
Abstract
Abstract
Background:
Carpal tunnel syndrome is due to the entrapment of the median nerve within the carpal tunnel resulting in tingling, numbness, pain, weakness, and electrical sensations within the median nerve distribution. The distribution of the median nerve is typically the thumb and first 2 or 3 fingers.
Objective:
To demonstrate the incorporation of various acupuncture techniques in the treatment of carpal tunnel syndrome.
Design and Patient:
Case report of a 62-year-old woman reporting pain and weakness upon gripping in both hands in the distribution of her palm, thumb, and first 2 fingers on the palmar side.
Intervention:
Acupuncture was performed using the wrist barrier points PC 4, SI 6, LU 6, LI 9; LI 4 was added to create a French Energetic input. Myofascial release was also performed on the pronator quadratus muscle and interosseous ligament.
Main Outcome Measure:
Decrease in pain and weakness symptoms.
Results:
After the first session, the pain had decreased by 70% and the patient reported normal grip strength. Pain reduction persisted at 70% at 6 months.
Conclusions:
Acupuncture may quickly open energy blockages and release myofascial spasms contributing to carpal tunnel syndrome symptoms.
Introduction

The median nerve passes under the pronator teres muscle.
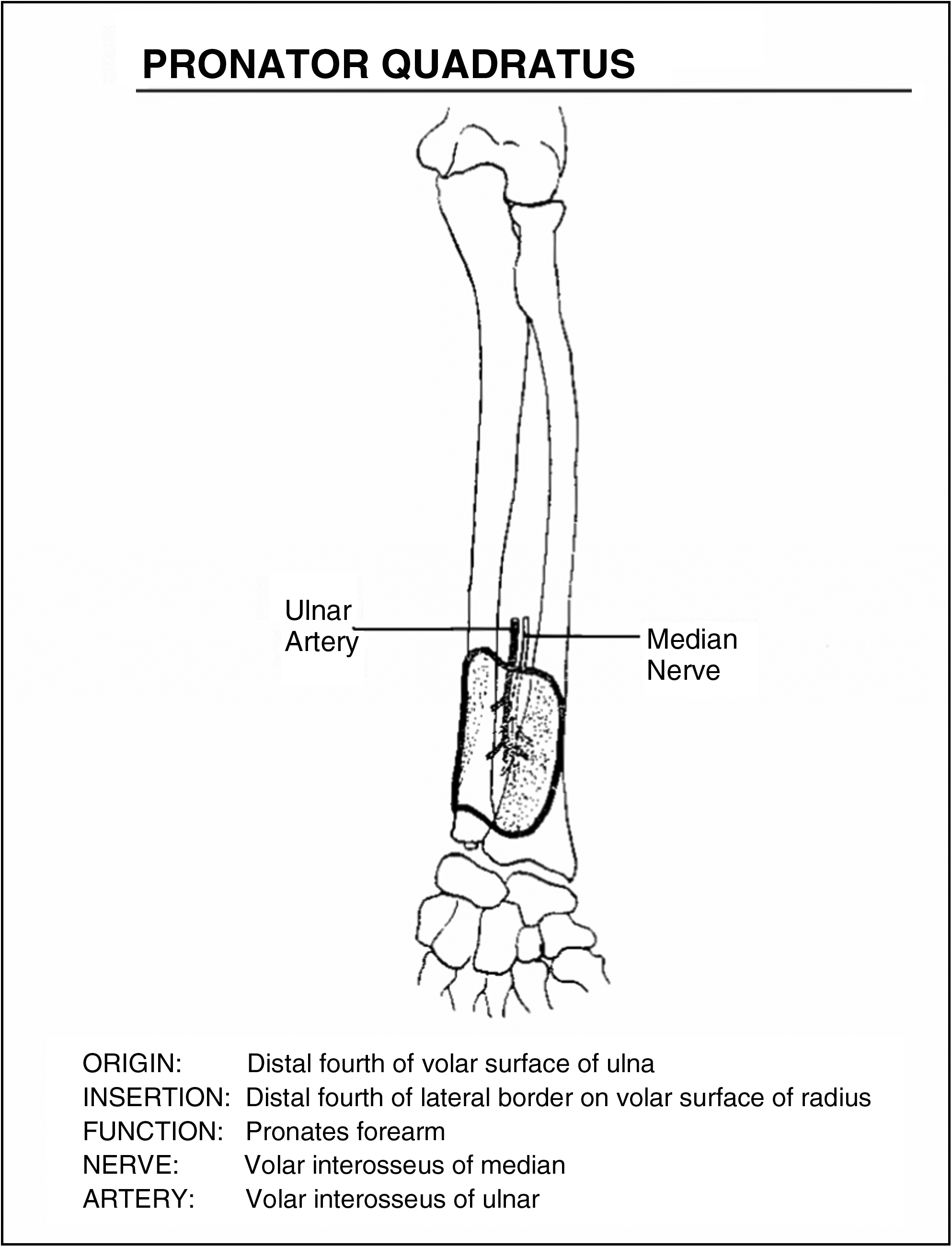
The median nerve passes over the pronator quadratus muscle.
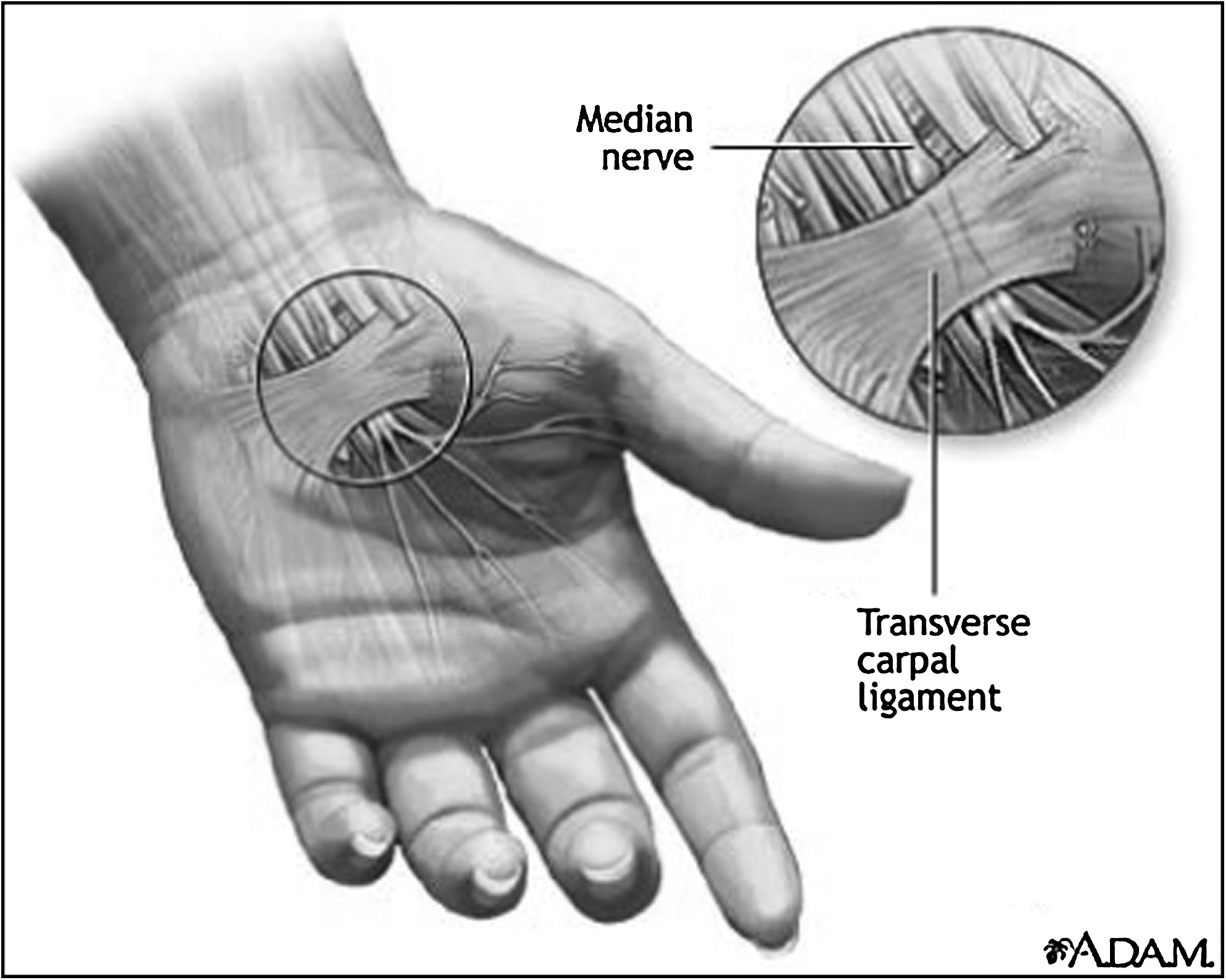
The median nerve passes through the carpal tunnel under the flexor retinaculum.
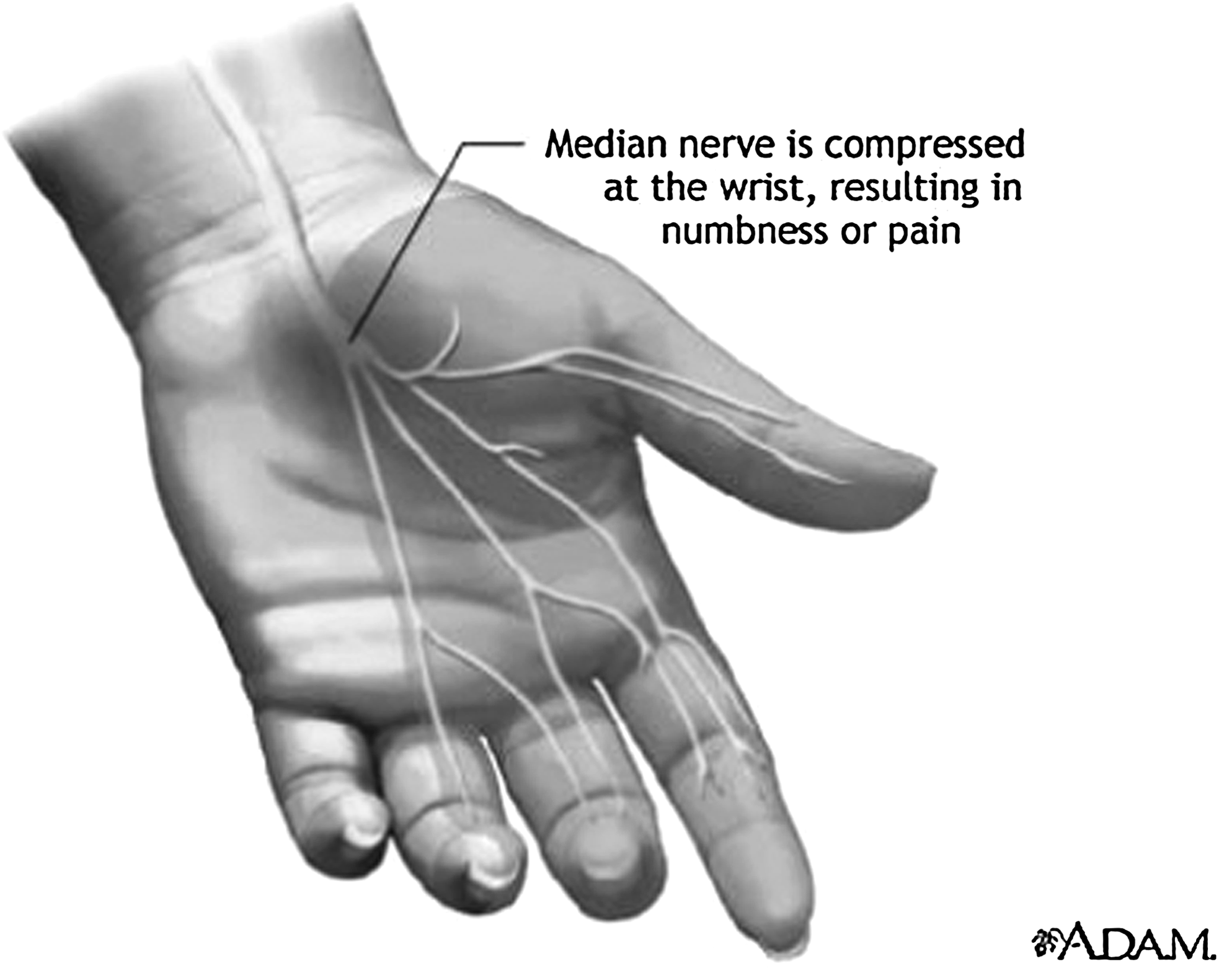
The sensory distribution of the median nerve.
Symptoms of carpal tunnel syndrome are due to irritation of the median nerve as it passes through the carpal tunnel. Irritation of the nerve is usually due to excessive pressure on the nerve. Common causes of excessive pressure within the carpal tunnel are repetitive use injury or irritation, cysts of the wrists, edema due to pregnancy, lymphedema after breast surgery, diabetes, and fractures or arthritis of wrist bones (Table 1). Women are affected more often than men. The age range is usually 30–60 years old. Symptoms are typically within the median nerve distribution. These symptoms include numbness and tingling in the radial side of the palm, thumb, and first 2 or 3 fingers. Pain can be experienced in these areas as well as extending upward toward the elbow. Fine finger movements can be affected. Patients may report a weak hand grasp due to pain. In severe cases of longer duration, muscle wasting and weakness in the thenar eminence may be found.
Physical examination can reveal numbness in the median nerve distribution, hand grasp weakness, a positive Tinel sign, and a positive Phalen sign. A Tinel sign is elicited by tapping over the median nerve at the wrist. This sign is positive if the patient experiences shooting pains from the wrist to the fingers. A Phalen test is performed by flexing the wrist forward to 90° for 60 seconds. The test is positive if the patient experiences numbness, tingling, or weakness. Electromyographic testing is normally done to evaluate the nerve conduction. Wrist x-rays can be done to rule out other underlying medical conditions.3–6
Case Report
A 62-year-old woman, working as a nurse, presented with numbness and pain in both hands. She reported pain in both palms radiating to the thumb and the first 2 fingers. She had been experiencing intermittent numbness in the same areas. She also reported weakness due to pain and the fear of pain upon using her hands. She stated that the symptoms began 3 years ago and were intermittent at first. However, over the last 2 months, her symptoms were more intense and more constant. She had a steroid injection bilaterally, which diminished the symptoms for about 1 month.
The patient had no history of injury to her wrists. Her other past medical history included hypertension, skin cancer, and ovarian cancer. On physical examination, she had decreased sensation on the palmar side of the first 2 fingers. Her grip strength was decreased due to pain. She had a positive Tinel sign, and the Phalen test was positive at 10 seconds. There was mild thenar muscle wasting, but this was proportional to her forearm and upper arm musculature. There was decreased range of motion at her wrist joint, including pronation. Her pulse was regular, tight, and weak in the kidney and lung areas; her tongue was thin, pale, and moist.
Methods
This treatment concentrated on the patient's carpal tunnel symptoms. (Her other constitutional conditions were addressed at other visits.) The patient received 2 treatments 1 month apart. Seirin 0.20 mm × 30 mm needles were used at all points, except at the TE 5 point where a Seirin 0.25 mm × 60 mm needle was used (Seirin, Tokyo, Japan). The needles were inserted bilaterally in the direction of the corresponding Meridian and to a depth to achieve De Qi. The wrist barrier points PC 4, SI 6, LU 6, and LI 9 were used to open blockages at the wrist; LI 4 was added to create an N -> N+1 French Energetic movement. TE 5 and PC 7 were added, opening the Luo-Yuan shunt around the wrist. The TE 5 point was needled to a depth to feel a fascial click; this released the pronator quadratus muscle. The needles were not rotated and were left in place for 20 minutes.
Results
After the first treatment, the patient had a 70% reduction in her symptoms of pain, numbness, and grip weakness. She returned 1 month later for a second treatment. The same treatment was repeated. The patient reported a 90% reduction in symptoms. At 6-month follow-up, the patient still reported a 70% reduction in symptoms.
Discussion
The carpal tunnel is a narrow passage at the wrist. Inflammation of any structure in this area can lead to excessive pressure on the median nerve as it passes through the tunnel. Carpal tunnel syndrome can result, due to this pressure on the median nerve. Median nerve dysfunction can result in numbness, tingling, or weakness. Many medical conditions can contribute to this situation, from traumatic to autoimmune to degenerative in nature. Uniformly, these conditions cause inflammatory congestion in the wrist.
Various treatments have been tested for carpal tunnel syndrome. The first line treatment is wrist splints, which help rest the wrist and keep it in the optimal position to promote fluid and inflammation to drain from the wrist, in order to reduce the pressure within the carpal tunnel. Patients are also encouraged to change their daily habits to reduce the repetitive injury to the wrists. In the early stages these steps may relieve the symptoms of carpal tunnel syndrome. 7 Nonsteroidal anti-inflammatory drugs and corticosteroid injections can relieve symptoms for a short period. 8 Carpal tunnel release is a surgical option. A cut is made in the flexor retinaculum to relieve the pressure on the median nerve. Surgery is successful most of the time, depending on the duration and severity of symptoms. The recovery phase typically lasts several months. 3
Acupuncture is a non-surgical treatment option. In only 2 or 3 sessions, patients can have very good relief of symptoms. There is no recovery phase that can cause patients to miss work. A change of work habits to reduce repetitive injuries is still encouraged. Relief of symptoms can last several months. Treatments can be repeated as needed.
Carpal tunnel syndrome is an inflammatory condition of the wrist with energy blockages. I use the wrist barrier points PC 4, SI 6, LU 6, and LI 9 to open these blockages. 9 Also, the excess inflammatory fluid needs to drain away from the wrist in order for the pressure to be relieved from the median nerve. I also add LI 4, which controls the energy in the upper limb and is a good general point for relieving painful conditions above the waist. This also creates an N -> N+1 energetic movement in the French Energetics system. This can be needled into the abductor pollicis brevis muscle as well. Releasing this muscle will help reduce the tension on the palmar carpal ligament and subsequently relieve pressure within the carpal tunnel. LI 4 is also the Luo point on the Large Intestine Meridian. LU 7, Yuan point, can be added to activate the Luo vessel shunt to help disperse excess energy. 9 For “tight” wrists with restricted forearm motion, I choose from the PC 4, PC 5, and PC 6, and TE 5, TE 6, and TE 8 points. These points can be needled deeply into the interosseous ligament and into the pronator quadratus and pronator teres muscles. 6 Releasing this ligament and these muscles will help reduce the pressure on the median nerve and the pressure within the carpal tunnel. Using TE 4 and TE 5 with PC 7 and PC 6 opens the Luo-Yuan shunt around the wrist. TE 5 is the Luo point on the Triple Energizer Meridian. A Luo vessel departs at TE 5 and travels to PC 7, the Yuan point on the Pericardium Meridian. PC 6, the Yuan point on the PC Meridian, sends a Luo vessel to TE 4, the Yuan point on the Triple Energizer Meridian. 9 For patients with sleep disturbances or with an anxiety component, I add HT 7. This point combined with PC 7 is very effective to calm an agitated patient. Auricular points can be added as well.
Acupuncture was an effective treatment for the symptomatic relief of carpal tunnel syndrome for this patient. In as little as 2 treatments, she experienced significant relief that lasted for at least 6 months. Larger studies with patients divided into subgroups according to variety of symptoms and/or severity of symptoms are needed.
Footnotes
Disclosure Statement
No financial conflicts exist.