
Abstract
Abstract
Rheumatoid arthritis (RA) is an autoimmune disease involving chronic inflammation of the joints. Conventional treatment often involves the early use of DMARDS, many of which have potentially toxic side-effects. For some patients, acupuncture may offer a creative alternative. Drawing from theory and personal experience, the authors suggest that an integrated approach, including acupuncture, functional and other energetic approaches, can occasionally reverse the disease process.
Introduction
Once RA is diagnosed, after the usual trials of nonsteroidal anti-inflammatory drugs (NSAIDS) and/or prednisone, patients are generally offered hydroxychloroquine or methotrexate. If those fail, newer disease-modifying antirheumatic drugs (DMARDS) are considered. All these drugs, however, tend to have significant side-effects. For example, hydroxychloroquine can be retinotoxic; methotrexate can be renal/lung/liver toxic, while leading to an increase incidence of lymphomas down the road; and the newer tumor-necrosis factor (TNF) antagonists can also lead to serious problems, such as liver failure, infections, and lymphomas. 2 Nevertheless, rheumatologists tend to recommend drugs early in the course of the disease, with the argument that, without treatment, cartilage damage and bony erosions will occur.
Much current research is directed toward developing new DMARDS, and there are now quite a few on the market (Table 2). But, while these drugs may block the immune dysfunction, they do not reverse it. So once started on immune modulators, patients tend to need the drugs long-term while the dysfunctioning continues outside of their awareness. In addition, many of these drugs are expensive. To spend what are often scarce funds taking drugs that reduce awareness and promote dependency is, in the authors' opinion, a less-than-optimal approach. A more creative option might be to try to restore a balanced immune system, so that drugs are not necessary. Indeed, the best way to avoid DMARD dependence is to never start taking such a drug in the first place. Perhaps this goal is achievable with Chinese Medicine (CM).
DMARDs, disease-modifying antirheumatic drugs; TNF, tumor-necrosis factor; IL, interleukin.
Rheumatoid Arthritis and CM
In CM, painful joints are referred to as Bi syndrome. Because CM really has no concept of genetic inheritance, Bi Syndrome is generally regarded as being the result of an invasion of pathogenic influences coming from outside the patient. Although patients may certainly inherit a constitutional predisposition to a specific condition, the disease will not necessarily manifest unless life circumstances weaken the patient's energetic defenses. Such circumstances might include things as: difficult childhood experiences weakening the Liver and Kidneys; stress, overwork, or poor nutrition affecting the Spleen function; or repeated coughs and colds compromising the Wei (defensive) Qi.
In the early stages of RA, when there is significant inflammation, the clinical picture is often one of Qi excess. However, this appearance is often false, being caused by a superimposition of Xie (pathogenic) Qi on the patient's Zhen (True) Qi. The actual energetic state of the patient is almost always one of Deficiency. Later, when the disease becomes chronic, the true Qi Deficiency can be more easily noticed. 3
External pathogens in CM are things such as Cold, Damp, and Wind. Such “weather pattern” pathogens are useful experiential descriptors of the symptom characteristics. For example, Wind moves around, Cold is painful and contracts, Heat rises, while Damp is heavy, fixed, and penetrating. Thus, an arthritic differential becomes: (1) Wandering (mostly Wind, (2) fixed (mostly Damp), (3) painful (mostly Cold), and (4) Heat (inflammation). 4 Because RA pain is often fixed and heavy, it is generally classified as either Damp Cold or Damp Heat.
What is Dampness?
Just like soggy ground after a few days of rain, Dampness characteristically pools and stagnates. When it invades the Spleen, it can cause upset stomach, nausea, reduced appetite, a swollen abdomen, and diarrhea. If Dampness enters the channels, it can give rise to stiff joints and heavy limbs; or it can transform into Damp-Heat and present as joint inflammation. Damp generally accumulates gradually, so that the effect of stiff joints is attributed to old age and/or osteoarthritis (OA). However, the appearance of swollen joints can be sudden, either because a certain threshold has been reached, or because there has been an abrupt shift of Damp from another site, such as could occur post-trauma.
On a physical level, Dampness spread diffusely may give rise to muscular aches and pains such as those encountered in polymyalgia or fibromyalgia. If focused into joints, the Spleen connection ensures a predilection for the T'ai Yin–Yang Ming circuit; hence, the commonly observed tendency to involve the thumb, index, and middle fingers. But other joints may also be T'ai Yin. For example, the anterior shoulders and elbows are certainly T'ai Yin–Yang Ming territory; hip pain often presents with pain medially in the groin, in the region of the T'ai Yin; knee pain usually evokes trigger points at the T'ai Yin–Yang Ming points Sp 9 (Yinlingquan) and St 35 (Dubi), and the big toe (in gout) is clearly T'ai Yin. Morning stiffness may be a characteristic of RA because T'ai Yin and Yang Ming energies are maximal between the hours of 3:00
On a mental level, Dampness is experienced as fogginess, cloudiness, or a feeling of “cotton wool” in the head. Impaired cognitive functioning may arise slowly as a result of depleted Spleen Qi brought on by overwork and mental exhaustion, or, more acutely, as the sequelae of a mild head injury or whiplash.
At the spirit level, Dampness might be understood as unmetabolized experience—unrecognized potential or soul tendencies that have not been permitted full expression by the developing ego.
In a previous article author M.T.G. discussed how the ego diverts energy into dump-sites, which may or may not be anatomically located. 5 With reference to RA, an arthritic joint could form an effective anatomical dump-site; generalized fluid retention might represent diffuse storage; and mental fogginess, a mental dump-site. Grouped together, all these phenomena might be understood to represent unmetabolized experience. In other words, all these things may be based on the ego's penchant to block the full expression of soul.
Transformational Opportunity
The onset of RA therefore presents a situation of both risk and opportunity. On the one hand, RA offers a unique chance for patients to explore and retrieve energies that may have been diverted sometime in the remote past. On the other hand, if symptoms are simply interpreted as pathological, then patients may see no option other than to take medications that are potentially toxic. Once a patient takes these drugs, the window of opportunity for transformation, which exists most accessibly in the early stages of the disease, can be missed.
Leaky Gut Syndrome
One theory that may help bridge the philosophical chasm between CM's Dampness and modern science is the concept of the leaky gut. Some researchers claim that increased intestinal permeability is a factor in dozens of diseases. 6 According to this theory, gut absorption can become compromised by a variety of triggers, leading to the absorption of incompletely digested proteins. Triggers can range from infections to drugs, to foods or traumatic events (Table 3). Reduced gut integrity leads to the absorption of partially digested proteins into the bloodstream. Such proteins form haptens, which, when attached to large carrier proteins, can activate immune cytokines and trigger a cascade of immune responses, leading to inflammation and the formation of antibodies against synovial membranes.
NSAIDs, nonsteroidal anti-inflammatory drugs; HIV, human immunodeficiency virus.
Although the leaky gut syndrome was originally a naturopathic concept, it has been incorporated into functional medicine, which has linked the syndrome to a whole range of immune dysfunction disorders, including asthma, diabetes, lupus, RA, multiple sclerosis, and Crohn's disease. 7
It is worth noting that some of the most common drugs used to treat RA can themselves give rise to the syndrome, and so paradoxically aggravate the disease. That drugs can energetically exacerbate the very diseases they are supposed to treat is, in the authors' opinion, an underappreciated phenomenon. But it is a predictable byproduct of the body's homeostatic mechanisms. Indeed, the difficulty can be applied to many drug classes, ranging from antidepressants 8 and anxiolytics, 9 to antihypertensives, 10 analgesics, 11 and even antibiotics. 12
Dmards and Spleen Qi
An exploration of the side-effect profiles of common DMARDS reveals that many of them have a tendency to aggravate Spleen Qi deficiency. Thus, both CM and leaky gut theory agree on the notion that drugs used to treat RA may be a factor in perpetuating the disease process (Table 4).
RA, rheumatoid arthritis; TCM, Traditional Chinese Medicine; TNF, tumor-necrosis factor.
Alternative Treatment Options
Consideration of the Spleen Qi Deficiency/Dampness/leaky gut rubric in the genesis of RA opens the door to a broad range of treatment options ranging from bacteriostatic antibiotics to food sensitivity testing, acupuncture, herbs, homeopathy, deep rest, and meditation.
Antibiotics
Rheumatic flare-ups have been attributed to infections with bacteria, such as Chlamydia13,14 and Mycoplasma.15–17 Indeed, Mycoplasma has been linked to both OA and RA. 18 Treatment with bacteriostatic antibiotics, in particular minocycline, doxycycline, or azithromycin, has been shown to reduce symptoms and even reverse a positive rheumatoid factor. 19 These particular antibiotics do not aggravate leaky gut syndrome.
Electrodermal Testing (EDT)
RA has also been linked to viral infections such as parvovirus B-19, 20 and hepatitis C. 21 Given that these do not respond to antibiotics, an alternative option might be homeopathic remedies designed to affect viral infections. Of course, such remedies can also be used to target Mycoplasma and Chlamydia. In this way, EDT can be a useful adjunct for identifying potential toxicities and their remedies. 22 EDT has grown out of EAV testing [electro-acupuncture according to Voll], 23 and, today, there are sophisticated computerized testing devices available. 24
Diet
Common foods thought to aggravate leaky gut syndrome include wheat, corn, and dairy foods. Other less-common culprits include citrus fruits, alcohol, chocolate, red meat, spices, carbonated drinks, and trans-fats. From a CM standpoint, foods that aggravate Damp and Heat include greasy food, dairy foods, shellfish, seaweed, eggs, sugar, alcohol, and excessive salt. Any of these foods could theoretically be a factor in RA. Although formal food allergy testing is available, it can be expensive and inconvenient to perform. An elimination diet can be a practical alternative, in which the patient avoids common allergens for 2 weeks, then reintroduces these foods one by one. 25
Adjunctive Therapy
A wide variety of natural approaches to RA have been advocated. For example, omega-3 fatty acid fish oils have been shown to be effective in a number of trials, 26 as have a number of supplements including vitamin C and E, zinc, bromelain, γ–linoleic acid, quercetin, and coenzyme Q10. 27
Herbal Therapy
Various Western herbs have been found to be beneficial for RA, including devil's claw, ginseng, valerian, blue flag, wild yam, and horsetail. 25 One currently popular remedy found to reduce inflammation in blinded trials, includes holy basil, turmeric, ginger, green tea, rosemary, bushy knotweed, Chinese goldthread, barberry, oregano, and scutellaria (Zyflamend, New Chapter).
Chinese herbal formulas can also be explored. Examples include: Du Huo Ji Sheng Tang (Meridian Circulation, Kan Herbs), Shu Jing Huo Xue Tang (Mobility 2: Health Concerns), Sheng Yang Ju Jing Tang (Phoenix Rising, Blue Poppy), and Zhui Feng Tou Gu Wan (Chase Wind Penetrate Bone Formula, Golden Flower). A detailed review of herbs is beyond the scope of this article, but interested readers can find extensive information from articles written by Dharmananda.28,29
Tu'ina
Chinese massage therapy can be remarkably effective, because it has the capacity to move Damp in ways that acupuncture cannot, working through direct pressure on affected joints. Although the experience can be very painful initially, perseverance brings results as the Damp gets mobilized slowly.
Deep Rest, Meditation and Qigong
Fatigue often forces RA patients to push themselves physically without considering that being stressed and worn out is what predisposed them to the condition in the first place. CM confirms this notion when it posits that overwork damages the Spleen. So, rather than fighting fatigue by reaching for stimulants, perhaps a better strategy might be to simply to get the rest the fatigue demands. The value of deep rest can be enhanced through formal meditation techniques, such as Trancendental Meditation,
Acupuncture
Although a Cochrane review concluded that acupuncture is not particularly effective for RA, 30 the reviewers' conclusion may be premature. Acupuncture for Bi syndrome is well-established in TCM literature,31,32 and conventional studies on acupuncture are fraught with logistical difficulties. The current effort to make acupuncture research fit an objective paradigm means that most randomized studies are too simplistic to be taken seriously, and, by and large, prove nothing. For example, one study on RA used a single needle on LV 3, 33 while another study used 6 standard points. 34 Both trials concluded that acupuncture did not work. Apparently, in both cases researchers were not aware that simplistic point formulas do not constitute acupuncture as it is generally practiced.
Getting results for patients with RA requires:
• Attention to each patient—This includes personalized treatments and a willingness to explore a range of therapeutic options. • Commitment and earnestness from patients—Those who give up after a couple of weeks generally get nowhere. Patients need to persevere with their explorations until they find out what works. • Optimal sector focus—This, in the early stages of the disease, may, in fact, be the T'ai Yin rather than the more commonly recommended T'ai Yang and Du Mai.
35
• Attention to the peculiarities of Damp accumulation—Being characteristically heavy and fixed, Dampness can be harder to shift than other energies. Wind, for example, often responds quickly to acupuncture; Cold can be gently warmed with Moxa and heat lamps; while Heat can be reduced using dispersing needles and/or cooling balms. Unfortunately, Damp does not respond to anything quickly. Moreover, if heated too much or too fast, the interstitial fluids can actually coagulate leading to even greater pain and fixity.
Subtlety, commitment, and perseverance, therefore, are the keys to success. In addition to picuring root, branch, and local Ah Shi points, the widespread Damp has to be mobilized and dissolved through a process that enables the Spleen to transform, the Kidneys to soften, the Lungs to release/disperse, and the Heart to vaporize. Concomitantly, the underlying Qi deficiency should be addressed through deep rest, lifestyle, and attitudinal changes. Success depends on a balanced and sustained approach involving all these elements.
Three Cases Using Acupuncture
Case 1
A 55-year-old woman attended a 10-day group residential chronic pain program. She had developed sero-negative RA ∼7 years previously shortly after her husband died of cancer. Medications she took included NSAIDS, prednisone, and weekly methotrexate injections. She wanted to stop taking these drugs and was keen to try dynamic interactive acupuncture (DIA). 36
The likelihood of significant unresolved grief pointed to a possible T'ai Yin imbalance. Therefore, her acupuncture treatment was focused initially on the T'ai Yin–Yang Ming axis, but also included other curious meridians, such as the Yang Qiao Mai. DIA Initiating points included BL 62, KI 6, Sp 4, and GB 40. Needle insertion was followed by marked myoclonic activity that continued intermittently for several days, and at the end of 10 days, she was almost pain-free. The patient returned for a second 10-day program, this time on a reduced dose of methotrexate and not taking any prednisone at all. During one spirit-level acupuncture interaction, she intuited that she had made a fundamental decision at the time of her husband's death to do whatever was necessary to ensure she never had to face the pain of a being involved in relationship again and that the development of RA had achieved this desired result. Following this realization, her symptoms subsided substantially and only recurred when she was under stress.
Case 2: Author's Experience
Author M.T.G. is a 62-year-old physician who developed swelling and pain in the shoulders, elbows, and hands, especially the thumb index and middle fingers, 6 weeks after a right hip replacement at age 60. His erythrocyte sedimentation rate (ESR) and C-reactive protein were elevated, his RA factor and anti-CCP were negative, but his polymerase chain reaction for Mycoplasma antibodies was positive. His symptoms persisted unchanged for several months, at which point he was diagnosed with sero-negative RA. He declined hydroxychloroquine treatment, and instead used doxycycline, acupuncture, Tu'ina, Qigong, Chinese herbs, and homeopathic remedies guided by electro-dermal testing.
His acupuncture treatments initially focused on the T'ai-Yin–Yang Ming axis using N–N+1 circuits, with additional local points in the arms, wrists and hands. A typical N–N+1 treatment involved points such as LI 4, LU 7, LU 1 and 2, LI 15, St 36, and Sp 6. As treatments progressed, evolutionary triangle balancing was introduced, mainly on the T'ai Yin as described by Buffington. 35 For example, a typical T'ai Yin balance included points such as LU 7, LI 4, St 36, BL 62 or SI 3, a couple of active T'ai Yang or Du Mai points (such as GV 14 or BL 11), and CV 17. (See Table 5 for points used for Case 2).
Another mainstay of treatment was Tu'ina, which was applied to active points on the T'ai Yin and Yang Ming channels, and to symptomatic joints. Although the experience was painful, and often accompanied by significant bruising, it proved to be very effective at mobilizing Dampness.
With this integrated approach, his symptoms were reduced gradually, and, over the following year, resolved completely.
Case 3: Another Author's Experience
Author C.L.S. is a 49-year-old physician who was diagnosed with sero-negative RA at the age of 31. At the time of diagnosis, her ESR, antinuclear antibody (ANA), and rheumatoid factor (RF) test results were negative. Two years later, she injured her neck in a motor-vehicle accident. By year 3, her ESR was 76, her ANA was negative, and her RF was positive. She declined conventional treatment and instead utilized acupuncture, herbs, Tu'ina, Feldenkrais, and Pilates for relief of pain with mixed results for 9 years. During that time, she completed the Helms course in French Energetics and began her studies of Classical Chinese Medicine (CCM) at USC with Dr. Anita Cignolini. At the age of 40, after the birth of her first child, she experienced severe joint pain/dysfunction and postpartum depression. Wrist X-rays showed advanced erosions. She used moxa on GV 4 to open her channels, build her Qi, and stabilize her mood; she also practised Qigong. She initially had to practice this sitting, as she was unable to stand because of her weakness and knee pain.
At age 41 she began treatment with Dr. Cignolini with CCM. After 10 treatments, C.L.S.’ pain decreased from 9/10 to 1/10. Her mood stabilized and her sleep improved. Over the next 2 years, she had 3 more series of 10 treatments. During that time, her left wrist flexion improved from 5° to 80°, her right wrist flexion improved from 0° to 20°, her ulnar deviation resolved, her hand strength improved, her toe extension and flexion improved, and her endurance and sleep improved. Her HAQ II score [RA Health Assessment Questionnaire, a measure of global functioning] fell from 21 of 30, to 0. Her depression lifted, and, as her energy returned, she added Pilates and Feldenkrais methods to increase strength and improve posture.
These treatments were individualized and rooted in TCM principles. Because she was energetically depleted, some care was required to avoid further depletion by excessive needling. This was accomplished by rotating different points along her channels during the first series of 10 treatments (for all points, see Table 6).
Day 1. Complete hand/foot treatment was performed using all Baxie/Bafeng points and an extra Shangbaxie point for RA (located as the most tender point between lateral Yaotongxue (N-UE-19) and TH-3 (Zhongzhu) between the fourth and fifth metacarpals (Fig. 1). Needles were inserted quickly, because the joints were very painful. The main points included PC 7, SI 6, TH 4, and TH 3.
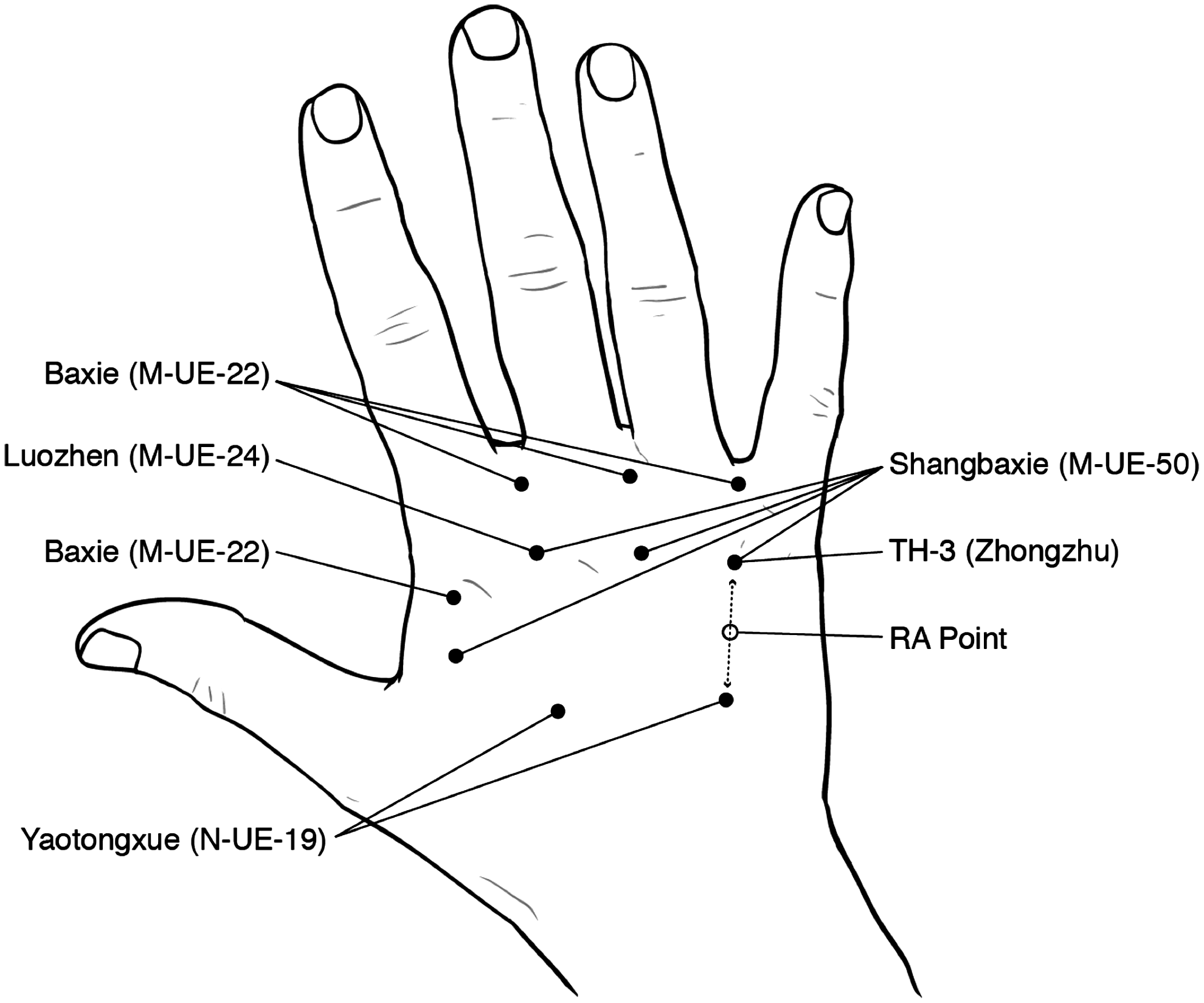
Some hand points mentioned in the text.
PC 7 is one of the 3 Yuan points of the hand used to assist in all hand problems
SI 6 is the Xi-cleft point of the Small Intestine Channel. Xi-cleft points are where the Qi and Blood, which flow relatively superficially along the channels from the Ting points, gather and plunge more deeply.
TH 4 is the Yuan source point of the Triple Heater channel. This point's main clinical application is in the treatment of contraction, stiffness, and pain along the entire length of the channel including the hand, elbow, arm, shoulder, neck, and back. TH 4 is one of the main points used to treat disorders of all five fingers, especially when characterized by contraction and pain.
TH 3 is the Shu stream and Wood point of the Triple Heater channel.
Baxie/Bafeng points are useful for arthritis.
Shangbaxie points lie proximal to the Baxie points on the dorsum of the hands. These points are good for hand pain and arthritis.
Day 2. Her decreased pain permitted more needle manipulation. Knee points were added, including the “eye” of the knee in the center of the patella, which is a good point for all knee problems. St 36 and 34 and GB 34 and 35 were needled in Tonification (Xiefa); KI 9 was needled with Tonification followed by a little reducing (Bufa).
KI 9 is the Xi-Cleft point of the Yin Linking channel. This point is used for all situations in which the Xie Qi is stuck in the deep Yin. Bones are deep Yin, and the condition was Cold and deep in the bone.
ST-34 is the Xi-cleft point of the Stomach Meridian
GB-35 is the Xi-cleft point of the Yang Wei Mai. It is a good point to use for pain, inflammation, and other protracted diseases.
GB 34 is the influential point of the tendons. It can be used for any kind of tendon problem.
St 36 is the lower He-Sea of the Stomach and Earth point of the Stomach Meridian. It strengthens the Qi and Blood, Spleen and Stomach, and Wei Qi.
A needle was then threaded from GV 14 to GV 13 to unblock her neck, which had been injured in the motor-vehicle accident; Hua-To-Jia-Ji points were added on either side of GV 14 in the groove lateral to the spinous process; and GV 20 was picured to help all the Yang, the back and the neck (now that it was open post last treatment). All points were tonified gently, as it was too painful for strong stimulation. After two treatments, her pain increased, in particular, her knee pain increased. These exacerbations were addressed in the third treatment.
Day 3. GV 14 was again threaded to GV 13; BL 11 was used for bones and also to help strengthen the Lung Qi, which was Deficient from years of bronchitis; GV 9 plus Hua-To-Jia-Ji points ½ cun laterally were picured to open the chest. These points were painful but helped to calm her anxiety; LI 16, 11, and 4 were used to nourish the Qi and send the Qi down the arms, which had been constricted for many years; TH 3, 4, and 5 were used for elbow contractures and forearm numbness, while St 34, 35, and 41; LV 8; Sp 6; Baxie; and other local points were added for pain.
GV 14 to GV 13 unblock the neck and send the Qi down.
BL 11 benefits bones and joints, and regulates the Lung Qi.
GV 9 and nearby Hua-To-Jia-Ji points unbind the chest and stabilize the emotions.
LI 16, LI 11, and LI 4 promote Qi flow down the arm.
TH 5, TH 4, and TH 3 promote free flow of source Qi in the arm.
St 34 and St 35 nourish the Qi and are good for knee pain.
LV 8 nourishes Blood/Yin and is good for knee pain.
St 41 nourishes the Qi and increases appetite.
GB 34 and GB 35 helps reduce limb pain and improves the gait.
Sp 6 resolves Dampness and is good for both joints and bronchitis.
Day 4. After day 3, her sleep had improved and she had less anxiety. The needling became less painful. PC 6 was threaded to PC 7 to calm her remaining anxiety; GV 14 was again threaded to GV 13. Other points included BL 11, KI 6, LU 7, LI 11, and the RA Shangbaxie point.
Day 5. PC 7, KI 5, and BL 62 were used.
KI-5 is the Xi-cleft point of the Kidney. Xi cleft points treat pain and the Yin Xi-cleft point nourishes the Blood.
BL 62 is the coupled Master point of the Du Mai. This point opens the Yang motility vessel.
Days 6–10. Kidney points (KI 5, 6, and 7) were used but rotated on different days. LU 7 and LU 6 were used on alternating days; other points picured included LI 11, GB 35, and GV 14 threaded to GV 13.
Results for Case 3. Over a period of 5 months, C.L.S. experienced almost complete restoration of hand function, although some limitation in right wrist range of motion remained. The right wrist extended 30° and flexed 15°. There remained some weakness of the third metacarpal joint of the right hand. Her energy and depression improved and she returned to normal activities. She continued to treat herself every 3–4 months with acupuncture using the Yuan points of the wrist (HT 7, LU 9, and PC 7), KI 6 or 7, and GB 35.
In June of 2002, she had sweating and Heat in her upper body, especially the chest. Red raised areas appeared on her chest. This was the Heat being expelled from the Lung, which had been present since an episode of bronchitis from 1987. These symptoms continued for 3 weeks and then resolved.
C.L.S. returned for a complete treatment in October 2002, by which time the RA factor had reverted to negative, and again in September 2003. The Zhi-Ze (treatment principle) continued to be treating the root of the disease by strengthening the Lung, Spleen, and Kidney. She continued strengthening her hands by returning to piano playing, gardening, and yoga. At times of increased stress, an increased sensitivity may be noticed in the joints. When this occurs, she uses acupuncture or does more Qigong to resolve this sensitivity. Wrist X-rays taken in 2011, compared to 2001, showed straigtening of the fingers and no further progression of erosions.
Discussion
The idea that RA might potentially be reversible is not a widely accepted idea. To be sure, it is known that the condition may go through periods of quiescence. But that is not quite the same thing as reversal. In that regard, cases 1 and 2 above might be examples of remission rather than reversal; but case 3, in which there was a reversion of the RA factor to negative, cannot be dismissed so easily.
That two of the case studies involved the physician–authors is perhaps not surprising. Physicians have a reputation of being discriminating patients, and will sometimes reject treatments that they recommend for their patients. 37 That they occasionally do so speaks directly to their confidence, or lack of it, with respect to conventional treatment options.
But then, physicians are perhaps more aware than most of the long-term consequences of drug regimens, having seen some of those consequences first hand in their patients. Also, physicians might be less inclined to relinquish responsibility to colleagues whom they suspect, based on their own experience of practicing medicine, probably do not have all the answers.
Clearly, it is one thing for a physician to explore acupuncture personally, but quite another to recommend it to patients. Indeed, a consideration of acupuncture and other alternatives to standard RA therapy can lead practitioners into some muddy waters. Perhaps the foremost difficulty is the admonition that DMARDS be instituted early, because, if acupuncture is to have any real chance of success, it should be utilized before drugs are instituted, not after. One way over this hurdle is insist that patients to take full responsibility for their choice of a non–evidence-based approach even to the point, if necessary, of having them sign appropriate waivers.
A related issue of how long it might be reasonable to pursue acupuncture before reverting to conventional options is a delicate one that must, for the same reason, be left for the patient to decide. A potential difficulty is that the response to acupuncture is often slow, and patients may give up before any improvement occurs, concluding in the process that acupuncture does not work. This difficulty mirrors the Cochrane conclusions, albeit for different reasons. When patients give up too soon, they demonstrate a lack of earnestness and commitment, both prerequisites for a successful outcome.
A third issue is that no one approach fits all. RA is a spectrum of disorders, which manifest differently in each person. The astute physician should be open to a multipronged approach, which might incorporate a whole range of options besides acupuncture, some of which have been mentioned in this article.
Perhaps the biggest issue of all is the widespread belief that healing is not possible, and that the only thing to do is to take medications. This view is often reinforced by well-meaning physicians and friends alike. In that regard, it can be a huge help is to find someone—particularly one with a certain personal knowledge—who can support the notion that healing is a real possibility. If such limitations can be negotiated, the rewards are potentially enormous.
Conclusions
Despite huge advances in science's understanding of the mechanism (the “how”) of RA, it is unlikely that science will ever elucidate the root (the “why”) of the disease. This is because the root lies in the Tao, which, by its nature, is beyond intellectual understanding, beyond knowledge, beyond diagnostic labels and treatment regimens. That the “how” tends to stand-in for the “why” in conventional medicine simply supports a collective illusion that, when it comes to an illness, physicians know what is going on. In fact, as many physicians will freely admit, they do not really know what is going on. Their Aesculapian authority is largely built on shifting sands. Perhaps indeed, one reason physicians “practice” medicine is because they can never know anything for sure.
The interesting thing is that the principle of not-knowing is one of the core tenets of acupuncture—the Tao itself being symbolic of the great unknown. This philosophical point actually has practical therapeutic implications. Specifically, by being up front with the admission of not-knowing, an acupuncture practitioner can, paradoxically, get a little closer to the “why” of illness. Of course, such an approach dismantles the illusion of Aesculapian authority, but it can simultaneously empower patients to trust their own instincts should they have an inner prompting to explore alternative treatment options. Such an approach can still respect conventional guidelines, while putting those same guidelines into a wider context that honors patient autonomy.
Perhaps then, in some situations, with the right patient, acupuncture might be an acceptable approach to RA. Because, as the authors can personally attest, it is possible to reverse the pathological process giving rise to the disease. No doubt a cynic might argue that spontaneous remissions of RA occur, that a few anecdotal reports prove nothing, and that acupuncture is as useless as the Cochrane panel suggests. But people who have explored acupuncture successfully know differently. They know that there is another way to proceed. And, for at least these 2 physicians, that has been practice-transforming.
Footnotes
Acknowledgments
Figure 1 was designed by Dr. Greenwood's son, Richard Greenwood, BFA, MA (website: ![]() ).
).
Disclosure Statement
No competing financial interests exist.