
Abstract
Abstract
Background:
The inadequately diagnosed and suboptimal treatment of primary headaches, especially migraines, are a clinical concern. Localization of primary headaches may be essential for diagnosis and treatment, especially acupuncture.
Objective:
To investigate a new method for localizing pain using New Developed Meridian (Gold Meridian) and Acupuncture Points of Korean Hand Therapy (KHT).
Design, Setting, and Participants:
This study was performed as one part of the physical examination at the Department of Neurology, Pusan National University Hospital in Korea from March 2006 to February 2008. Six hundred patients with primary headaches and without other neurological or systemic diseases were included. The patients were diagnosed based on the classification and diagnostic criteria of the International Headache Society. We checked both sides of the head and neck on Gallbladder Gold Meridian such as CM-1 to CM-10 and Urinary Bladder Gold Meridian such as CI-1 to CI-8 using a roller stimulator produced by KHT or the round tip of neurological examination tools.
Main Outcome Measures:
The exact location for diagnosis of the primary headache.
Results:
Patterns of pain localization of primary headaches were various combinations, migraine and tension-type and mixed pattern based on Gold Meridian and acupuncture points. The patterns were not simple but complicated in certain headache groups. Mainly involved Gold Meridians were Gallbladder and Urinary Bladder.
Conclusion:
The Gold Meridian and Acupuncture Points of KHT can help localize headache pain.
Introduction
Many problems exist in the management of primary headaches, especially migraine headaches. Even with much advance in anatomy, physiology, and pharmacology relating to the brain, the response rate of headache treatment is not adequate. High proportions of patients are undiagnosed and untreated and a high percentage of patients seeing physicians are in a state of underdiagnosis and undertreatment. A study on the underdiagnosis of primary headaches indicated that missed diagnosis and misdiagnosis involve not only patients with migraine, but also those with other primary headaches.9,10
There is a valid need for comprehensive approaches for treatment. Several strategies are available for the management of primary headache including nonpharmacological and pharmacological methods. Medications are the mainstay of treatment, while other methods are underutilized. Treatment with newly developed medications is well-tolerated and not associated with serious adverse events, but the success rate is not high.11,12
All patients need nonpharmacologic management; the extent and type is dependent on the patients, especially those who are intolerant of medication, those for whom abortive and preventive agents are contraindicated, and those who have not responded to drug therapy. Nonpharmacologic treatment may play a particularly important role. One of the nonpharmacological methods available is acupuncture; however, there are some controversies.13–17 Another pharmacological method is botulinum toxin injection. The botulinum toxin significantly reduced the frequency of headache episodes in the prophylactic treatment of migraine and chronic daily headaches. Its treatment of headaches has been demonstrated to be safe with minimal side effects and low discontinuation rates due to adverse events.18–25 Both have some unsolved problems such as specific indication, optimal site, dosage of botulinum toxin, or number of acupuncture needling, and also side effects.
The efficacy of treatment is less than 70% with medications or nonpharmacological approaches.26–30 This might suggest diagnosis and treatment are not satisfactory.
There are some studies on localization that are related to several kinds of headaches.31–34 One diagnostic criteria of primary headaches of the International Headache Society (IHS) is location, which has been underestimated. 35 There is no standard method to check tender points or pain areas on the head and neck. 36 Tender points should be confirmed for exact diagnosis and specific treatment such as with botulinum toxin injection or acupuncture manipulation.
In this study, we examined the importance of pain location for accurate diagnosis. In East Asian Medicine, meridian systems exist only in theory and their existence has not been proven.37–42 It was not applied objectively for diagnosis and treatment of primary headaches, which causes controversies over the efficacy of acupuncture.13,14,43 The efficacy rate of treatment can be improved if we make accurate diagnoses. For localization of a tender point or pain area, we suggest the use of Gold Meridian by Korean Hand Therapy (KHT) instead of Meridian of East Asian Acupuncture, which is complex to use. 40 To our knowledge, there have been no data on primary headache and Gold Meridian and Acupuncture of KHT.
Methods
This study was performed at the Department of Neurology, Pusan National University Hospital (Medical Center) in Korea from March 2006 to February 2008; 600 patients with primary headaches and without other neurological or systemic diseases were included. The patients were diagnosed using the classification and diagnostic criteria of IHS. 33 This procedure was explained to all patients before physical examination and consent was obtained. This study was reviewed and approved by the institutional review board of this hospital.
In order to determine the exact side and sites on physical examination, we checked both sides of the head and neck on acupuncture points on Gallbladder Gold Meridian such as CM-1 to CM-10 and Urinary Bladder Gold Meridian such as CI-1 to CI-8 (Figures 1 and 2) using a roller stimulator produced by KHT or the round tip of a neurological examination tool, reflex hammer, or turning fork (Figure 3).
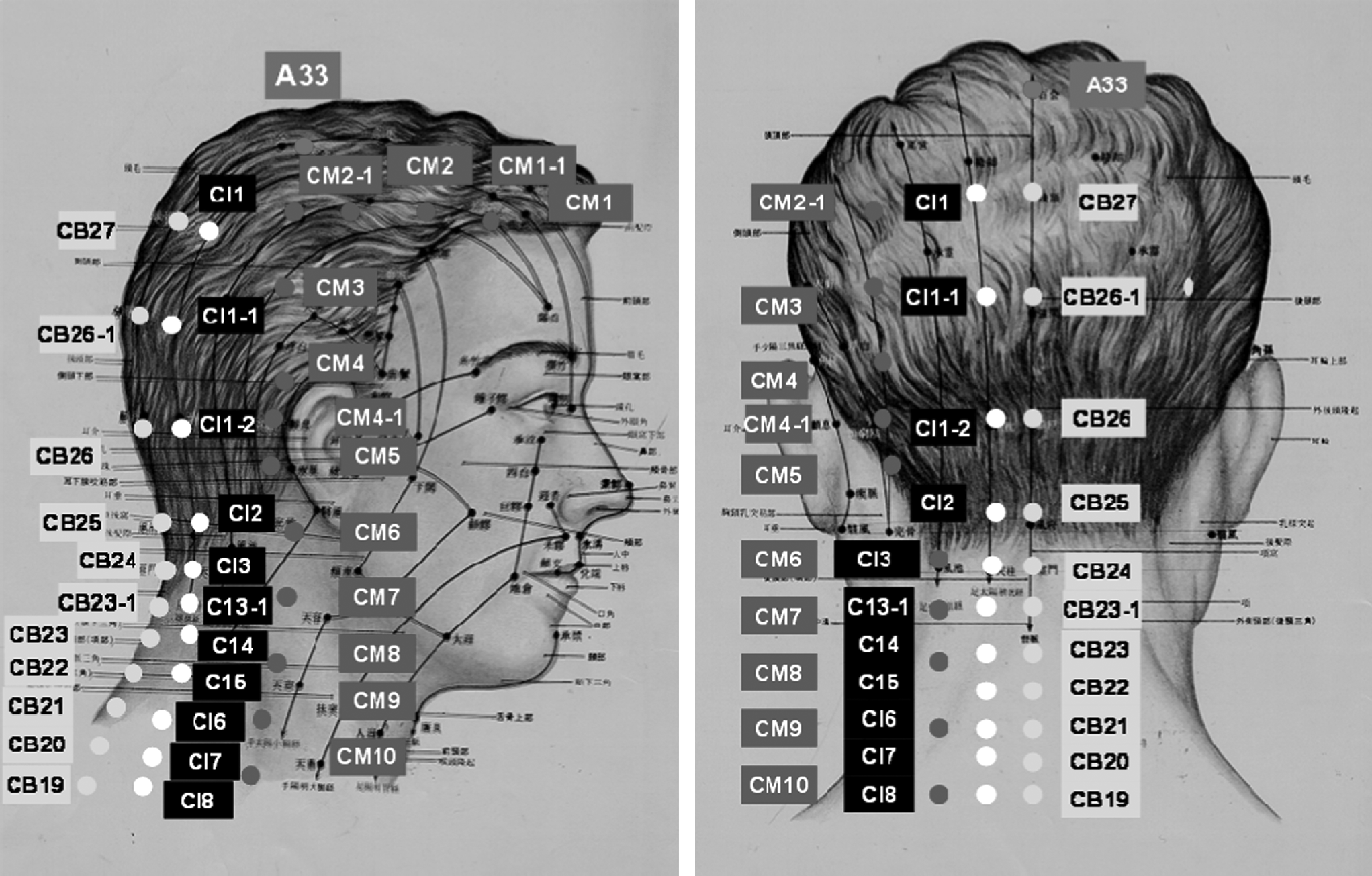
Gallbladder Gold Meridian (CM) and Urinary Bladder Gold Meridian (CI) are shown. Governing Vessel Gold Meridian (CB) is added as reference.
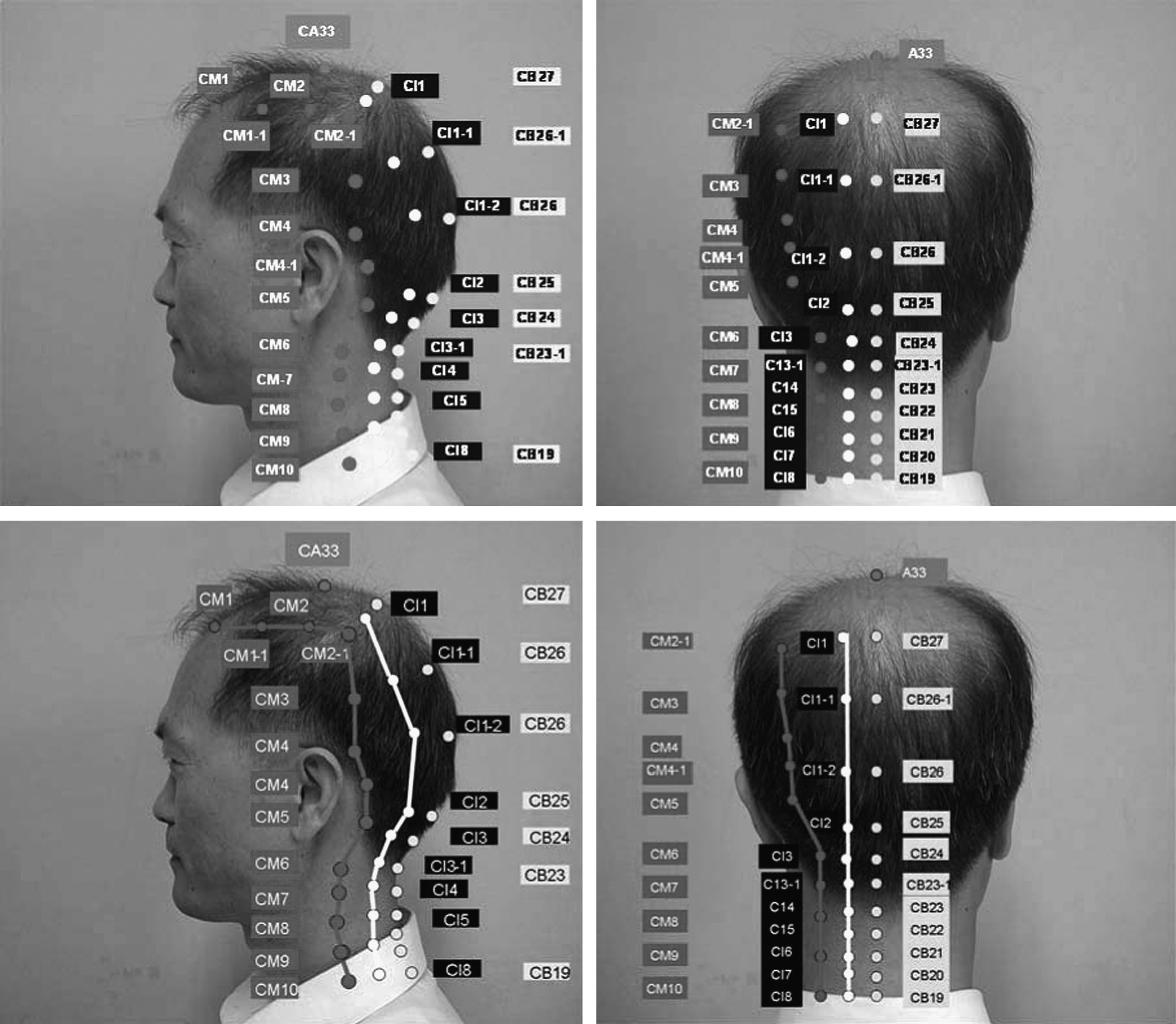
Gold Acupuncture Points and Meridians in migraine and tension-type headaches. Gallbladder (CM) and Urinary Bladder Gold Meridian (CI) are shown. Governing Vessel Gold Meridian (CB) is added as reference.

Several instruments such as a hammer, tuning fork, fountain pen, and products of Korean Hand Therapy are used for checking the tender points. Areas on the temporal, postauricular, and neck are demonstrated.
There are 6 Meridians of East Asian Acupuncture in each side of the head, over which only Gallbladder Gold Meridian (CM) and Urinary Bladder Gold Meridian (CI) were checked. 40 We confirmed the side and sites using Micromeridians of KHT.37–41
KHT and Gold Meridian Therapy
Korean Hand Therapy was discovered and developed by Dr T.W. Yoo in 1971. There are 14 micromeridians and 401 corresponding acupuncture points in the hands.37,38,40 Gold
Results
The locations of tenderness of 600 primary headache patients consisted of various patterns in migraine, tension-type, and mixed pattern based on Gold Meridians and Acupuncture of KHT (Figure 4). The tender points or painful areas were on one or both sides among the headache patients.

Various combinations of localization of migraine (M), tension-type headache (T), and mixed types are shown. Rt indicates right side; Lt, left side, and Both, right + left.
The 400 migraine patients showed tenderness when comparing right and left sides; the right side of migraine was more painful than the left side. The number of only the right side of Gallbladder Gold Meridian and Acupuncture points (CM) was 136 (33%); only left side of CM was 110 (28%); both sides of CM was 48 (12%); right side of CM and Urinary Bladder Gold Meridian and Acupuncture points (CI) was 20; right side CM and left side CI was 40; left side CM and CI was 16; left side CM and right side CI was 30. Of migraine patients, 27% showed several combined patterns such as Gold Gallbladder and Urinary Bladder Gold Meridians. Various combinations of CM and CI were shown among migraineurs.
The 200 tension-type headache patients showed that the left side was more predominant than the right side. Tension-type headache also showed unilateral predominance rather than bilateral. The numbers of right side tension-type headache were 67 (34%); only the left side was 105 (52%); both sides were 28 (14%). Tension-type headache showed importance of location. In comparing migraine headaches, a pure form of tension-type headaches was related to mainly the Urinary Bladder Gold Meridian.
Discussion
With a great deal of effort and with international cooperation, IHS published a classification and diagnostic criteria of headaches, 35 which may be used to diagnose headache patients. Some studies point out that underdiagnosis in headache patients may have negative consequences, enhancing the risk of progressive worsening of primary headache syndromes, increasing their impact on individuals and on society, and favoring medication overuse.2–8,44–46
The importance of rapport between physician and patient has been emphasized in order to obtain a detailed history for headache patients. To make a diagnosis of a primary headache, it is necessary to create a standard protocol for physical examination, because laboratory tests do not show specific findings.35,47,48
According to the classification and diagnostic criteria of IHS, the location is one important diagnostic criterion for a headache. 35 Most textbooks describe headache location briefly. There are a few articles concerning location of migraine headache and other headaches,31–34 but there were no descriptions on how to decide the location: side (left and right), sites (frontal, temporal, postauricular, occipital), and neck.
The exact location may be a good clue or guide to improve diagnostic accuracy and increase the success rate of treatment. It can be one method to solve underdiagnosis and undertreatment of primary headache. There is documentation of location in East Asian Meridian Acupuncture that has been used for a long time without scientific evidence.37–43
Palpation is an important part of the physical examination that has been underestimated in practice. How can the tender points be found in the head and neck? Detailed history-taking is not enough to improve underdiagnosis. According to East Asian Medicine, more than 100 points exist on meridians and acupuncture points on each side of the head and neck.37–43 Practically, our knowledge is lacking in how to use the meridians and acupuncture points in Western medicine, which is a quite different system.
For the diagnosis and treatment of primary headache to be effective, the New Modified Meridians and Acupuncture Points (Gold Meridians and Acupuncture points) of KHT are useful to detect tender points in the head and neck. It can define location such as side (right and left) and sites. We can save time to confirm location on physical examination. Headaches could be treated more effectively with pharmaceuticals such as botulinum toxin injection and nonpharmacological approaches such as acupuncture treatment. Gold Meridians and acupuncture points of KHT may be a useful diagnostic method on physical examination without any side effects or danger to the patient. We can utilize this for effective treatment of primary headache with optimal sites, small dosages of botulinum toxin, and fewer needling.
This study showed various combined patterns of migraine, which was quite different from that of tension-type headache. We could draw imaginary lines if we connected the tender points on the head, which might be related with Gold Meridians and acupuncture points of KHT. We believe that if the location is fully evaluated using Gold Meridians and acupuncture points of KHT, it can help to treat primary headaches more effectively. Pure form migraine and tension-type headaches can be controlled with medication as well as with botulinum injection and acupuncture. It also suggests that the efficacy of medication is limited or has partial effect in some headache patients, especially in combined mixed pattern of headaches.
Acupuncture is often used for tension-type headaches and migraine prophylaxis but its effectiveness is still controversial.13,14
How can we solve such controversies of acupuncture? If we have a concept of principles of acupuncture, objective diagnostic method, and treatment protocol, we can apply acupuncture effectively with fewer acupuncture needles. We can also undertake scientific studies of acupuncture. We need to prove scientific evidence based on principles or hypothesis.49,50
Korean Hand Therapy has been studied for more than 35 years.39–43 It presents New Modified Meridians (Gold Meridian and Acupuncture), which is easier to learn and to practice than East Asian Meridians from a clinical and research viewpoint. 40 In this study, we applied Gold Meridians and acupuncture points for the localization of primary headaches. There are 12 Gold Meridians right and left side, and 2 Gold Meridians, midline front and back. We consider the location in the aspect of right and left sides and various sites.
To our knowledge, this is the first trial to apply Gold Meridians to define the exact location of primary headaches. The pattern of pain location is not simple but diverse.
Conclusions
An improved protocol is needed to make accurate diagnoses of primary headache. It will bring increased efficacy of treatment. Location of pain may be a clue or guide for solving such a problem. It is not easy to decide the location of pain, but Gold Meridians and acupuncture points of KHT may be helpful. The pain locations of primary headaches are not as simple as the classification and diagnostic criteria of IHS. The pain location may be closely related with a Meridian system, which is different to trigeminal sensory territory. Accurate location (right or left side and site) is an essential component for diagnosis and treatment of primary headaches. We can increase the efficacy of treatment with a few acupuncture applications, a small dosage of botulinum toxin, or a few acupuncture applications as well as medication.
Funding
This study was supported by Pusan National University Hospital Research Grant, and Pusan National University Research Grant 2009.
Previous Presentations
Some portions of this paper were presented as a poster at the 14th International Headache Congress in Philadelphia (Pennsylvania), in 2009, and an oral presentation was given at the 28th Korean Neurological Association in Seoul, in 2009.
Footnotes
Disclosure Statement
No competing financial interests exist.
Acknowledgments
We are grateful to Jong K. Baik for his helpful suggestions and critical reading of the manuscript.