
Abstract
Abstract
Background:
Ting Well Points are commonly used for patients with acute conditions. For chronic musculoskeletal pain, which is caused by blockage of Qi in channels, the use of these points is believed to produce an excessive surge of Qi behind the blockage, which aggravates the pain.
Objective:
The purpose of this study was to demonstrate that concomitant use of Tonification, Ah Shi, and Meeting points could be used to relieve the Stagnation allowing the Excess Qi to flush out the blockage.
Materials and Methods:
Twenty cases representing a broad cross-section of various kinds of musculoskeletal pain were studied. The patients were treated at twice-weekly intervals for 8 weeks, with an assessment at each visit. An electronic point stimulator with a polarity switch was used to stimulate all of the points used in this study. The primary endpoint was an immediate response after the first treatment. The secondary endpoint was level of pain before the second treatment to assess duration of pain relief. The final endpoint was pain relief at 8 weeks.
Results:
Overall pain relief (87% reduction) after four treatments occurred in the patients. At 8 weeks, 15 patients had total pain relief. The other 5 patients had advanced structural damages, which limited their response to acupuncture. It was notable that there was no aggravation of pain in any case.
Conclusions:
In this 8-week study, Ting Well points, along with points used to to unblock channels, provided total pain relief in all cases in which irreversible structural damages were not present.
Introduction
In Chinese medicine the term Painful Obstruction Syndrome indicates pain or numbness of muscles, tendons, and joints from invasion of Wind, Cold, or Dampness. This is called Bi, which means obstruction to the flow of Qi and/or Blood in the channels. 3 A weak body constitution predisposes patients to this Syndrome, with the space between skin and muscles being open, which allows Wind to penetrate. 3
Addressing Painful Obstruction Syndrome requires a channel treatment by definition, but chronic obstruction requires treatment of internal organs. It is necessary to treat all three pathogenic factors and also the organs—the Liver when Wind is present, Kidney Yang when Cold is present, and Spleen when Dampness is present.4,5 Qiu Mao Liang CAc, advocates stimulating Kidneys and Governing Vessels, 6 because the defensive Qi has its root in Kidney Yang and the Governing Vessel.
The objective of this study was to demonstrate that Ting Well points can be used with benefits provided to patients with all chronic painful syndromes—this has been the experience of the author for many years. The usual accepted teaching is that these points are used for acute conditions, including emergencies, 5 but are not usually used for chronic painful conditions, because of the common belief that their use for chronic painful conditions will aggravate pain. This is because these points are the most distal points of the channels and there is a potential to create an excessive surge of Qi if these points are stimulated. All painful syndromes result from a blockage of Qi. A surge of Qi proximal to the blockage will lead to an Excess situation proximal to the blockage, thus, increasing the patient's pain. An attempt was made to obviate this problem by removing the blockage at the same time when the Ting Well points were stimulated. Using this procedure helps the Excess Qi flow with force. This was facilitated by stimulation at the Tonification or Source points, thus, flushing out the blockage.
The reason for using this method was to develop one fundamental principle for treating all musculoskeletal painful syndromes rather than using various differing “recipes” from textbooks.
Materials and Methods
Traditional Chinese Medicine acupuncture was used in this study.
Study Design
Twenty cases were selected from existing medical records in the author's two clinics in Melbourne, Australia, for the period 2008–2011. The clinics' human research committee considered this study to be a noninvasive audit and, thus, no approval was necessary. Verbal consent was obtained from all patients. Cases were selected according to two criteria: (1) The patient had musculoskeletal pain and (2) the patient's musculoskeletal pain was chronic, lasting for a minimum of 3 months; if the pain was intermittent, the pain was present for at least 15 days per month for 3 months.
The selected cases represent a broad cross-section of various kinds of musculoskeletal pain syndromes, which were:
• Rheumatoid arthritis (RA; Cases 1 and 2), with maximum pain in the right elbow (Case 1) and in the left knee with severe structural damage (Case 2) • Osteoarthritis (OA) of the knees (Case 3) • Low-back pain, with sciatica on the right side (Case 4) • Low-back pain of 40 years duration, with 15 surgical treatments involving the back (Case 5) • Chronic pain of the left shoulder without a history of repeated movements or injury, involving the Large Intestine and Small Intestine channels (Case 6) • Rotator-cuff syndrome of the right shoulder after repeated movements as a plasterer (Case 7) • Hemicrania continua in the left parietotemporal region (Case 8) • Hemicrania continua in the right parietotemporal region (Case 9) • Sacroiliac pain associated with “dragging down” of the ligaments caused by displacement of the pelvic organs (Case 10) • Pain in the sternal region radiating to the left and right chest, associated with local tenderness (Case 11) • Intercostal neuralgia on the left side (Case 12) • Intercostal neuralgia on the right side (Case 13) • Chronic neck pain associated with cervical spondylosis (Case 14) • Chronic neck pain following a motor car accident 6 years prior to the study (Case 15) • Pain in the finger joints associated with OA and CREST [Calcinosis, Raynaud's syndrome, Esophageal dysmotility, Sclerodactyly, and Telangiectasia] syndrome (Case 16) • OA of the right hip with near-total joint-space loss (Case 17) • Rotator-cuff syndrome on the right side (Case 18) • Carpal-tunnel syndrome, bilateral (Case 19) • Midline lumbar pain, chronic, involving the Governing Vessel channel (Case 20).
The methods used to address these patients' pain were:
(1) Stimulate the Ting Well points on both sides (reinforcement method). (2) Stimulate the Tonification point or Source point to boost the flow of Qi; this is done unilaterally on the side where pain occurs, using a reinforcement method to create a better momentum for the Qi to flow. (3) Reinforce the meeting point where this meridian meets another meridian, which could be a blockage point, using bilateral stimulation (points are discussed later in this article). (4) Reduce all Ah Shi points to remove blocks locally.
The stimulation time is 20 seconds for all points
Study Endpoints
The primary end point was immediate relief of pain after the first treatment. The secondary endpoint was level of pain before the second treatment to assess the duration of pain relief. The final endpoint was level of pain at the end of 8 weeks.
Assessments
Assessment of pain was evaluation on a scale of 0–10, with 10 being the level of pain prior to treatment. The patients were divided into 2 groups of 10 patients each; the grouping was done in such a way that similar cases were distributed in separate groups. In this way, each patient was treated with a different combination of points even if the presenting symptoms were similar. The first group (group 1) received three treatments involving Ah Shi points only; the second group (group 2) received three treatments involving the combination of Ting Well points, Tonification/Source, and Meeting points; no Ah Shi points were used for this group.
Level of pain was assessed immediately following the first treatment and again before the second treatment 3 days later. After three treatments, pain level was assessed again and, afterward the patients received treatments involving the combination of both sets of points. Level of pain was assessed at each visit. Points for treatment of Disharmony Pattern were added after the fifth treatment.
The total number of treatment was fifteen, but anyone who had a decidedly curative effect, could stop the treatment at that time. Final assessment of pain was performed after 8 weeks. Because the patients had been divided into different groups and responses to different groups of points used were assessed, it was possible to make a final selection of the most effective points for each particular patient.
Ting Well points are quite painful; so needling was not done. A laser could have been used, but it was very important that these points be stimulated by a reinforcement method, which is not possible with a laser. There is a hypothesis that stimulation below 5 mW could be reinforcing and above 8 mW could be reducing, but this has not yet been proven. Thus, an electronic point stimulator with a polarity switch was used. All points were stimulated using this instrument. The instrument was an Electro Stimulator Device, Pointer Excell II, made in Hong Kong for Lhasa OMS Inc., Weymouth MA. It used a single channel, microcurrent with 0–2 MA in the blue zone, 2–22 MA adjusting in the black zone. The pulse width was 220 MS+20%. It produced a Biphase square wave. The device was run on 9-volt batteries and had a polarity changeover switch for reinforcement and reduction.
All treatments were performed personally by the author who, among his other degrees, is a DM with registration in Australia as a specialist medical practitioner and acupuncturist (MastACU), and who has been practicing acupuncture as a main discipline since 1964.
Results
The primary, secondary, and final endpoints results are shown in Tables 1 and 2 and the accompanying graphs in Figures 1 and 2.

Average pain scores at each visit shown in
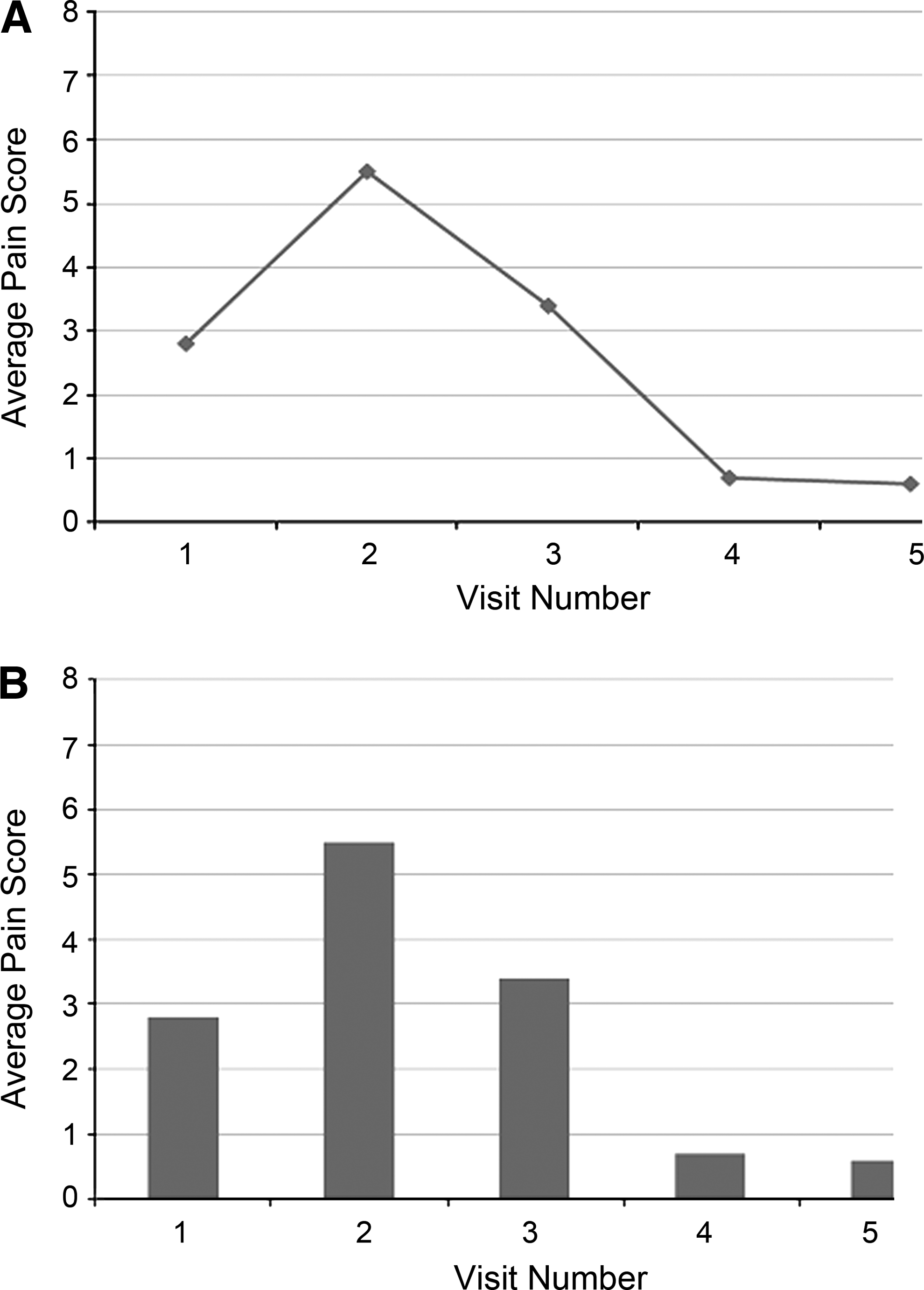
Average pain scores at each visit shown in
Ah shi points only.
Assessment of duration of pain relief after 1st treatment.
Ah shi+Ting Well points combination.
Combination of Ah Shi, Ting Well, and points for Disharmony Pattern.
Ting Well points combination.
Assessment of duration of pain relief after 1st treatment.
Ah shi+Ting Well points combination.
Combination of Ah Shi, Ting Well, and points for Disharmony Pattern.
As shown in the tables, these combinations of points reduced the patients' pain by 87% after four treatments. An attempt was made to fractionate the group of points to Ah Shi points only and combination of Ting Well, Tonification, and Meeting points to assess their relative efficacy in the first three treatments. It was not possible to do this. Any apparent disparity was the result of differing severities of pain and varying associated irreversible damages already present in some patients prior to starting the treatment. Combining the two groups of points in the fourth treatment definitely had a beneficial impact on the patients; however, addition of points to correct the associated Disharmony Pattern did not make much difference in reducing the patients' pain. The apparent small difference (in improvement) was the result of more treatments, but those additional points may have had the added benefit of correcting the associated Disharmony Pattern and hence the possibility of recurrences; and this made the treatment holistic.
In no case was there any aggravation of pain.
No attempt was made to compare the efficacy of this method to the beneficial effects of standard treatments given in textbooks, but one point is clear—this method is clearcut and simple, and, in effect, is second to none. Eighty-seven percent relief in four treatments for a chronic painful syndrome is plausible; anyone with a bit of experience in acupuncture would not expect anything to happen more quickly.
Of the 20 cases, 15 had total pain relief. With respect to the addition 5 cases, there were complicating factors involved. Case 2 had a combination of RA and advanced OA of the knee and needed knee replacement. Case 5 already had fifteen surgical treatments for his back and, that alone, made his back incurable. Case 17 had advanced OA of the hip with no joint space and had to have hip replacement. Case 19 had thenar muscle wasting caused by median nerve compression, and surgical treatment was mandatory. These cases were included to highlight the limitations of acupuncture in cases with advanced structural damage. Case 8 had to discontinue treatment because of an unrelated illness, but was already 80% better after five treatments.
Discussion
To treat Painful Obstruction Syndrome with this approach, the precise pathways of various meridians and fundamental knowledge about the various types of meridians are mandatory. When one speaks about meridians, this is usually interpreted to mean the twelve principal meridians, but the meridian complex actually includes:
• Twelve principal meridians • Branch meridians of varying numbers from each principal meridian • Fifteen connecting meridians (Luo) • Twelve muscle meridians • Twelve divergent meridians • Eight Extra meridians • A whole series of meridian complexes on the surface and in the interior of the body forming a meridian network.
Apart from the two midline Extra meridians—the Conception and Governing Vessels—the twelve main meridians are the only ones that have their own acupuncture points. The other meridians are influenced through the points of the principal meridians.
The Yang meridians control the exterior of the body; the Yin meridians control the interior of the body. They are coupled with one another; this connection takes place at the tips of fingers and toes.
Qi flows from one meridian to the other in succession, until a whole circuit is completed, thereafter flowing onto the first one again.
The coupled meridians are also connected by connecting meridians known as Luo meridians. These Luo meridians run over the superficial parts of the body between two the principal meridians they connect, thus enlarging the surface area of influence of the meridians. This fact must be considered when attempting to identify the meridians involved in a particular case.
The Muscle Meridians, which were important in this study, run superficially along the surface of the muscles. They pass from joint to joint. They can be considered as the entity through which the principal meridian exerts its influence over the musculoskeletal system. They follow exactly the same course as the principal meridians, but with two differences: (1) They have no connections with internal organs and (2) the flow of Qi in these meridians is always centripetal, from the extremities in an upward direction, irrespective of the direction of flow in the corresponding principal meridian. They have four meeting points as follows:
(1) The three Leg Yin meridians unite at CV 3. (2) The three Yang Leg meridians unite at St 7 (some people say this occurs at SI 18,
7
but the author has always used St 7 and obtained excellent results). (3) The three Yin Arm meridians unite at GB 22. (4) The three Yang Arm meridians unite at GB 13.
These facts form the nucleus of the method of treatment for Painful Obstruction Syndromes described in this article–stimulating a Ting Well point at the beginning of the meridian and stimulating the Meeting points at the abovementioned locations.
Divergent Meridians
Most of these divergent meridians emerge at the neck—the Yang divergent meridians rejoin the parent meridian; the Yin divergent meridians join their Yang counterparts, and this is the way the Yin meridians, which end at the chest, influence the head and neck through their divergent meridian connections with their Yang counterpart. For example, the Kidney meridian exerts its influence over the head through the Bladder meridian via a divergent meridian.
Extra Meridians
Of the Extra meridians, only the Conception and Governing Vessels have their own points and circulation of energy. They act as reservoirs of Qi; when there is Excess, they take Qi from meridians; when there is deficiency, they supply Qi.
Many parts of the body are not near any of the twelve principal meridians; but the whole meridian complex covers the entire body. 8
In many parts of the body, especially the neck, many meridians run close together and it becomes difficult to ascertain which meridian is involved. Extra meridians will be helpful in such situations.
Organ Effects on Meridians and Meridian Effects on Organs
A Liver condition can cause pain along the Liver meridian and stimulation of a point on that meridian can have curative or ameliorative effect on the Liver disorder. By the same token, a pathological lesion on a point on the Liver meridian can produce Liver symptoms.
Cellular Pathology and Meridians
Meridians have a controlling effect on the regions of the body they traverse, and this control is irrespective of the pathological processes or tissues involved. Hence, a patient with pain in the knee may have degenerative arthritis, inflammatory arthritis, tendonitis, muscle injury, or a skin lesion—the same points can be used irrespective of pathology. The pathological diagnosis gives a label to that sickness, but does not dictate the choice of points.
Knowledge of these basic facts is essential before considering treatment of Painful Obstruction Syndrome using channels.
All pain results from blockage to the circulation of Qi; when this blockage is present over a long period of time, there could be additional blockage of Blood. Qi Stagnation is associated with distending pain that can move from place to place; Blood Stagnation is associated with fixed pain that is of a stabbing quality. In cases of additional Blood Stagnation, as was shown in cases 8 and 9 (hemicrania continua produces fixed pain and is caused by Blood Stagnation), additional points UB 17 and Sp 10 had to be used to move the Blood. In case 20 (midline back pain) the Governing Channel was used, because that is the only meridian that passes through the midline of the back. This meridian has no Ting Well point, but for all practical purposes, GV 26 can be considered as a Ting Well point (which is used in acute emergencies as other Ting Well points), and by using the same principle, the patient's pain was relieved. GV 1 was used as the Meeting point where this channel meets the Conception Vessel. GV 4 was used as a Tonification point.
In all cases, pain relief was immediate and lasted for a day or two. Hence, in acute conditions where there is no Ben (root), this treatment alone may be sufficient. Because this study focused on Chronic Painful Syndromes, all had Ben, and that had to be treated separately to obtain long-term relief.
The clear advantage of this method is its simplicity. All one has to know is the meridian involved as well as the Ting well points, the Tonification/Source points, and Meeting points of each meridian. With this knowledge, any painful musculoskeletal syndrome can be approached with confidence. When meridians run close together, such as in the neck, the identification of involved meridian can pose a problem. An expert in Chinese diagnosis will help resolve this problem by using Tongue and Pulse signs. This is not everyone's preferred approach; an effective alternative method that everyone can use with success is to use Extraordinary Channels (however, any discussion on this is limited here because of space constraints and would require a separate article potentially in a 2013 issue of this Journal).
While this method is second to none in terms of efficacy, there may be acupuncturists who would prefer to use recipes from textbooks. These acupuncturists can continue to use their own methods, and this can serve as additional dependable tools to use for unyielding recalcitrant cases, which are not too uncommon in everyday practice. A classical example would be intractable shoulder pain. An acupuncturist might routinely use LI 15, TE 14, SI 9, SI 11, LI 4, LI 16, and St 38. If there is an insufficient response, the acupuncturist can use the method presented in this article as an adjunct treatment. If the pain were in the large intestine channel, the author would would use LI 1 (Ting Well), LI 11 (Tonification), and GB 13 (Meeting point). The points used routinely would be covered by Ah Shi points if they are relevant. Or if the pain was in the Small intestine Channel the author would use SI 1 (Ting Well), SI 3 (Tonification), GB 13 (Meeting point), and other Ah Shi points. From experience, it has been found that most cases of Large Intestine channel involvement will have associated Lung Channel symptoms and most cases of Small Intestine channel involvement will have associated Triple Energizer channel symptoms. Points are used following the same principles; the routine use of St 38 in all shoulder pains lacks basis. St 38 is useful in Large Intestine channel pain, because of the axis relationship between the Large Intestine and Stomach channels. If the Small Intestine channel is the culprit, the corresponding point to be used will be BL 58 for the same reason. Diligent use of points according to the channels involved will lead to more successful outcomes for any disease.
The widespread understanding that Ting Well points are to be used mostly in acute conditions is a myth; the belief that the use of these points for chronic painful conditions will aggravate the pain is also a myth. With proper selection of points as indicated in this article, these points can be used with advantage for all Painful Obstruction Syndromes with considerable success.
Conclusions
The use of Ting Well points need not be confined to treatment of acute syndromes; these points can be successfully used with confidence for all chronic musculoskeletal painful syndromes without fear of aggravation, provided concomitant use is made of points to unblock the channels, and the results are often quite extraordinary.
Footnotes
Disclosure Statement
No competing financial conflicts exist.