
Abstract
Abstract
Introduction:
Acupuncture is one of the most popular forms of complementary medicine. Previous studies have proven that traditional manual acupuncture is safe when it is performed by well-trained professionals. However, the safety of electro-acupuncture (EA) has not been well-evaluated.
Objectives:
This literature review was undertaken to assess the safety of EA.
Methods:
In October 2010, searches were conducted—using six electronic databases, three Chinese databases (CBM, CNKI, and VIP), and three English databases (PubMed, EMBASE and Cochrane Library)—to identify articles published between 1979 and 2010 regarding EA. Case reports, case series, surveys, and observational studies were considered to be eligible for inclusion in this review if they reported factual data on adverse events (AEs) related to EA. Review articles, translations, and clinical trials were excluded. Information on acupuncture points and AEs was extracted from the primary articles and entered onto a preformulated spreadsheet.
Results:
Fifteen articles met the inclusion criteria. In total, 44 cases of AEs after EA were reported. These AEs were classified into two categories: general AEs (n=7) and specific AEs (n=37). General AEs included 4 traumatic events, 2 cases of fainting, and 1 case of hyperventilation syndrome. Specific AEs associated with electrical current were spastic injury (e.g., fracture of the femur head and dislocation of the wrist joint), electrical injury, atrioventricular block, aggravated bulbar palsy, and “others.”
Conclusions:
Apart from general AEs, there are also types of specific AEs that could be caused by connecting an electrical current to the acupuncture needles. Although the incidence of the AEs is unknown, based merely on information acquired during this review, the specific risks associated with EA should be of concern for acupuncturists in clinical practice.
Introduction
Methods
Inclusion/Exclusion Criteria
Published surveys, case reports, and case series were included in the review if they reported factual data relating to the safety of EA. Review articles, translations, and clinical trials were excluded. AEs related to other types of acupuncture (e.g., auricular acupuncture, injection in acupoints, and laser acupuncture) were excluded from this review.
Literature Search
Six electronic literature databases were searched in December 2010, including the Chinese Biomedical Literature Database (CBM, 1980–2010), the Chinese Journal Full-Text Database (CNKI, 1979–2010), the Weipu Journal Database (VIP, 1989–2010), PubMed (1950–2010), EMBASE (1970–2010), and the Cochrane Library (Issue 2, 2010). The search terms included
Two reviewers (Zheng and Zhang) examined independently the titles and abstracts of all the articles found through the search to determine which articles to include, basing their judgments on the selection criteria outlined above. The full texts of potentially relevant articles were then retrieved for further assessment.
Data Extraction and Analysis
Information on authors, patients, acupuncturists, AEs, treatment, and prognoses was extracted and entered onto a preformulated form.
Important information was summarized in a table including details of each AE. Acupuncturists, manipulations, acupoints, and patients' conditions in all cases were sorted into different subgroups.
Results
Fifteen articles met the inclusion criteria (Fig. 1) All of these articles were case reports, covering a total of 44 cases of EA-related AEs published between 1979 and 2010. The ages of patients ranged from 17 to 65.
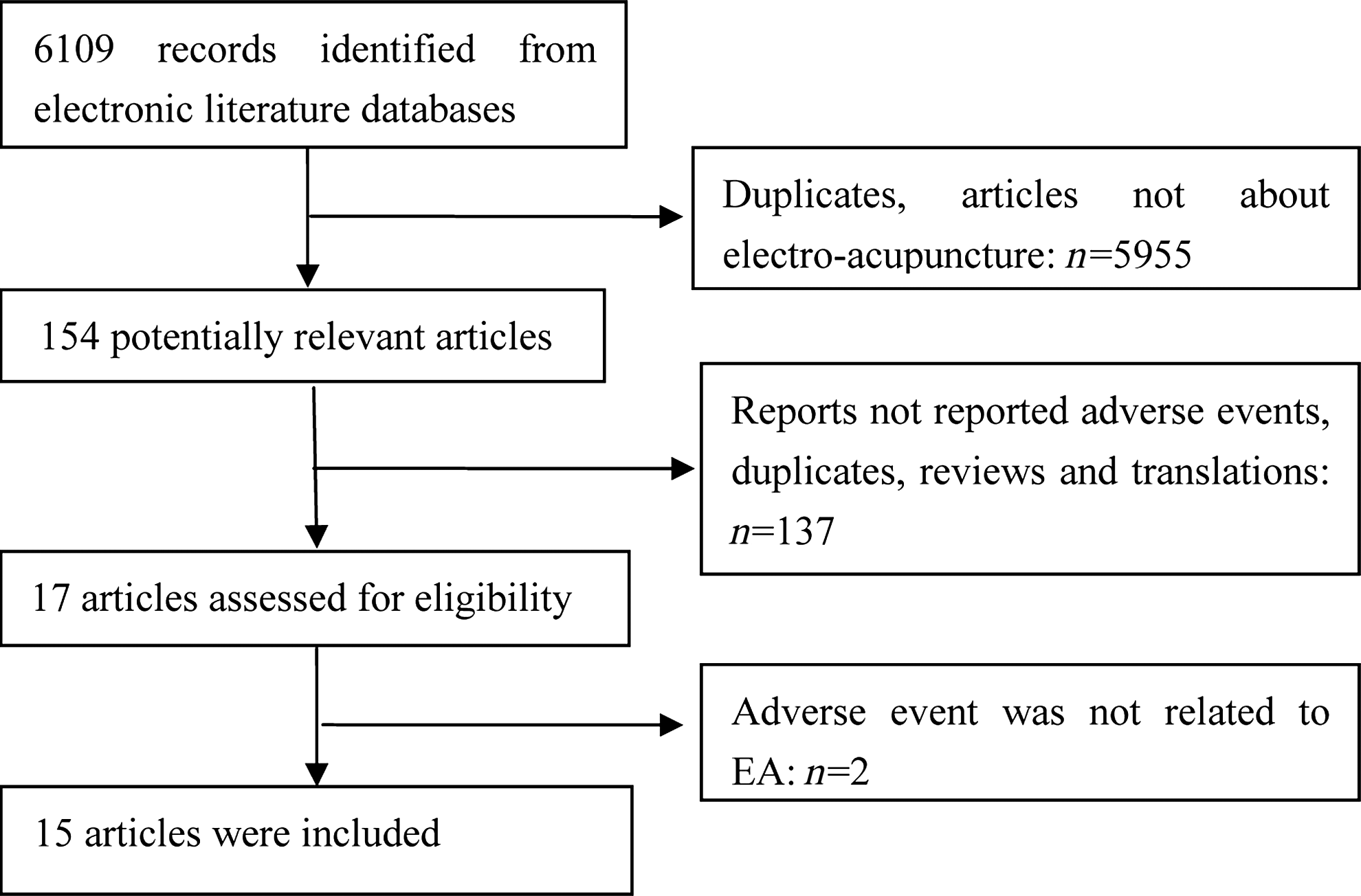
Literature selection of electro-acupuncture (EA)–related adverse events.
The reported AEs were classified into two categories: general AEs (n=7) and specific AEs (n=37). General AEs were events that were irrelevant to electrical stimulations, while specific AEs were considered as those that were most probably caused by the electrical stimulations accompanying the acupuncture.
General AEs
A total of 7 cases of general AEs were reported in 6 articles. These cases were classified into two subgroups according to the various patients' symptoms.
Traumatic events
Traumatic events were reported in 3 articles with 4 cases. Two patients died from spinal-cord injuries.3,4 The commonly used acupoints were Fengchi (GB 20), Yamen (GV 15), and Dazhui (GV 14) in the nape of the neck area. A 19-year-old girl with a history of schizophrenia had a heart injury after being needled at the Jiuwei (CV 15) point. In this case, the doctor inserted a 2-inch needle into the Jiuwei (CV 15) point vertically and turned the same needle 1′ toward her sternum. He also needled in the Quchi (LI 11) point and connected it with a device called a G6802 instrument. (This device may have been a kind of instrument used in China before the 1970s. The author of the article failed to provide more information about it). The needle at Jiuwei (CV 15) started vibrating vigorously immediately after the instrument was powered up. A few minutes later, the patient began to vomit suddenly, then stopped breathing, and, finally, her heartbeat ceased. Unfortunately, a pulmonary infection occurred during an attempt to rescue her with open thoracic heart massage, and this patient died 20 days later. 4 A hydropneumothorax-complicated infection occurred in a patient after EA at the bilateral supraclavicular fossa for neurosis. The patient recovered after 8 days of treatment. 5 The author of the article, however, did not mention which acupuncture points had been needled.
Needles were inserted too deeply in those acupoints in high-risk areas of the body, which could have led to these organic injuries. In addition, electricity pulses may have led to a gradual deepening of acupuncture needles and increased the risk of organ damage. These serious AEs occurred before the 1980s, when acupuncture practitioners might not have been well-trained, and lack of medical resources in rural hospitals might have also led to avoidable deaths.
Other general events
Two cases of fainting and a case of hyperventilation syndrome were reported after patients received EA treatment for the first time. A 42-year-old man experienced tardive fainting after EA in the Jiaji (Ex-B2) point and the Weizhong (BL 40) point in treatment for lumbar strain. 6 The other patient with diagnosed thyroid cancer had EA at the Yifeng (SJ 17) point for anesthesia. The patient became pale, felt dizzy, and lost consciousness for 2 minutes, but recovered after timely treatment. 7 Such AEs might be attributable to improper electrical stimulation of the carotid sinus. Hyperventilation syndrome was reported in a 35-year-old woman who had breathlessness and palpitation. After EA at Fengchi (GB 20) and Jiaji (Ex-B2), she experienced an exacerbation of these symptoms and recovered after timely treatment. 8
WHO, World Health Organization; AEs, adverse events.
Specific AEs
Specific AEs were reported in 9 articles and included 37 cases. These events were classified into five subgroups as discussed in the sections below.
Peripheral nerve irritation–related events
Fourteen cases of peripheral nerve–irritation related AEs were reported, including aggravated Bell's palsy (n=13) 9 and oculomotor paresis accompanied by neuroparalytic keratitis (n=1). 10
Thirteen patients in the early stage of Bell's palsy had aggravated symptoms after receiving EA. These events were mainly caused by incorrect operation of the EA device with a strong electric current. All patients recovered after ∼3 months of treatment, except in 1 case—a 65-year-old woman lost her eyesight forever.
Cardiac-conduction block
One article reported a total of 17 cases of atrioventricular block during EA treatment for psychosis at the Anmian points (between SJ 17 and GB 20) in the neck area. 11 Except for 1 patient, all recovered when the EA was discontinued. The cause of this type of AE might have been that the electrical current affected the function of the vagus nerves.
Electrical burn
One case of an electrical burn was reported in a patient who received EA on his leg. 12 He felt a burning sensation around the needle site after 10 minutes of EA, and his skin blistered 5 hours later. Three days later, the skin of the leg developed extensive necrosis and a concurrent infection. Detailed information on the treatment and prognosis for this patient was not provided in the article. Such an AE following EA might have been the result of long-time and/or strong electric current stimulation.
Spasm
Three articles reported 3 cases of spasm following EA, including a femoral neck fracture, 13 a subluxation of the wrist joint 14 and a nape of the neck muscle spasm. 15 The latter 2 patients recovered within 1 week after timely treatment, while the prognosis of the patient with the femoral neck fracture was not reported. Strong electrical stimulation combined with wrong operation of the EA devices accounted for these AEs.
Irritable gastric ulcer
Two cases of irritable gastric ulcer were reported in 2 articles. One was a 61-year-old man who received EA at Liangqiu (St 34), Xuehai (Sp 10), Xiyangguan (GB 33), Yanglingquan (GB 34), Fenglong (St 40), and Sanyinjiao (Sp 6) using a G6805 instrument for rheumatoid arthritis. 16 How the electrical circuit was created was not reported. The patient experienced a sudden stomach pain accompanied by vomiting of blood and unconsciousness when the acupuncturist turned up the electric current to the maximum tolerable level. He was diagnosed with stress ulcer associated with hemorrhagic shock. The reason for this AE was that the patient had a history of stomach bleeding, and long-term use of anti-inflammatory analgesic made him overreact to the strong electrical stimulation. After 2 months of treatment, the patient was discharged from the hospital.
Another patient received EA treatment at bilateral Zusanli (St 36) points, using a G6805 instrument for gastric ulcer for the first time. 17 Although the electric current strength was at a tolerable level, the patient felt unbearable pain under the xiphoid bone and had nausea accompanied with chest tightness 13 minutes later. This patient was diagnosed with gastric ulcer complicated by perforation. He recuperated after surgery and 10 days of treatment. However, the reason for this AE was not clear.
Discussion
A range of AEs associated with EA have been reported in the Chinese literature. Approximately 84% of these AEs (37/44) were related to an electrical that was added to acupuncture needles. EA used in high-risk acupoints and/or with a strong electric current may multiply the risk associated with EA.
Traumatic events following improper manipulation at high-risk acupoints caused serious AEs, including 3 deaths. All of the deaths occurred in patients with schizophrenia. These AEs serve as a reminder not to use EA in patients with psychiatric disorders. The depth of needle insertion was crucial in these fatal cases, while the electric current might have been irrelevant. For specific AEs, cardiac-conduction block, aggravated Bell's palsy, and spasm electrical burn were evidently related to the electric current added to the needles. Therefore, acupuncturists should pay more attention to the strength of the electric current and the position of acupoints used. However, there are no well-established criteria for selecting an appropriate current type and strength for EA. Further studies are needed. Currently, the present authors do not recommend use of EA at acupoints located in the head, neck, and the pericardial area of the body because electric current in these areas is apt to affect the function of the heart and the central nervous system, causing serious complications. It is strongly suggested that acupuncturists become very familiar with their patients' medical histories before initiating treatment. Patients with a history of stomach ulcer or stomach bleeding should be treated with caution.
This review had several limitations. Although the search strategy was comprehensive, the authors are not certain that all relevant articles were located. All of the AEs were reported in the Chinese literature. This may be a result of publication bias. EA costs too much more than traditional manual acupuncture to be popular for use in rural clinics in China, and this might have affected the number of AEs reported as a result of EA treatment. Furthermore, it was not possible to identify the incidence of AEs associated with EA from several case reports.
Conclusions
In addition to general AEs related to manual acupuncture, a range of specific AEs associated with EA were identified in this review. It was not possible to calculate the incidence rate of these AEs, but most AEs were attributed to improper operation. Therefore, EA should be used cautiously. EA is safe when performed by competent practitioners. Further studies are needed to justify whether EA is better than traditional manual acupuncture for specific conditions.
Footnotes
Acknowledgments
This review was supported by the New Century Excellent Talents in University (NCET-09-0900) program, which is supported by the Chinese Ministry of Education.
The authors thank Li Zhang, Ph.D. for her help with literature searching and Wei Mu, Ph.D. for revising the English language.
Disclosure Statement
No competing financial conflicts exist.