
L.C. was diagnosed with lupus erythematosus (LE) two years prior, and was scheduled to begin a second trial of corticosteroid therapy (prednisone, 40 mg PO daily) for an acute flare-up. After two weeks on the corticosteroid therapy, L.C. came seeking assistance with avoiding or lessoning the significant adverse effects she experienced during her previous and current trial of corticosteroid therapy, which included significant irritability, depression, and mood lability—all of which negatively affected her social relationships, work performance, and mental and physical well-being. Given that L.C. has a propensity for alternative and complementary therapies, she sought a nonprescription approach to symptom mitigation.
Medical history
As mentioned previously, L.C. has suffered from symptoms of moderate anxiety and mild depression at various points in her young adulthood. She has not been hospitalized for any of these symptoms nor has she ever experienced any suicidal, self-harming, or violent ideation. She has not been medicated for any of these conditions and has responded moderately well to psychotherapy and mindfulness-focused therapies in the recent and remote past.
L.C. has no history of any major physical or medical injuries or illnesses. Surgical history includes a tonsil and adenoid removal in 2005 and a carpal tunnel repair in 2010. At the time of treatment initiation, her symptoms related to her LE flare-up included moderate to severe joint pain and swelling, moderate fatigue, and scattered skin lesions with photosensitivity.
Psychosocial history
L.C. did not smoke, drink alcohol, or use recreational drugs. At the time of treatment, she was in a committed relationship with a supportive partner, living with her parents for financial support. She was employed full-time as a health care professional, but recently cut her hours to part-time to decrease her stress level due to physical limitations that were worsening with her LE symptom exacerbation.
Assessment measures
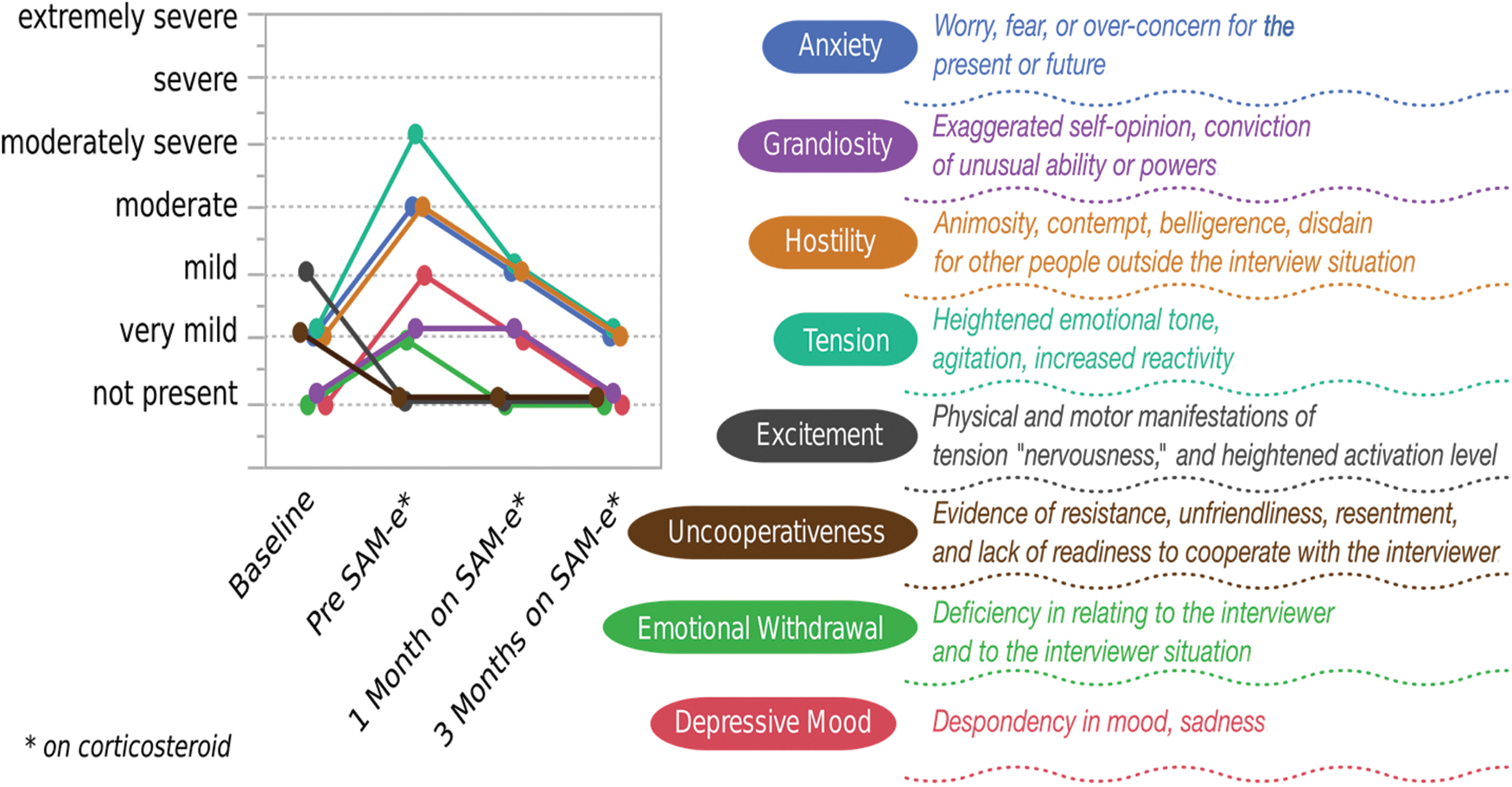
In addition to treatment sessions monthly and ad lib, the Brief Psychiatric Rating Scale (BPRS) was given at regular intervals to track and monitor symptom presence and severity. The BPRS is a widely used clinical instrument in assessing a wide variety of psychiatric symptoms, especially over brief periods of time (such as hospital stays). This was determined to be an appropriate choice of outcomes measure for this patient, as the comprehensive nature of the scale would encompass a wide variety of categories of psychologic symptoms (even those the patient had perhaps not experienced in the absence of corticosteroid therapy) and could track these quickly and easily over the duration of treatment. The intervals that were measured were (1) patient baseline (no SAM-e or corticosteroid therapy), (2) pre-SAM-e initiation (on corticosteroids for two weeks), (3) one month post-SAM-e initiation, and (4) three months post-SAM-e initiation.
Therapeutic Approach and Outcomes
After two weeks of prednisone therapy, L.C.'s treatment plan with this practitioner consisted of initiation of SAM-e at 200 mg qAM on an empty stomach for seven days, which was then increased to 400 mg qAM on an empty stomach thereafter. After one month of SAM-e treatment, as assessed and recorded using the BPRS, she began to experience relief from the BPRS-labeled symptoms of anxiety, emotional withdrawal, tension, depressive mood, and hostility she had developed after two weeks of prednisone therapy; however, she did not yet experience a decrease in the symptoms of somatic concerns or grandiosity. After three months of treatment, she experienced a decline in all of the aforementioned symptoms. Impressively, all of the symptoms that had increased in severity after corticosteroid therapy initiation returned to baseline by three months of SAM-e treatment. The exception, which perhaps was an anomaly given the emotional nature of the session preceding the baseline BPRS administration, was the category of excitement and uncooperativeness—both of which decreased after the initial baseline read. All of these results, as well as a description of each of the BPRS categories, are quantified and represented in Fig. 1.
Conclusion
For this particular client, SAM-e was effective in improving scores on several items in the BPRS. This patient was generally uncomplicated in terms of mental health treatment history and comorbid conditions; however, based on current available evidence, these findings are likely to be replicated for patients of various types with a similar treatment goal. SAM-e tends to be well tolerated and offers a good option for a patient looking to treat symptoms of mood disorders, including but not limited to irritability, without the use of prescriptive agents. 5 ■