
Abstract
Abstract
Background:
While there have been studies examining who seeks acupuncture treatments, there have not been any studies to see who returns for more treatments.
Objective:
This study was conducted to compare demographic, symptomatic, and syndrome differentiation among patients who came for one visit and those who came for five or more visits.
Design:
This was a chart review comparing 33 randomly chosen patients who came to the Oregon College of Oriental Medicine (OCOM) clinic for one visit to 39 randomly chosen patients who came for five or more visits.
Setting:
All patients were seen by student interns at the Acupuncture and Herbal Clinic of the OCOM.
Patients:
All patients were new patients to the clinic who came for their first visit during the spring and summer quarters of 2008.
Outcome Measures:
The two groups were compared with respect to a variety of demographic factors and presenting conditions.
Results:
Age was the major statistically significant difference between the two groups. There were other suggestive differences, but they were not significant.
Conclusions:
While there was only one statistically significant difference between the two groups, there were suggestive differences between the two groups that may help acupuncturists to discern better what types of people are more likely to become regular patients.
Introduction
Methods
From the patient files at the Oregon College of Oriental Medicine (OCOM) Acupuncture and Herbal Medicine intern clinic, the files of 33 patients who began treatment in the spring and summer quarters of 2008, and only came for one visit, were randomly selected. These patients were compared to 39 randomly chosen patients who started treatment during the same time period and who came for five or more treatments. Patients who were students or employees at the college were excluded. All patients signed a consent form that included allowing the data from their cases to be used for research and educational purposes. Upon initial intake to the clinic, all patients completed a Measure Yourself Medical Outcome Profile 2 (MYMOP2) form. These forms were validated for assessment of conditions presented. 2 , 3 From these forms, it was possible to determine the nature, duration, and severity of each patient's presenting condition. Information was also extracted from the patients' files regarding their ages, genders, residence in relation to the OCOM clinic, whether patients were receiving any kind of allopathic care, whether patients were taking any prescription drugs or supplements (e.g., herbal supplements, vitamins, etc.), number and type of Traditional Chinese Medicine (TCM) differentiations the interns diagnosed the patients, and how much patients paid for each treatment. It was then determined if there were any statistically significant differences between the groups with respect to these variables.
Results
The two groups were remarkably similar in some respects, yet different in others. The mean age for patients who only came for one visit was 39.5, with a median age of 39.5. The ages ranged from 11 to 74. The mean age of the patients who came for five or more visits was 52.4 with a median age of 59.5. The ages for this group ranged from 23 to 91. This was a statistically significant difference with a p-value of <0.0001, a t-difference −4.65 and degrees of freedom (df) of 47.
The group that came for five or more visits came for a total of 467 visits with a mean of 12.0 treatments. However, when this group was divided into two groups based on age—subjects under age 55 and those 55 and older—there was a slight difference between the two groups. The people who were under 55 came for an average of 11.1 treatments. The people who were 55 and older came for a mean of 12.8 treatments. While this was not a statistically significant difference, it was suggestive. The p-value was equal to 0.18; the df were 35, and the t-difference was 0.919.
Of the 33 patients who came for a single visit, 20 (60.6%) were female. Of the 39 patients who came for at least five visits, 29 (74.4%) were female. This was not a statistically significant difference; however, it is suggestive, with p = 0.2123 and a Pearson's value of 1.555.
The patients' zip codes were used to determine how far they lived from the OCOM. When comparing the distance traveled by the two groups, the patients who came for only one visit traveled an average of 91.3 (± standard deviation [SD] 289.7) miles to be treated, whereas the group that visited five or more times traveled an average of 7.7 (<SD 6.6) miles. In spite of the large difference in means, the p-value of the difference equaled 0.94, because of the very large SD in the group who only came for one visit. However, when the patients who traveled from outside the Portland metropolitan area (defined as traveling more than 20 miles to get treatment) were eliminated, the group that came for only one treatment was smaller by 6 patients and traveled an average of 6.7 (± SD 4.3) miles. In contrast, the group who received five or more treatments only shrank by 2 patients and averaged a travel distance of 6.3 (± SD 4.0) miles, which was similar to the distance traveled by patients who came only once. This meant that nearly 20% of the patients who only come for one visit lived outside the Portland metropolitan area. There was a strongly suggestive difference between the number (6) of patients who lived 20 or more miles from the OCOM, and only came for one visit, and the number (2) of patients who lived more than 20 miles from the OCOM and came for at least five visits. There was a p-value equal to 0.08 and a Pearson's value of 3.084.
The two groups paid similar amounts for their treatment. The patients who came only one time paid an average of $31.12 (± SD $7.40). The patients who came five or more times paid an average of $31.44 (± SD $5.90).
The patients who came only one time, reported and average of 1.6 reasons for their visit on their MYMOP2 forms. The first complaint averaged a severity of 4.2 on a scale of 1–6. For the secondary complaint, they averaged 4.1 on the same scale. The patients who came for five or more treatments reported an average of 1.72 complaints. This group had an average of 4.17 for the primary complaint and 3.52 for the secondary complaint.
The duration that patients reported of the chief complaint was similar between the two groups with one exception. In the group who came five or more times, a smaller percentage of patients had had the ailment for 3–12 months than in the group who came only one time (see Fig. 1).
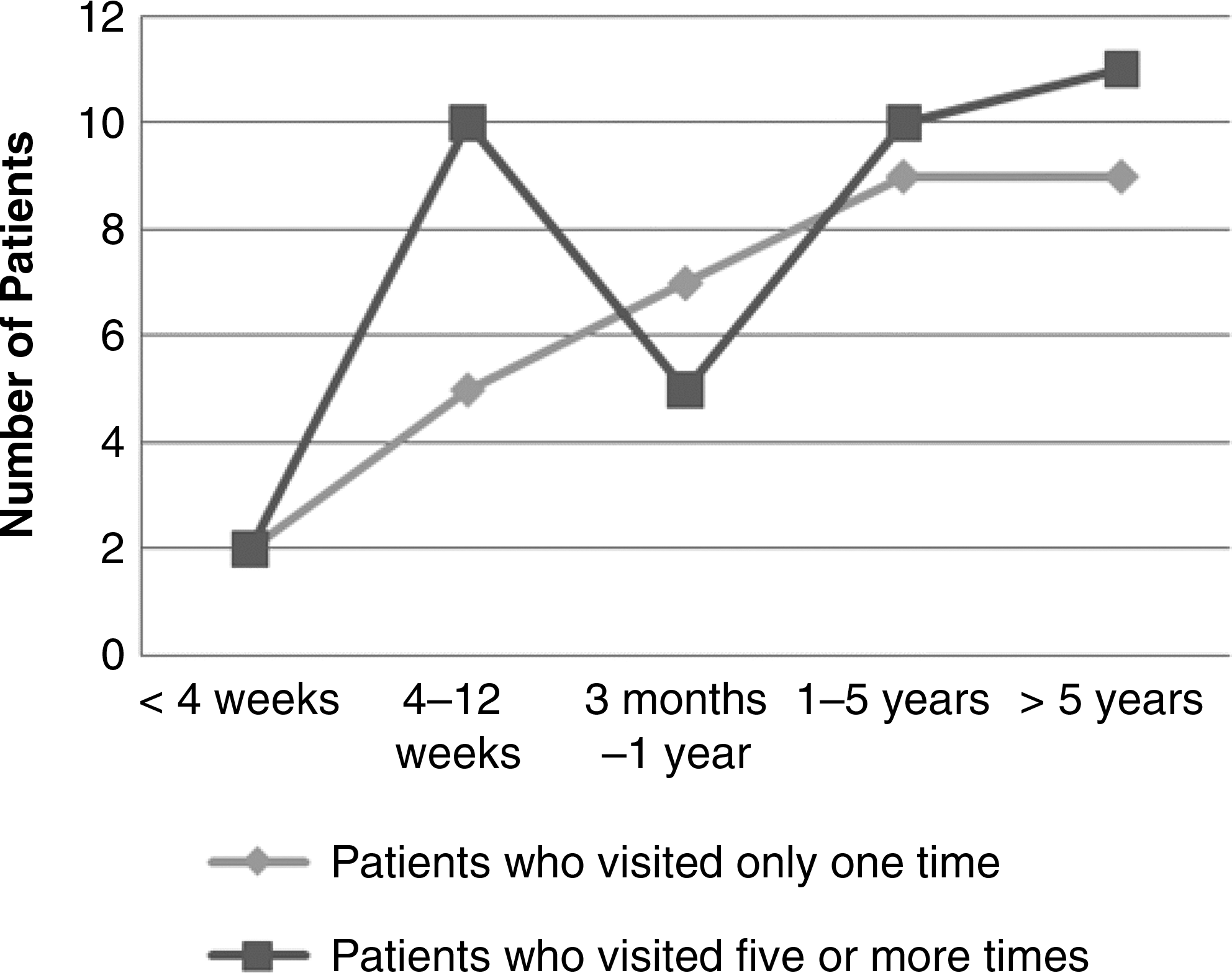
Duration of complaints.
Equal percentages (62%) of each group were under the care of an MD. Similarly, equal percentages (42%) were taking some form of prescription druga. A difference, however, was that, while 39% of patients who came only one time were taking some form of supplement (herbal supplements, vitamins, or others), 59% of the people who came five or more times were taking such agents. Again, this was not statistically significant, but was suggestive, p = 0.096 with one df and a Pearson's = 2.741.
The 33 patients who came for a single visit listed a total of fifty-eight complaints on the MYMOP2 forms. Of those fifty-eight, twenty-seven (46.6%) were for musculoskeletal conditions. Patients who visited five or more times reported seventy-two complaints. Of those, thirty-six (50%) of the complaints were musculoskeletal in nature.
Of the musculoskeletal complaints, the most common were back pain and neck pain. Other common complaints were shoulder pain and knee pain. There were no significant differences between the two groups in the kinds of pain they reported (see Fig. 2).

Number of reports of each musculoskeletal condition.
After pain, the next most common ailment differed between the two groups, but not significantly. Among the one-visit patients there were ten reports of an emotional nature, including depression anger, stress, moodiness, and anxiety. Among the five-visit patients emotional complaints were listed only four times, once each for depression, anger, stress, and anxiety. In contrast, fatigue was listed as a complaint by four of the patients who were treated five or more times, but not at all by those who only came once.
Nearly all of the other conditions listed by patients were listed only once in each group.
The TCM syndrome diagnosis of both groups is presented in Figure 3. The two groups were diagnosed with a similar number of TCM syndrome differentiations. For the group that came once, interns ascribed an average of 2.5 syndromes to the patients. The five-or-more visit group averaged 2.3 syndromes per patient.
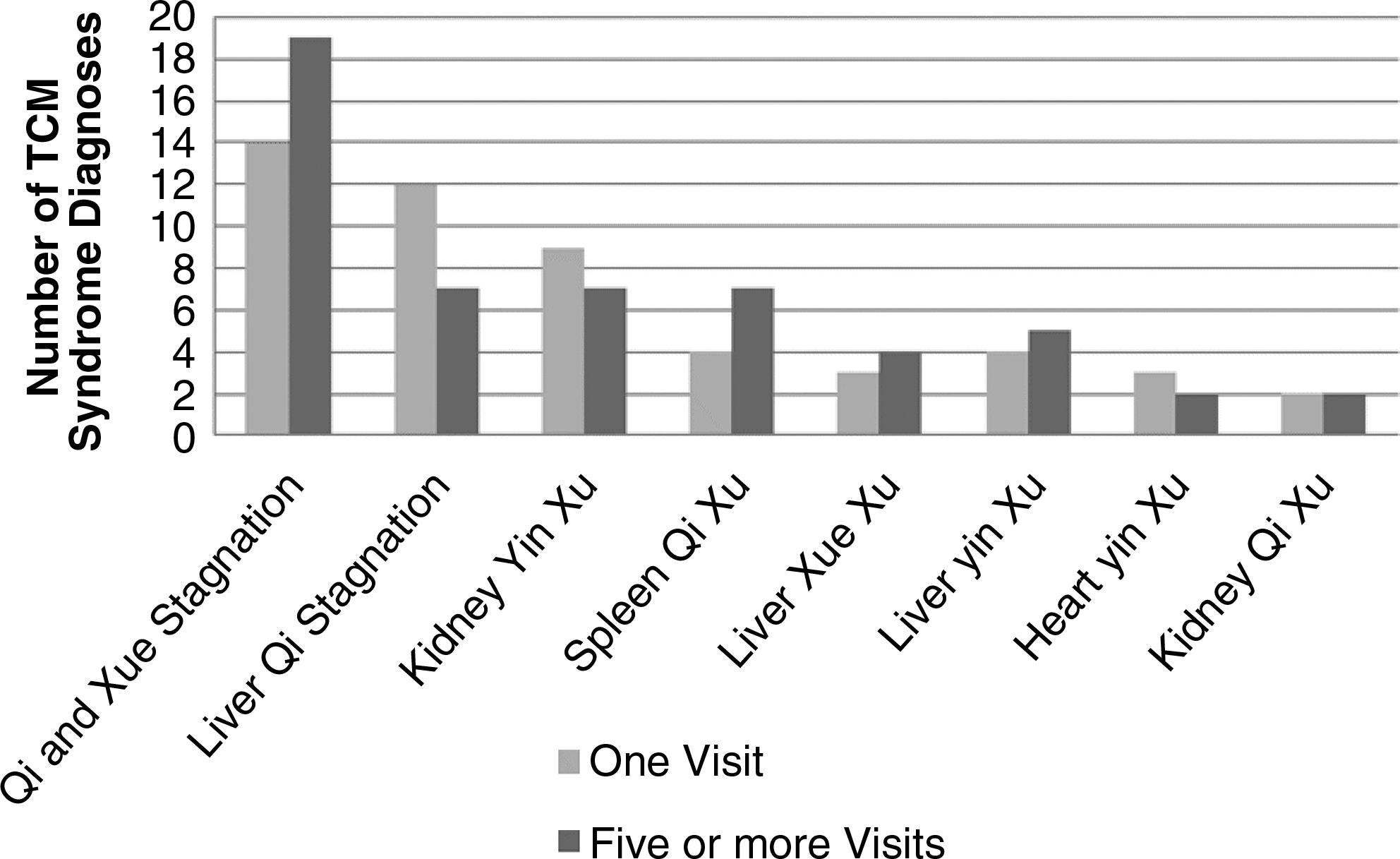
Number of Traditional Chinese Medicine (TCM) syndrome diagnoses.
The most common syndrome in both groups was Qi and Xue Stagnation; other common syndromes were Spleen Qi Xu, Liver Qi Stagnation, Kidney Yin Xu, and Liver Yin Xu. There were similar numbers of each syndrome in the two groups (see Fig. 3.)
Other syndromes were diagnosed zero to three times, but there were no significant differences. Often, when a syndrome was reported in one group, there were none reported in the other group.
Discussion
While there were few findings that were statistically significant, there were some that were suggestive of potential significance. Age was the primary indicator that a patient would return for five or more treatments. Furthermore, among patients who did return for five or more treatments, patients older than 55 returned more often. This may indicate that the OCOM and other acupuncture teaching clinics may be wise to target their marketing to these older patients. However, it could also reflect that perhaps older people seek medical treatment more often than younger people.
The vast majority of patients lives within the Portland metropolitan area; however, among those who came for only one visit, nearly 20% traveled more than 20 miles. Many of these patients came from so far away that it was impractical to expect that they would seek continuing treatments.
There was a suggestive result in the difference in the number of patients who were taking some form of supplement (herbal, vitamin, etc.). This difference, while not statistically significant, could indicate that patients who are already doing some form of self-care are more likely to seek treatment more often.
In all the other ways that the compared the two groups were compared, they were similar.
One surprising factor was that the two groups paid nearly the same amount for their treatments. At the time, the OCOM clinic used an honor-based sliding scale that allowed patients to pay according to income level. The rates were staged in three tiers, $39, $29, and $22. The fact that there was no significant difference in the amount each group paid seems to indicate that finances were not a significant factor in whether or not patients returned for multiple treatments.
In choosing inclusion criteria for the pools of patients to be compared, it was decided to only use patients who began treatment in the spring and summer terms. This was intended to reduce any possibility that the relative inexperience of interns during the fall and winter terms would have a negative impact on the likelihood that patients would return. However, an interesting situation was that none of the excluded patients, those who were students or employees, were randomly selected and their data were not used for this study. Had we included these patients and used a broader timeframe, especially the first quarter of the school year, it is very likely that there would have had a drastically different result. Most of the student body starts being seen in the OCOM clinic during their first quarter of school. Most of the students and employees of the college are significantly younger than the mean age of the test group and receive more than five treatments. Furthermore, given that this population also pays a significantly discounted fee, the mean payment would have been significantly lower. Finally, many students engage in the kind of self-care that was measured. These combined factors would most likely have given very different results.
Conclusions
While there were many different factors used to compare the two groups of patients, there was only one statistically significant difference, age. The mean age for patients who came for one visit was 39.5 years. The mean age for patients who came for five or more visits was 52.4 years. A strongly suggestive difference was found between the groups with respect to the percentage who were taking some form of supplement (herbal, vitamin, etc.). In the group who came for only one visit, 39% were taking some form of supplement. In the group who came for five or more visits, 59% were taking some form of supplement. There was also a suggestive difference between the two groups in terms of gender. In the group who came for only one visit, 60.6% were female. In the group who came for five or more visits, 74.4% were female. In all other respects the two groups were similar.
Knowing these differences may assist acupuncturists and Oriental Medicine schools to fine-tune their outreach to attract patients who will return for multiple treatments better.
Further research to compare patients using different criteria may be warranted. Other criteria could include what other practitioners the patients accessed (Western biomedicine, chiropractic, physical therapy, bodywork, etc.), how long it took for the patients to receive five treatments, and what treatment modalities (herbs, GuaSha, cupping, bodywork, etc.) were used by the student interns.
Footnotes
Acknowledgments
I would like to thank Richard Hammerschlag, PhD, for his invaluable assistance in developing this article. I would also like to thank Tim Chapman, PhD, for his help in selecting patient pools and explaining statistical analysis. Furthermore, the Clinical Research Committee at OCOM, made this article possible by implementing the data collection process. This project could not have gotten started without the participation of the individual patients who came to the OCOM clinic and the interns who treated them.
Disclosure Statement
No competing financial conflicts exist
This article was written as part of the Research Scholars Program, funded by an Acupuncture Practitioner Research Education Enhancement (APREE) grant from the National Institute of Health at Oregon College of Oriental Medicine.