
Abstract
Abstract
Background:
The auricular acupuncturist frequently uses physical changes in the auricle, whether visible or not, in the diagnosis as well as the treatment of many maladies. However, the practice of auricular inspection in nonauricular disease processes is not common in Western medical practice.
Objective:
To describe a case of significant physical auricular change correlated with severe pulmonary disease.
Patient:
A 14-year-old previously healthy boy with worsening respiratory status secondary to a new diagnosis of Wegener granulomatosis. Physical examination revealed large blood-filled bullae in the lung distribution of the lower conchae.
Main Outcome Measure:
Change in auricular appearance before and immediately after plasmapheresis.
Results:
Immediately after plasmapheresis, there was notably significant improvement in auricular appearance, with near disappearance of the bullae.
Conclusions:
Inspection of the auricle in patients with significant systemic disease may provide insight into the Western diagnosis and treatment of these patients. Further study of patients with concomitant auricular changes and pulmonary disease may better define the suspected auricular signs of pulmonary or systemic disease.
Introduction
Case Report
A 14-year-old boy, previously in good health, was admitted to a hospital for increased shortness of breath and coughing. His pulmonary status continued to deteriorate and he was admitted to the intensive care unit (ICU) for respiratory support. After an extensive medical workup, a diagnosis of Wegener granulomatosis was considered. He was brought to the operating room for placement of a Permacath so that plasmapheresis could be initiated.
On physical examination by an anesthesiologist, the patient was ill-appearing and required supplemental oxygen of 10 L by a nonrebreathing face mask to maintain his oxygen saturations to about 95%. His body temperature was 38°C, and his remaining vitals were stable. Auscultation of his lungs revealed crackles throughout, most pronounced at the bases. His heart examination was without murmurs, rubs, or gallops. He had no pharyngeal edema, had a class I airway with a thyromental distance of 8 cm, and normal range of motion of his neck. He was noted to have bilateral blood-filled bullae in both ears, at the lower conchae, corresponding to the auricular acupuncture Lung areas (Figure 1). He denied having any pathology of the ears or similar lesions prior to his admission to the hospital.

Bilateral blood-filled bullae in both ears, at the lower conchae.
Methods
A Permacath was placed without event under general anesthesia and the patient returned to the ICU where he underwent plasmapheresis. Physical examination and photographs of the patient's ears were taken immediately postoperatively upon return to the ICU. Several hours later, after plasmapheresis, the patient's pulmonary condition improved; he required no supplemental oxygen to maintain oxygen saturations greater than 95%, and his affect was bright. Photographs were again taken immediately following plasmapheresis.
Results
Auscultation of the patient's lungs revealed mild crackles only at the bases, and upon inspection of his ears, both bullae were diminished to the point that the right ear appeared nearly normal (Figure 2).
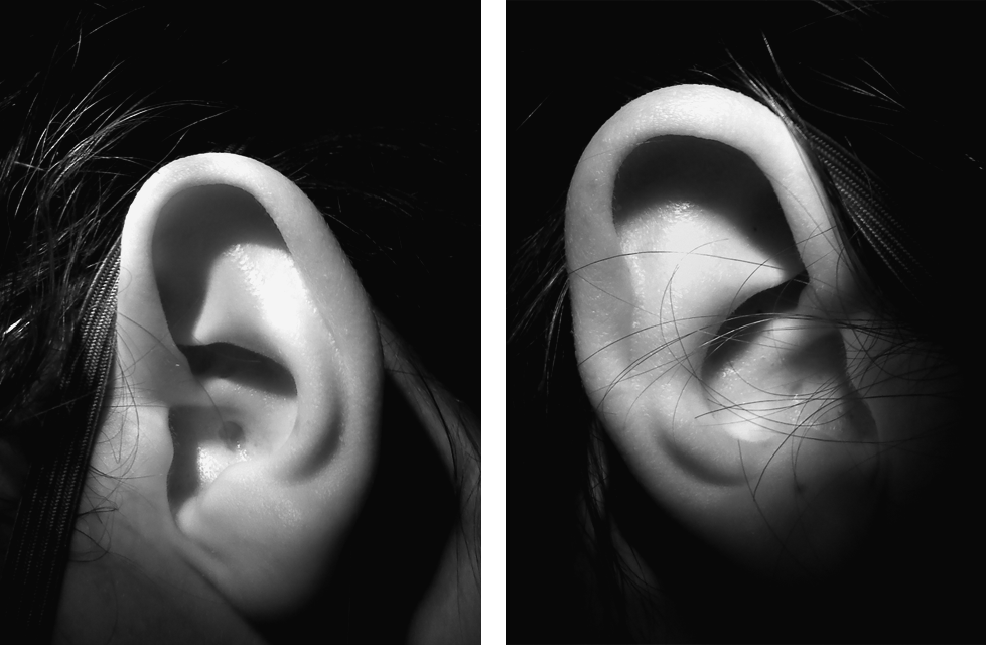
Patient's ears following plasmapheresis.
Discussion
Wegener granulomatosis is a systemic, necrotizing, and granulomatous vasculitis that affects the upper respiratory tract, lungs, and kidneys. It is the most common antineutrophil cytoplasmic antibody (ANCA) vasculitis. 4 Plasmapheresis reduces ANCA titers and can be useful in diseases in which circulating ANCAs can be pathogenic, 5 such as in the described case. Although clear evidence documenting the effectiveness of plasmapheresis in patients with Wegener granulomatosis is lacking, 6 its efficacy in this patient's clinical symptoms was clear.
The respiratory status of this particular patient improved immediately with plasmapheresis, with notably easier breathing and less supplemental oxygen requirement. The improvement in the appearance of the patient's auricle immediately following treatment was also dramatic. However, had the care team not been sensitive to the auricular signs preoperatively, the dramatic improvement in this physical sign might have gone unappreciated. Although the auricle may not be the most reliable indicator of the severity of a systemic disease process such as Wegener granulomatosis, it may provide additional clues as a reflection of the temporal course of a patient's disease. There remain few substitutes for following a patient's clinical picture, as even changes in radiographic studies frequently lag long after clinical symptoms resolve.
Conclusions
Inspection of the auricle in systemic disease is frequently underemphasized in the Western diagnostic tradition. Conversely, the acupuncturist, in addition to examining the patient's general appearance, pulse, and tongue, regularly inspects the auricle in the diagnostic process. Inspection of the auricle in patients with significant pulmonary or systemic disease may provide insight into the “Western” diagnosis and treatment of these patients. Acute changes in the patient's condition may be reflected by acute changes in the auricle as well. Further study of patients with concomitant auricular changes and pulmonary disease may better define the suspected auricular signs of pulmonary or systemic disease.
Disclosure Statement
No competing financial interests exist.
Footnotes
Acknowledgment
The author would like to thank Dr Carlos J. Munoz for his assistance in timely photography.