
Abstract
Abstract
Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), and excessive bleeding are serious albeit rare complications of major joint surgery. Chinese Medicine would relate these phenomena to Qi/Blood stagnation and Spleen Qi deficiency, induced by effects of surgery and drugs. Drawing from acupuncture theory and personal experience, the authors suggest an energetic approach that might enhance current prevention strategies for suitable patients.
Introduction
Joint Replacement Surgery: Postoperative Issues
Venous thromboembolism (VTE) and excessive bleeding are occasional but potentially serious complications of major surgery, particularly total joint replacement surgery. Eliminating such complications is a universal therapeutic goal. We all want to minimize the risk to our patients from the possible sequelae of DVT and at the same time minimize the risk of the prevention treatments. 4
Attempts to reduce the incidence of pulmonary embolism (PE) have largely centered around early mobilization, mechanical compression (stockings and pneumatic compression devices), and anticoagulants such as low-molecular-weight heparin (LMWH), warfarin, and aspirin. Much debate surrounds the best choice of these medications. Although choosing the most appropriate anticoagulant is clearly important, rarely is any consideration given to the negative impact of other drugs routinely used in the perioperative period that might contribute to blood clotting, such as opioids and gabapentin. But from an acupuncture perspective, using potent anticoagulants to counteract the effect of other routinely prescribed medications is contradictory and potentially counterproductive.
Perhaps for many low-risk patients, a better approach might be fewer medications, not more, combined with alternative approaches for pain management. For example, during my (Greenwood) own hip replacement surgery, I (M.T.G.) was surprised at the way potent analgesics were being liberally distributed to people who neither wanted nor needed them. The intent behind this policy seemed to be a pervasive assumption that everything possible should be done to eradicate pain in order to facilitate early mobilization. Though no doubt rooted in compassion, the policy actually compounded issues of urinary retention, ileus, and constipation, which in turn needed to be managed with yet more drugs and sometimes invasive procedures like bladder catheterization (as if there was no relationship between the stagnation of the bowels or bladder and stagnation of the blood).
It seems that modern evidence-based research has become so concerned over the esoteric differences between dalteparin, warfarin, and aspirin that it simply forgets to consider the impact of analgesics and the issue of energy flow maintenance.
Guidelines
The current guidelines proposed by the US Centers for Medicare & Medicaid Services (CMS) for use of perioperative anticoagulation have been imposed on orthopedic services without consulting the surgeons on the frontline. 5 CMS adopted guidelines from the American College of Chest Physicians (ACCP) recommendations, and many hospitals implemented the guidelines over the objections of orthopedic surgeons, largely to avoid lawsuits. Yet perhaps because the ACCP is not a surgical organization, its guidelines fail to consider the impact of various medications on local surgical complications such as wound healing, hematoma, prolonged drainage, and infection.6,7 Perhaps worse, most of the studies cited by the ACCP in drafting the guidelines have been industry sponsored. 8 In response, the American Academy of Orthopaedic Surgeons has developed its own guidelines. 9 And to add to the confusion, there is yet a third set of guidelines from the Surgical Care Improvement Project (SCIP), to which hospitals must pay attention.10,11
If it weren't for such political pressures to use the latest drugs, many surgeons would actually prefer to use aspirin combined with mechanical compression for low-risk patients. 7 Such a simple approach is not without justification, because while aspirin may not be as effective as LMWH preparations to prevent deep vein thrombosis (DVT), it has proven equally effective for preventing PE.5,12 And perhaps more to the point, potent anticoagulants have paradoxically been associated with a higher all-cause mortality rate. 13
One difficulty is that bleeding complications from potent anticoagulants are not insignificant. Major bleeding occurs in about 2% of hip surgery patients. 14 Hemorrhages into the spinal cord or brain can be catastrophic, while local bleeding can give rise to the most common complication of patients having to be returned to the operating room. For example, in 1 study, the use of enoxaparin was associated with significantly increased surgical complications: 4.7% readmissions, 3.4% return to the operating room for wound incision and drainage, 5.1% prolonged hospitalization (wound drainage), and 3.4% injection site complications. In addition, the number of days of wound drainage was predictive of a return to the operating room for hematoma or infection. 7
Placing the anticoagulant question into the broader context of energy flow maintenance might encourage a more creative approach to postoperative drug use, and the incorporation of other energy techniques such as acupuncture and herbal therapy in the perioperative period.
Drugs Used in the Perioperative Period
Opioids (e.g., hydromorphone)
are routinely used for postsurgical pain. While they are certainly effective, it is probably not because they move the Qi, as current Chinese medicine opinion might suggest, 15 but rather because they induce dissociation. 16 Indeed, the fact that opioids frequently produce adverse effects such as constipation, urinary retention, nausea, and mental confusion indicate that they actually aggravate Qi stagnation (Table 1). Since pain is itself a reflection of Qi stagnation, opioids tend to make the problem worse while simultaneously reducing mental presence, a mechanism that can cause tachyphylaxis. That the use of opioids simultaneously increases the need for them, while well understood in a chronic use/abuse context, seems underappreciated in the acute setting. The issue is not so much a concern about dependence or addiction, but rather the consequences of aggravated Qi stagnation exacerbating the incidence of postoperative complications.
Gabapentin and Pregabalin
Structural derivatives of inhibitory neurotransmitter γ-aminobutyric acid (GABA), gabapentin and pregabalin are indicated not only for epilepsy, but also for neuropathic pain in conditions like reflex sympathetic dystrophy and fibromyalgia. Their mechanism of action is unknown, but they are thought to bind to the α-δ subunit of the voltage-dependent calcium channel in the central nervous system, which in turn reduces calcium influx into the nerve terminals. 17 Both are often used in the postoperative period to manage pain and restless legs and to reduce the need for opioids like hydromorphone. Side effects include dizziness, drowsiness, peripheral edema, and liver and renal toxicity (Table 1).
Drugs Used in Anticoagulation
Aspirin
Aspirin is a relatively safe, inexpensive, and effective anticoagulant that works by suppressing the production of prostaglandins and thromboxanes through inactivation of the cyclooxygenase enzyme.18,19 It is not without side effects and it can induce gastritis, microscopic bleeding, and occasionally more serious bleeding complications (Table 2).
LMWH and Alternatives
Enoxaparin, dalteparin, and tinzaparin are LMWH preparations given subcutaneously on a once- or twice-daily basis in the perioperative period; fondaparinux, a synthetic pentasaccharide, is used in a similar way. 20 A more recent addition to the list is rivaroxaban, an oxazolidinone derivative that has the advantage of once-daily oral administration. 21 All these agents interfere with factor Xa, and their perioperative use is a balancing act between positive and negative effects. Adverse reactions include bleeding, anemia, elevation of serum aminotransferase, diarrhea, nausea, and heparin-induced thrombocytopenia (Table 2).
Warfarin
Warfarin is a vitamin K antagonist that decreases blood coagulation by inhibiting vitamin K epoxide reductase. Although widely used to reduce blood coagulability, it also paradoxically can increase coagulability when first started, which is why heparin is often used adjunctively at initiation of warfarin.
Energetic Effect of Drugs
Tables 1 and 2 show that the major energetic effect of opioids and gabapentin is Qi stagnation, from Liver to Stomach, to Large Intestine, to Bladder. Peripheral edema might be related to Kidney or Spleen Yang deficiency and is in the postoperative period more likely due to traumatically induced Qi stagnation, secondarily aggravated by the analgesics. Though the effect is probably minor in comparison to surgery and analgesics, anticoagulants can paradoxically compound the stagnation by spreading it to other systems like the Blood and Lungs, while further compromising the Spleen Qi so that the stagnant Blood pools rather than clots.
Chinese Medicine and Risk Stratification
The attempt to standardize perioperative anticoagulation has led surgeons to appreciate and stratify risk factors tailoring the use of LMWH or warfarin therapy to higher-risk patients. Such patients include those with varicose veins; chronic venous stasis disease; lower extremity edema; recent surgery; history of malignancy; body mass index greater than 30; older age; use of drugs such as birth control or hormone therapies; current or recent inflammatory or infectious process; current immobility; smoking; and a history of DVT or PE. 4
In Chinese medicine, these higher-risk patients would probably correspond to those with preexisting Qi and Blood stagnation, and in more frail or elderly patients, Spleen and Kidney deficiency. The Chinese medicine concept of Blood stagnation is not synonymous with venous thrombosis. Rather, it might be understood as sluggish blood movement that can give rise to blood pooling in predisposed patients, such as those who are overweight or who have leg varicosities. Such patients would likely be classified in Chinese medicine as Spleen Qi deficient or a Tai Yin Earth constitution. Excessive postoperative bleeding, though occasionally related to Heat in the Blood (either from a postoperative fever or more rarely, an infection), is more often due to surgical trauma followed by drug-induced Spleen Qi deficiency, particularly if superimposed on a constitutional predisposition.
Postoperative Energy Dynamics
Figures 1 and 2 illustrate acupuncture energy dynamics; Figure 1 illustrates a low-risk individual with normal Qi flow. Surgery will result in a temporary compromise of Qi flow, but probably not sufficient to induce Blood stagnation. In this situation, early mobilization is likely all that is necessary to reestablish normal flow. If analgesics are overused and compression stockings prescribed, an inadvertent conversion of Qi to Blood stagnation may occur.

Surgical trauma leads to some obstruction of normal Qi flow.

Preexisting Qi stagnation leads to Blood stagnation and bleeding.
Figure 2 represents a higher-risk individual with preexisting Qi and/or Blood stagnation. Surgery, with or without analgesics, may precipitate or worsen Blood stagnation. When potent anticoagulants are added, excessive postsurgical bleeding and/or prolonged serous drainage may occur.
The highest-risk individual, with both Qi/Blood stagnation and deficient Spleen/Kidneys, may well already be receiving warfarin. Surgery plus analgesics, anticoagulant complications, and difficulties with mobilization may precipitate a complex combination of Blood stagnation and hematoma formation.
Contradiction of Energy Strategies
While attempting to promote energy flow through early mobilization, the conventional approach simultaneously blocks energy flow with drugs. Compression stockings, too, may be a double-edged sword. While studies certainly show some benefit to the use of such stockings in bed-confined hospital patients, 22 it is not clear whether that benefit extends to those who are low-risk, motivated, and mobilized early. To be fair, there are different kinds of compression stockings: pneumatic and graduated. While the pneumatic compression stockings probably do promote Qi/Blood flow in bed-confined hospital patients, the graduated compression stockings prescribed for home use, while mitigating leg swelling and blood pooling, simultaneously block the flow of Qi.
Although their energetic effects are minimal compared with opioids, anticoagulants offer a similar contradiction. While studies show that anticoagulation works to reduce the incidence of venous thrombosis and PE, the downside is that they increase the tendency to bleeding and paradoxically, to Blood stagnation as well. Thus, conventional perioperative management fails to appreciate that early mobilization is just one energy strategy amongst others, and misses the strategic importance of intention and energy consistency that ensure that all energy strategies are in alignment.
A more creative approach for suitable patients might be one that aligns all energetic strategies. Such an approach is very much the purview of Chinese medicine.
Chinese Medicine Treatment Options
Ear Acupuncture
All patients, regardless of their risk stratification level, could benefit from ear acupuncture. Ear acupuncture has been shown to reduce pain in acute injuries; can be used to reduce the need for opioids; and is currently used by the US military in the field. 23 Figure 3 illustrates the regimen. It includes 5 standard ear points placed in a specific order (Cingulate Gyrus, Thalamus, Omega 2, Point Zero, and Shenmen). The NADA (National Acupuncture Detoxification Association) protocol is another option illustrated in Figure 4 and is intended especially for those having difficulty tapering opioid use (Sympatheticus, Shenmen, Liver, Lung, Kidney). 24 In either case, points representing a surgical scar could easily be added. Such an approach would likely reduce opioid use, improve mental clarity, moderate adverse effects like constipation, and thereby help with mobilization.

Battlefield Acupuncture Ear Acupoints.
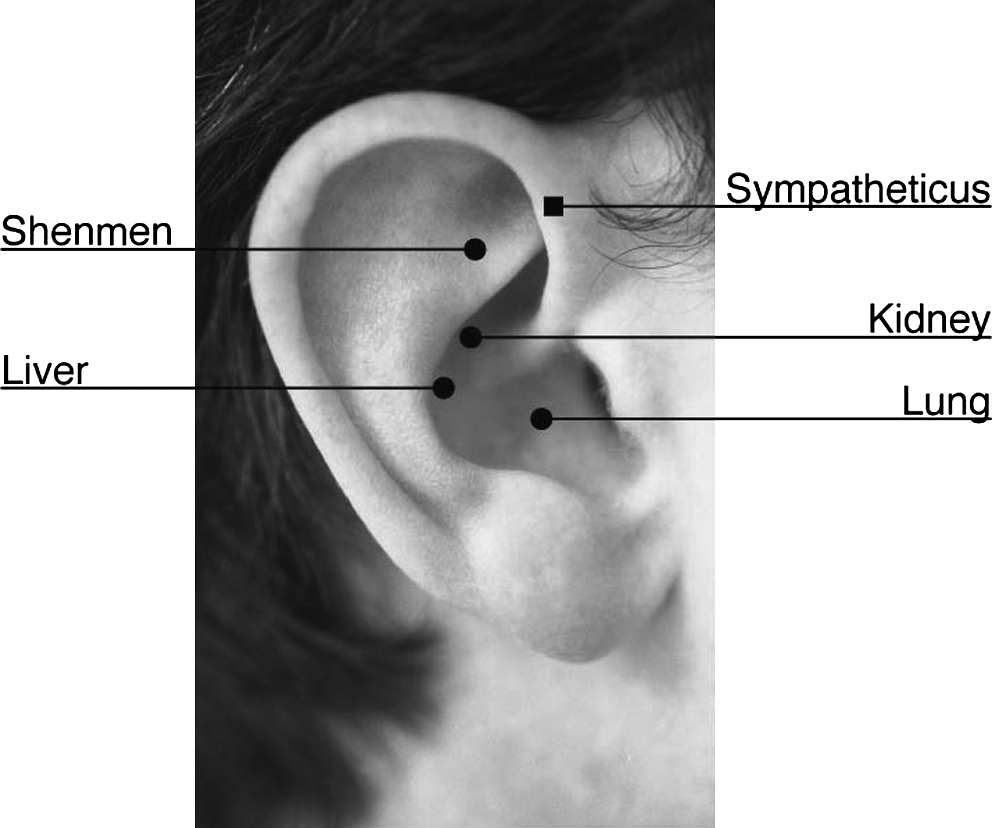
NADA Ear Acupoints. NADA indicates National Acupuncture Detoxification Association.
Body Acupuncture: Low-Risk Patients and Stagnant Qi
Body acupuncture, being more logistically difficult than ear acupuncture, may be feasible only for selected patients: those who appreciate energy dynamics; are open to acupuncture; and are willing to be responsible for the uncertainty of a non evidence-based approach. In such patients, postoperative opioid use would be less of a standard intervention and more of a request-only option. Pneumatic compression stockings could be used for a few days in the hospital, but home compression stockings could be discontinued once the patient was up and about. Patients who do not taper their analgesics despite ear acupuncture would be disregarding fundamental energy dynamics and thus be demonstrating their unsuitability for body acupuncture.
The bottom line is that patients need to take both responsibility and concrete action to achieve energy alignment, or else forfeit their select status. For these select patients, in the immediate perioperative period, standard tendinomuscular acupuncture (TMM) protocols could be offered daily or even twice daily. 25 Since few needles are required, perhaps the nursing staff could administer the treatments. With hip surgery and a lateral incision, the GB-TMM is an obvious choice. Key points involve the Ting points GB 44, gathering point SI 18, with local focusing points around the scar site. Knee surgery might demand a greater variety of Ting points but the principle would be the same (Table 3).
KI 1′ is located on the base of the medial side of the 5th toenail, opposite BL 67.
After hospital discharge, acupuncture could switch to a more linear N−N+1 input into the zone of involvement: the front (Yang Ming-Tai Yin), side (Shao Yang-Jue Yin), or back (Tai Yang-Shao Yin), plus local scar points. A typical post–hip surgery protocol would be GB 34 (Yang Ling Quan) and GB 40 (Qiu Xiu), LV 3 (Tai Chong), TH 5 (Wai Guan), and MH 6 (Nei Guan), using high-frequency (100–150 Hz) electrical stimulation to induce movement on Yang, and local points around the lateral hip scar. A more needle-conserving option would be to simply balance the Shao Yang and Jue Yin in the affected leg, with points like GB 34 and LV 5 (Li Gou) and/or GB 29 (Ju Liao) and LV 10 (Zu Wu Li) across the hip joint, with similar electrical stimulation.
For peripheral edema in low-risk patients, the Four Gates (LV 3 and LI 4 Hegu) could be added. The colander technique (in which needles are placed superficially but evenly in multiple locations so that excess fluid drains out) is probably not a suitable in-hospital option. 26
Herbs
In the immediate postoperative period, Yunnan Paiyao could be a standard. It is a patent formula used widely in China (its specific contents remain secret, but it is widely thought to contain raw and steamed Tienchi Ginseng) to help cope with the shock of acute trauma such as surgery. 27 After a few days, Du Huo Ji Sheng Tang (available from K'an Herbals as “Meridian Circulation”) might be substituted and used for several weeks to move the Qi and Blood. For those with predominantly more Blood stagnation, Shen Tong Zhu Yu Tang might be a good alternative (Shen Tong Zhu Yu Tang and Mo Yao Xiang Sheng Dan are available from K'an Herbals as “Meridian Passage”).
Medium-Risk Patients: Qi/Blood Stagnation, Spleen Qi Deficiency
Medium-risk patients would be those with a constitutionally based long-standing decreased Qi and Blood flow, such as patients with varicose veins, an intermittent/mild cardiac dysrhythmia, or a high body mass index. This group of patients would be somewhat less suitable for body acupuncture, although ear acupuncture is always an option. Nevertheless, there may be some committed patients who demonstrate their suitability by taking concrete steps to shift themselves from medium-risk to low-risk in the months prior to surgery.
Preoperative strategies might involve herbal tonics and a series of bi-weekly acupuncture treatments to correct issues of Blood stagnation, Spleen Qi deficiency, or Dampness. Herbal formulas to address Blood stagnation (e.g., Du Huo Ji Sheng Tang) or Spleen Qi deficiency (e.g., Liu Jun Zi Tang or Bu Zhong Yi Qi Tang) might be used for several months preoperatively (these standard formulas can all be found at http://www.bluepoppy.com). Such patients should try to reduce their body mass index to <30 and discontinue any energy-stagnating drugs such as potent analgesics and nonsteroidal anti-inflammatories.
High-Risk Patients: Blood Stagnation, Kidney/Spleen Deficiency
Highest-risk patients, those with both Qi/Blood stagnation and Spleen/Kidney deficiency, are generally poor candidates for any kind of intervention although ear acupuncture may be offered. These patients would primarily include those who are elderly and taking multiple drugs for chronic disease management.
Case Study
A 60-year-old physician-acupuncturist underwent a cementless right total hip replacement performed under spinal anesthesia (Figures 5 and 6). In the immediate postoperative period, in addition to LMWH injections, he was given the standard regimen of long-acting hydromorphone and gabapentin, and experienced postanesthetic constipation and urinary retention. After discharge on day 3, he discontinued all analgesics other than aspirin (combined with compression stockings for VTE prophylaxis) and instead used acupuncture, herbs (Du Huo Ji Shen Tang), and therapeutic touch (starting with TMM treatments for a few days, then followed with linear N− N+ 1 circuits). Within a few hours of the first TMM treatment, his gastrointestinal and urinary systems recovered while simultaneously his postsurgical pain markedly improved.

Preoperative anteroposterior view of the pelvis demonstrating right hip advanced osteoarthritis, with complete loss of joint space and osteophyte formation.

Right total hip arthroplasty at 3 months postoperatively with the use of cementless titanium implants.
Discussion
Although theory and the author's personal experience would suggest that acupuncture might hold promise as an adjunct to standard total joint replacement postoperative care, the reality is that such a radically different approach to postoperative management might prove difficult to introduce in a more than sporadic way. Funding and organizational issues would certainly pose obstacles; insurance guidelines restricting the use of acupuncture in Medicare patients would need to be circumvented; frequent daily visits may prove difficult to arrange; and many orthopedic surgery departments might not be interested in the idea. However, such obstacles might not be insurmountable if ear acupuncture were the primary tool, and ward staff could somehow be incorporated into the treatment protocols.
Even after addressing these initial obstacles, much more work would emerge. Pilot projects showing promise would need to be followed up with randomized controlled clinical trials comparing acupuncture, aspirin, LMWH, and various combinations in suitable low-risk patients. As with all trials, significant patient numbers would be required, with any promising results being reproducible in different institutions. Many acupuncturists would find such a project far too challenging to contemplate, particularly since the double-blind randomized trial is not really a suitable way to study acupuncture. 28
Conclusions
Despite the generally held belief that pain is problematic and should be avoided, the standard regimens for postoperative pain management in joint replacement surgery tend to work at cross-purposes and may inadvertently prolong postoperative pain and compromise healing. A more creative approach for suitably motivated patients might be to minimize the use of opioid analgesics while combining acupuncture and other energetic techniques to enhance the flow of Qi.
Since acupuncture theory clearly relates pain to a stagnation of the Qi and blood, the use of stagnating drugs simply generates the need for more, gives patients the erroneous impression that they are in more pain than they actually need be, and may inadvertently increase the risk of complications. Such a curious conundrum has no easy solution, other than indicating the need for a radical transformation of the current medical and surgical paradigm to one that incorporates an energy viewpoint.
Though not likely to happen anytime soon, it may be important if some of these therapeutic options could be incorporated postoperatively as optional regimens for suitable patients undergoing elective joint replacement surgery. In the meantime, those who are interested and aware of such energetic contradictions may need to chart their own course.
Footnotes
Acknowledgment
Graphics were designed by Richard Greenwood, MA.
Disclosure Statement
No competing financial interests exist.