
Abstract
Abstract
Background:
Phantom limb pain (PLP) occurs in up to 85% of patients who have amputations and significantly worsens their quality of life. PLP is extremely difficult to treat, and common pain treatment is rarely effective. This case report describes the use of Yamamoto New Scalp Acupuncture (YNSA) to treat chronic severe PLP.
Case:
A 59-year-old man presented to an outpatient pain clinic with a chief complaint of chronic severe PLP after the left-femoral lower-third amputation that he had 21 years before.
Intervention:
YNSA was performed on the points representing the cranial nerves.
Main Outcome Measures:
PLP intensity, duration, and frequency were monitored to determine if the patient gained any pain relief from YNSA.
Results:
During the week after the thirteenth YNSA session, the patient reported a decrease in PLP intensity from 9±1 before the treatment to ∼1 or no PLP at all. Following the sixteenth YNSA session, the patient reported a decrease in the average duration of PLP (0.5±0.25 minutes) from ∼ 13±11 hours to 30 seconds per incidence, with an intensity of ∼1. After the twenty-fourth session, the patient reported a sustained reduction of ∼50% in the frequency of PLP episodes.
Conclusions:
This is the first case report on the effective use of YNSA for the treatment of chronic severe PLP.
Intorduction
Military conflicts; and road, extreme-sport, and other accidents, for instance, are the main reasons for an increased number of wounded patients with single-and multiple-limb amputations.5,6 PLP frequently develops in these individuals.5,6 The precise etiology of PLP is yet to be determined. Possible contributing mechanisms include stump-related pathology, and spinal and cortical changes. 7 The underlying mechanisms of phantom pain are primarily related to peripheral/spinal dysfunction, and to supraspinal and central plasticity in sensorimotor body representations. 7
It is believed that focus must be placed on defining the treatment options that improve QoL of patients with PLP.5,6
Several invasive therapies for addressing PLP have been studied. 5 In addition, the ability of noninvasive approaches5,8 to decrease PLP and to improve QoL of patients with PLP was investigated. For instance, research has included the use of mirrors for treating pain. 5 In addition, use of low-frequency, high-intensity auricular transcutaneous electrical nerve stimulation (TENS) 8 and the application of TENS to the contralateral limb 9 have been examined. However, these studies lacked the data necessary to select the most efficient method for approaching this problem.
The present case report describes the use of Yamamoto New Scalp Acupuncture (YNSA) for treating chronic severe PLP. YNSA is a completely new concept developed around 1970 and was first reported in Japan in 1973. 10 The location of YNSA points is quite different from the location of points in Chinese scalp acupuncture. 10 YNSA is classified as a somatic representation or microsystem comparable to other well-known microsystems, such as ear, mouth, nose, hand, or foot acupuncture. 10
Case
A 59-year-old man who had had amputation of the left-leg presented at an outpatient pain clinic with a chief complaint of chronic severe PLP. This patient had a severely injured left leg as a result of a traumatic fall from a great height 21 years before. The severity of this injury led to the patient undergoing a femoral lower-third (above-the-knee) amputation.
In addition to PLP, this patient had left nephroptosis, hypertension, diabetes mellitus, duodenal peptic ulcer, discogenic cervical pain, hip osteoarthritis, bilateral medianus neuropathic pain, and shoulder pain. The bilateral medianus neuropathic pain and the shoulder pain were the result of his frequent and prolonged use of crutches. This patient did not have any of these concurrent disorders prior to the falling accident.
In the past, the patient had received invasive and noninvasive pharmacological and Traditional Chinese Medicine (TCM) treatments. A sympathetic blockade using a contrast material was not a treatment option for his chief complaint, 11 because he was allergic to iodine. All previous treatments reduced the intensity of the neck and back pain temporarily; however, they failed to affect his PLP.
Intervention and Outcome Measures
Treatment for PLP
Treatment was focused mainly on this patient's PLP, although the ability of YNSA to normalize the other imbalances in the patient was also taken into consideration. YNSA sessions were performed once per week using 0.25 ×30-mm, silicon-covered, sterile acupuncture needles (Best Needles, HaMillenium Chinese Medicine, Israel). Each session lasted for 20 minutes. The points that were selected for treatment corresponded to the cranial nerves (CNs) that matched meridians and Brain points (see Table 1). 12 This treatment is ongoing as of this writing.
Informed Consent
Oral informed consent for the publication of the present case report was obtained from the patient.
Outcome Measures
The outcome measures included reduction of PLP intensity, duration, and frequency of occurrences. PLP intensity was rated via a numerical rating scale from 0 to 10, in which 0 was defined as “no pain at all” and 10 as the “worst pain possible.”
At baseline, the patient rated his PLP intensity as 9±1. He reported his PLP duration as 13±11 hours, and the frequency of occurrences was measured per 24 hours.
The primary outcome measures were documented from the beginning of YNSA treatment throughout the treatment period covered in this article. Prior to each session, all the details related to the effect of the treatment were recorded carefully in the patient's file.
Neck and Abdominal Diagnostics and Treatment
The patient's left side was more sensitive than his right side, and, therefore, all the procedures were performed on his left side. YNSA neck diagnostics 12 was used to detect the points to be punctured on the scalp. The appropriate areas on the neck were palpated, and after a sensitive area had been found, the corresponding scalp point 12 was detected using a PS 3 Point Detector (Silberbauer, Austria) and punctured. Subsequently, an absence or a substantial reduction in the sensitivity of the neck area was ensured. YNSA modified abdominal diagnostics 12 was also used to test the sensitivity of the YNSA Brain points and to confirm the sensitive areas that were identified by YNSA neck diagnostics. Following the detection of each sensitive abdominal area, the corresponding scalp points were identified and punctured using same technique as in the neck diagnostics (see Table 1). Thus, an absence or a considerable decrease in the sensitivity of the abdominal area was ensured. 12
Results
According to the patient, improvement started after the first session. Following the fifth session, he reported a considerable reduction in the frequency of PLP during the day, but stated that there was no change at night.
All of his neck areas corresponding to CN I–XII, except for CN X (Vagus), appeared to be sensitive at least one time. However, the neck areas corresponding to CN I (Olfactory) and CN II (Optic) appeared to be sensitive constantly and frequently, respectively. In addition, the abdominal areas corresponding to the YNSA Brain points were were sensitive periodically. The acupuncture of all the used points triggered phantom pain of low intensity and short duration (∼10 seconds), followed by relief.
The patient reported a substantial sustained improvement in his QoL after his thirteenth YNSA session.
Outcome Measures (Fig. 1)
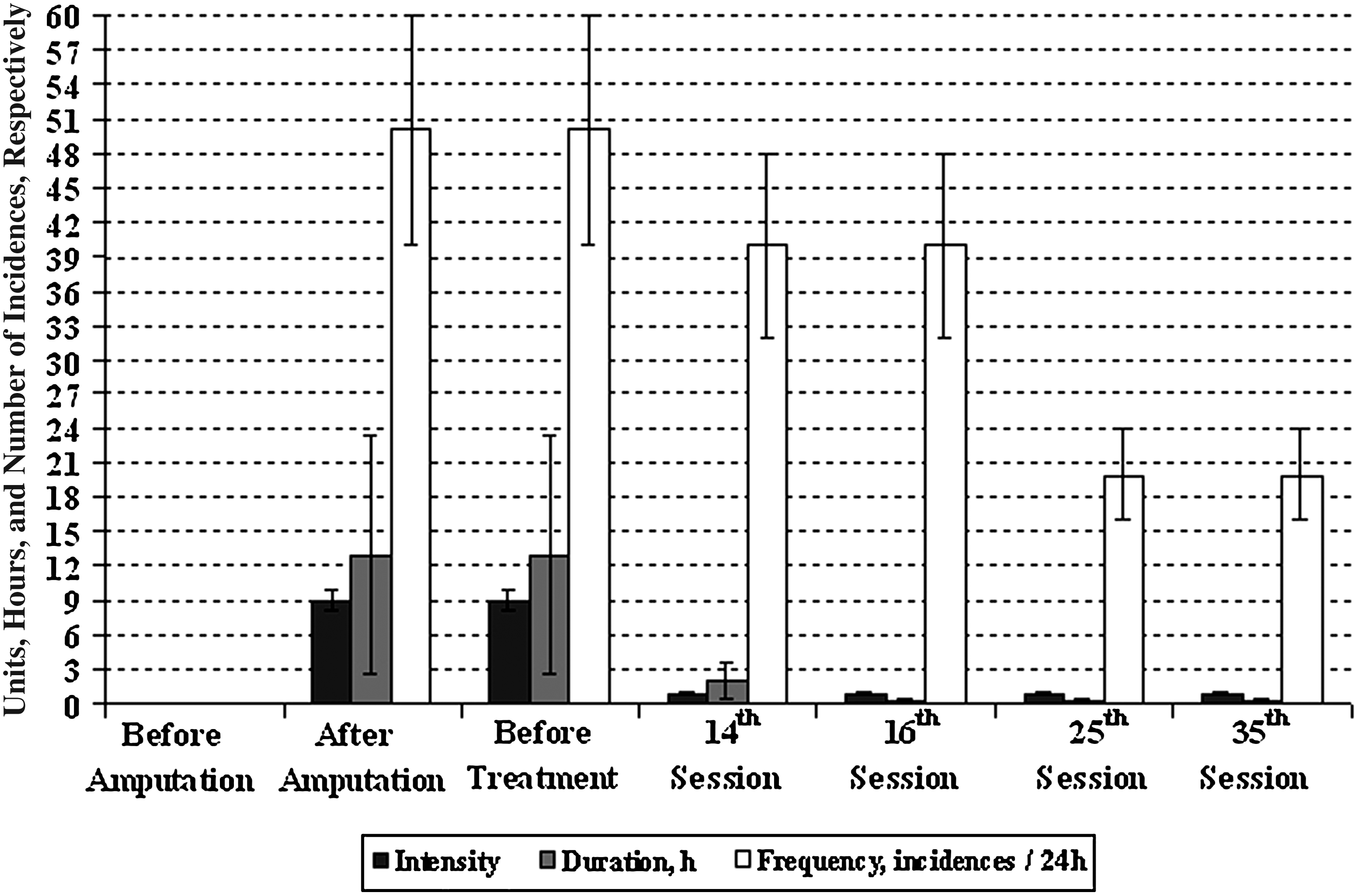
Phantom leg pain intensity, duration, and frequency. h, hours.
PLP intensity. The patient rated the intensity of his PLP after amputation (21 years ago) and prior to the beginning of YNSA treatment as 9±1. During the week after his thirteenth session, the patient reported a decrease in PLP intensity to ∼1 or no PLP at all. During the period from the thirteenth until the thirty-fifth session (22 weeks), his PLP intensity remained at ∼1.
PLP duration
Following the sixteenth session, the patient reported an average of 0.5±0.25 minutes decrease in the duration of his PLP, ranging from from 13±11 hours to 30 seconds per incident at the intensity of ∼1. No increases of the duration of PLP were reported by the patient.
PLP frequency
Following the twenty-fourth session, the patient reported a reduction of ∼50% in the frequency of his PLP. The frequency decreased from an average of 50±10 incidents per day to 20±5 incidents per day. By that time, each incident lasted for an average of 0.5±0.25 min (∼30 seconds), with the intensity of ∼1.
Overall response to treatment
This patient reported no worsening in any of outcome measures by the thirty-fifth YNSA session. Compared to the maximum possible intensity, and unpredictable frequency and duration of PLP incidents that the patient experienced prior to the beginning of the treatment, the results of YNSA treatment can definitely be considered to be substantial and prolonged (at least from the twenty-fourth to the thirty-fifth session, i.e., for 11 weeks) improvement in all of the outcome measures. Thus, the QoL of the patient was improved considerably.
Discussion
Invasive Treatment Methods
Saris and colleagues reported that dorsal root–entry zone (DREZ) lesioning can abolish phantom limb pain selectively but does not not stump pain. 13 About 40 % of the patients in their study had pain relief that lasted from 6 months to 4 years. 13 Nonetheless, 9 of 22 patients treated with DREZ developed minor but chronic neurological deficits. 13
Bittar and colleagues assessed the clinical outcome of deep-brain stimulation of the periventricular grey matter and somatosensory thalamus for the relief of chronic neuropathic pain associated with a phantom limb in 3 patients. 14 In that study, the patients were assessed preoperatively and at 3-month intervals postoperatively. A complete alleviation of the burning component of the pain, changes in QoL measures in all three patients, and reductions in opiate intake in 2 patients who required morphine sulfate preoperatively, indicated a statistically significant improvement. 14 Thus, the results showed a positive effect of deep-brain stimulation on PLP.
A case series and review by Viswanathan and colleagues showed that, for selected patients with PLP who have not attained adequate relief with medical management, spinal cord stimulation (SCS) can be an effective intervention. 15 However, long-term follow-up is needed to determine whether SCS produces sustained relief from PLP. 15
The results of a case report by Di Rollo and Pallanti showed that low-frequency repetitive transcranial magnetic stimulation over the motor cortex in the unaffected hemisphere ameliorates PLP with long-lasting analgesic effects. 16
Psychological Approach
A study by de Roos and colleagues investigated treatment of chronic PLP using a trauma-focused psychological approach. 17 The results of this study supported the idea of treatment aimed at processing unresolved trauma and pain-related memories. 17 According to these results, intensity of PLP can be reduced by decreasing the affective dimension of pain-related memories or by integrating the somatic-memory components. 17
Tens
Katz and Melzack evaluated the effect of low-frequency, high-intensity auricular TENS on PLP. In their study, TENS applied bilaterally to the earlobes resulted in a modest, yet statistically significant short-term decrease of PLP. 8 The duration of pain relief and the long-term efficacy of auricular TENS were not evaluated. 8 Perhaps, detecting sensitive points and treating these points specifically could have increased the effect of TENS treatment obtained in this study.
Giuffrida and colleagues reported a significant improvement in the perception of PLP and sensations, which was maintained at a 1-year follow-up after application of TENS to the contralateral (nonamputated limb) in 2 patients with PLP. 9 To confirm this positive finding, additional investigation involving a greater number of patients is required. 9
To date, there has been no systematic review of available evidence, and the effectiveness of TENS for addressing phantom pain and stump pain is currently unknown. 18
YNSA
YNSA was introduced ∼38 years ago. It is one of the most frequently used acupuncture microsystems. 19 Beneficial effects of YNSA treatment have been shown in uncontrolled studies in patients with hemiparesis after a stroke, in patients with musculoskeletal pain, and in emergency medicine. 19 In addition, in patients with poststroke hemiparesis, the effect of YNSA correlated with cortical activation, which was visualized by functional magnetic resonance imaging (fMRI). 19
The results of the present case report show a substantial effect of YNSA treatment on chronic severe PLP.
The correlation between the sensitive CNs and the occurrence of PLP described in the present case report remains to be analyzed and decoded. An understanding of the pattern that underlies this correlation may offer insight into the mechanism of PLP in general and thereby contribute to improving the treatment approach to this complicated syndrome.
Nevertheless, it appears that the sensitive CNs that were detected and punctured expressed a complex of imbalances, which were ameliorated by YNSA. Conceivably, YNSA treatment in the present study successfully influenced the direct and indirect causes of PLP.
Although the auricular TENS method seems to have the advantage of being less invasive than YNSA, the long-term efficacy of auricular TENS treatment was not investigated. Additional studies are necessary to compare the efficacy, long-term effects, cost-effectiveness, and other parameters of auricular TENS and YNSA used to treat PLP.
Conclusions
To date, this is the first case report on the effective use of YNSA for treating chronic severe PLP. Studies to confirm the results of the present report, which shows that YNSA treatment significantly improved PLP-related parameters, including QoL, are warranted. In addition, further investigation of the effectiveness of YNSA for treating PLP with concurrent disorders is necessary.
Footnotes
Acknowledgments
The authors wish to thank the patient for his willingness to grant the consent needed to publish this report. They also express their gratitude to Toshikatsu Yamamoto, MD, PhD, for consulting.
Disclosure Statement
No competing financial conflicts exist.