
Abstract
Abstract
Background:
Acupuncture has been demonstrated as an effective way to control nausea and vomiting induced by chemotherapy but has not been tested in conjunction with optimal use of antiemetic medication.
Objective:
The goal of this study was to explore the feasibility and safety of electroacupuncture (EA) for women with breast cancer, who were receiving chemotherapy.
Design:
The study was a randomized controlled pilot trial.
Setting:
This trial was conducted at a medical oncology clinic at the Royal Prince Alfred Hospital, in Sydney, New South Wales, Australia.
Patients:
Thirty-two women with breast cancer were recruited from a medical oncology clinic between March 2008 and July 2009.
Intervention:
The intervention tested was true EA versus sham EA.
Main Outcome Measures:
The study tested the effect of EA on women with breast cancer who were receiving chemotherapy, with respect to nausea, vomiting, and blood cell counts.
Results:
All but 2 participants completed EA treatment; these two dropouts were 1 from the true EA group and 1 from the sham EA group. No adverse effects of EA were reported. There was no significant difference in nausea and vomiting between the groups. However, there were significant differences in adjusted white blood-cell and neutrophil counts at week 6 in the true EA group, compared to the sham EA group.
Conclusions:
The findings of this trial suggest that EA during chemotherapy is a promising option for controlling side-effects of chemotherapy. An adequately powered, randomized, controlled trial to confirm the effect of EA is, therefore, warranted.
Introduction
Prevention and treatment of chemotherapy-induced nausea and vomiting has substantially improved with the advent of 5-HT3 receptor antagonists, dexamethasone, and the neurokinin-1 antagonist, aprepitant. 11 However, control of both acute and delayed nausea remains problematic. Approximately 50% of patients have reported experiencing nausea despite being given aprepitant, and there have been no significant reductions in rates of nausea. 12
Neutropenia is also a major concern in women receiving anthracycline-based adjuvant chemotherapy for breast cancer. The incidence of overall neutropenia is 82%, with rates of potentially life-threatening febrile neutropenia and neutropenic infections at 10.8% and 4.4% respectively. 13 Colony-stimulating factors (CSFs), such as growth CSF (GCSF), have been administered to women receiving chemotherapy for early stage breast cancer to maintain optimum dosages of anticancer drugs. However, these factors are expensive, and frequently reported side-effects include musculoskeletal pain and fever.14,15 Thus, considering that >50% of women with early stage breast cancer receive adjuvant chemotherapy, it is essential to minimize its side-effects to enable women to tolerate the treatment.
Within the last 12 years, concurrent use of complementary medical therapies, especially acupuncture, has gained increasing popularity in relieving some side-effects associated with anthracycline-based adjuvant chemotherapy.16–18 A meta-analysis of 1247 patients reported a 20% reduction in chemotherapy-induced acute emesis for manual acupuncture and electroacupuncture (EA), when used in conjunction with antiemetic drugs. 19 However, previous trials investigating the effects of manual acupuncture or EA used less-than-optimal antiemetic regimens, did not include assessment of delayed nausea and vomiting, and did not consistently utilize a sham comparison. 19 Therefore, while it is evident that acupuncture can prevent vomiting and nausea, it is not known if acupuncture provides any additional benefit in excess of current, optimal antiemetic regimens or placebo.
In addition, acupuncture treatment appears to have the potential to modulate the number and activity of neutrophils 20 and white-cell counts (WCCs).21–23 A meta-analysis on this topic suggests that acupuncture could increase WCCs by 1221 cell/mL, on average. 24 However, conclusions in this meta-analysis were limited by the poor methodological quality of the included studies, and little research has been undertaken to understand the mechanisms contributing to these results. 21
Thus, this pilot randomized controlled trial (RCT) was conducted to evaluate the effects of EA used in conjunction with anthracycline-based adjuvant chemotherapy among women with breast cancer. With the aim of providing data that would be needed for a larger RCT, the objectives of the pilot study were (1) to evaluate the feasibility and safety of a study evaluating the use of acupuncture in conjunction with chemotherapy and (2) to assess the efficacy of EA for relieving chemotherapy-induced vomiting, nausea and neutropenia.
Participants And Methods
Study Participants
Patients were recruited from a medical oncology clinic at a tertiary teaching hospital between March 2008 and July 2009. Inclusion criteria were: female patients ages ≥18 with early stage breast cancer; planned treatment including a combination of adriamycin (60 mg/m2) and cyclophosphamide (600 mg/m2) or epirubicin (100 mg/m2), cyclophosphamide (500 mg/m2), and 5-fluorouracil (500 mg/m2); Eastern Cooperative Oncology Group (ECOG) status of 0–2 (indicating capable of self-care activities despite effects of cancer and its treament); adequate baseline full blood count (hemoglobin, white cell, neutrophil, and platelet counts within the normal range) and other biochemistry results (serum creatinine, bilirubin, alkaline phosphatase, γ-glutamyl transferase and transaminases ≤1.5 times upper limit of normal); and ability to provide written informed consent. Patients were excluded if they had previous chemotherapy treatment; a cardiac pacemaker or defibrillator or any other implanted or topical electrical device; active infection; a coagulation disorder, including participants on warfarin or low–molecular-weight heparin; currently used antiemetics on a regular basis; had a needle phobia making it impossible to receive EA; were pregnant or breast feeding; and had any other serious medical or psychiatric conditions that compromised providing informed consent.
The study protocol was approved by the Human Research Ethics Committee of Royal Prince Alfred Hospital, Sydney, New South Wales, Australia.
Randomization Procedure
Patients were stratified into 2 groups depending on the type of chemotherapy received: (1) AC (adriamycin 60 mg/m2 and cyclophosphamide 600 mg/m2); or (2) FEC (epirubicin 100 mg/m2, cyclophosphamide 500 mg/m2 and 5-fluorouracil 500 mg/m2). The participants were then assigned randomly to receive either true or sham EA treatment according to a computer-generated randomization list. Serially numbered and sealed envelopes were used to indicate assignments, and patients were entered into a study log before the envelopes were opened. All envelopes were accounted for.
Conventional Treatments
Chemotherapy: Women received either AC or FEC every 3 weeks.
Antiemetics: All patients received the same antiemetic therapy. On day 1, the patients were given 5 mg of tropisetron and 125 mg of aprepitant orally, and 8 mg of dexamethasone intravenously, 1 hour before chemotherapy. Participants then received 5 mg of tropisetron, 80 mg of aprepitant, and 4 mg of dexamethasone on days 2 and 3 after chemotherapy. Additional antiemetic medication was allowed at the discretion of the oncologists.
EA Administrations
True EA: EA was scheduled at least 2 hours prior to chemotherapy. It was administered on days 1 and 2 of the first two cycles of chemotherapy. EA treatment consisted of bilateral perpendicular insertion of stainless steel acupuncture needles (Viva, made in China, gauge and size 0.20×25mm) at the PC 6, LI 4, and ST 36 acupuncture points. These points are designated for reducing emesis and stimulating immune function. 25
The PC 6 acupuncture point is located on anterior surface between tendons of palmaris longus and flexor carpi radialis, whereas the LI 4 is located on the dorsum of the hand radial to the midpoint of the second metacarpal bone and ST 36 on the tibialis anterior muscle. The needles were inserted at PC 6 on the left arm, at LI 4 on the right hand, and ST 36 on both legs at on day 1, and then the corresponding points in the alternate arm and hand on day 2.
The needles were inserted with bilateral rotation until the De Qi sensation was elicited. The needling technique included twirling, thrusting, lifting, and initial flicking. After De Qi was achieved, the needles were connected through a microalligator clip and an electrode to a battery-operated pulse generator connected to the negative pole and the positive pole. PC 6 and ST 36 were connected negative-to-positive and likewise for LI 4 and ST 36. Electrical frequency was then delivered at 2 Hz, for a 1.5-second duration pulse width output of 0.5–4.0, for 20 minutes (Electro-Acupuncture Units IC-4107, ITO Co. Ltd. Japan).
Needle sites were examined at the end of each treatment. Two acupuncturists (B.O. and B.K. [see Acknowledgments for B.K.]), with more than 6 years of training and 10 years of experience, gave the acupuncture treatment to the participants. Before the needles were inserted, the acupuncturists evaluated patients according to Traditional Chinese Medicine (TCM) diagnosis procedures. However, the acupuncturists administered the standard EA protocol only. The first treatment took an average of 60 minutes, including the time used to establish a TCM diagnosis. The follow-up visit procedure took an average of 40 minutes, including evaluation and treatment. EA treatment took approximately 20 minutes per session.
Sham EA: Patients in the sham EA group received a placebo acupuncture treatment. The procedure followed was identical to that used with the true EA treatment but used Streitberger's placebo needles (Asiamed, Pullach, Germany; 0.30×30 mm) 26 and a false electrode. The placebo needles had a similar appearance to the needles used in the true acupuncture group, but when pushed forward against the skin the needle slid into the handle to appear shortened and provided patients with a pricking penetration sensation.
Outcome Measures
Nausea and vomiting: Nausea and vomiting were assessed by the Multinational Association of Supportive Care in Cancer (MASCC) antiemetic tool (MASCC Antiemesis Tool; MAT). This is an 8-item scale, in which participants record both acute episodes (occurring within 24 hours of chemotherapy) and delayed episodes (occurring 2–4 days after chemotherapy) of vomiting, nausea, and other side-effects from each cycle. The MAT was validated with adults who had cancer and demonstrated high internal consistency (Cronbach's α=0.77) 27 and enough sensitivity to detect the different dimensions of chemotherapy-induced nausea and vomiting.
WCC and neutrophil count: All participants' WCC and neutrophil counts were measured in the Hematology Department of the Royal Prince Alfred Hospital. Baseline blood samples were collected 2 hours before each cycle of chemotherapy and nadir blood samples were collected 10–12 days after each cycle.
Assessment of masking: At the end of the 63-day study period, patients were asked whether they thought they had received true or sham EA treatment.
Statistical Analysis
A target sample size of at least 30 participants was chosen for convenience. Two patients dropped out from the study and were excluded from the data analysis. Proportions with complete control of vomiting/nausea in the sham and true EA groups were compared, using the Fisher-Boschloo test. 28 When patients had pegfilgrastrin (GCSF)–affected blood counts, a count of 0×109/L was imputed to assess how acupuncture affected blood counts in the (hypothetical) absence of GCSF (“adjusted” counts). The Mann-Whitney U-test was used to compare adjusted blood counts at different timepoints. Results were considered to reach statistical significance with a p-value of <0.05. The statistical software package Stata 11.1 was used for all analyses.
Results
Participant Recruitment and Follow-Up
Thirty-two consecutive eligible patients were recruited. Fifteen were assigned to receive true EA (n=15) and seventeen were assigned to receive sham EA (n=17). All but 2 patients (7%) completed their EA and the questionnaires. One patient dropped out of the true EA group after receiving only two EA sessions, because she was hospitalized for severe nausea after chemotherapy. The other patient dropped out of the sham EA group after she recognized that she was receiving sham EA. No participant experienced adverse effects from the EA, and all participants received their planned chemotherapy treatments.
Demographic Characteristics of Participants
Demographic characteristics of participants are shown in Table 1. The mean age of participants in this study was 52 (standard deviation=9) years. There were no significant differences between the true and sham EA groups in alcohol intake, smoking, travel sickness, morning sickness, ethnicity, education level, ECOG scale, CAM and acupuncture use, or chemotherapy treatment.
The n varies because of missing values.
†AC includes two drugs: doxorubicin and cyclophosphamide.
EA, electroacupuncture; SD, standard deviation; ECOG, Eastern Cooperative Oncology Group; CAM, complementary and alternative medicine; AC, anthracycline; FEC, combination of fluorouracil (5FU), epirubicin, and cyclophosphamide.
Assessment of Masking
Participants were not reliably successful in identifying whether they received true or sham EA (χ2=2.397, p=0.215).
Nausea and Vomiting
Overall, more patients who had complete control of vomiting (79% versus 69%) were in the EA group than in the sham group, whereas the opposite result was found for complete control of nausea (14% versus 25%; see Table 2). However, these differences were not statistically significant. There was also no statistically significant difference between the sham EA and true EA groups in both acute and delayed vomiting and nausea (Table 3). However, there was a trend for fewer patients to experience acute vomiting in cycles 1 and 2 when receiving true EA, compared sham EA, but results for delayed vomiting were not consistent. Similarly, it was observed that there were fewer episodes of nausea for patients in the true EA group in cycle 1, but not in cycles 2 and 3.
EA intervention was implemented at chemotherapy cycles 1 & 2.
†Acute means in the 24 hours after chemotherapy.
‡Delayed means the period from the day after chemotherapy to 14 days after chemotherapy.
EA, electroacupuncture.
EA intervention was implemented at chemotherapy cycles 1 & 2.
Acute means in the 24 hours after chemotherapy.
Delayed means the period from the day after chemotherapy to 14 days after chemotherapy.
Mean severity of nausea indicated by participants on an analogue scale (range 1–10).
Number of vomiting episodes reported by participants.
EA, electroacupuncture.
Myelosuppression
There were no significant differences in WCC and neutrophil count between the sham EA group and the true EA group at baseline, cycle 1, or cycle 2. However, the true EA group had a significantly higher adjusted WCC (median 6.05 versus 4.50×109/L, p=0.01) and neutrophil count (median 3.55 versus 1.90×109/L, p=0.01), compared to the sham EA group at week 6, prior to cycle 3 (Figs. 1 and 2).
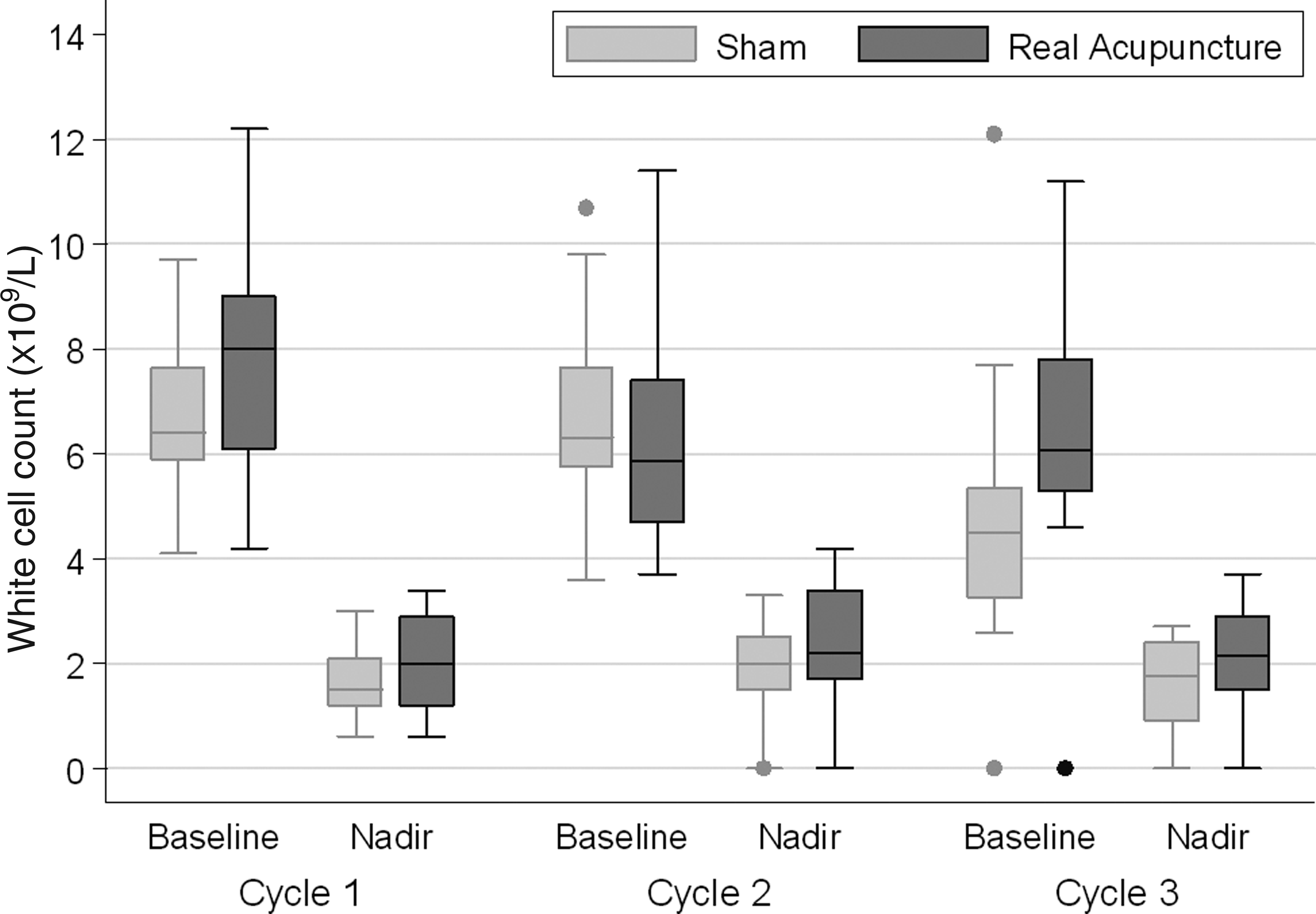
White cell count (× 109/L) of true EA group versus sham EA group. EA, electroacupuncture.
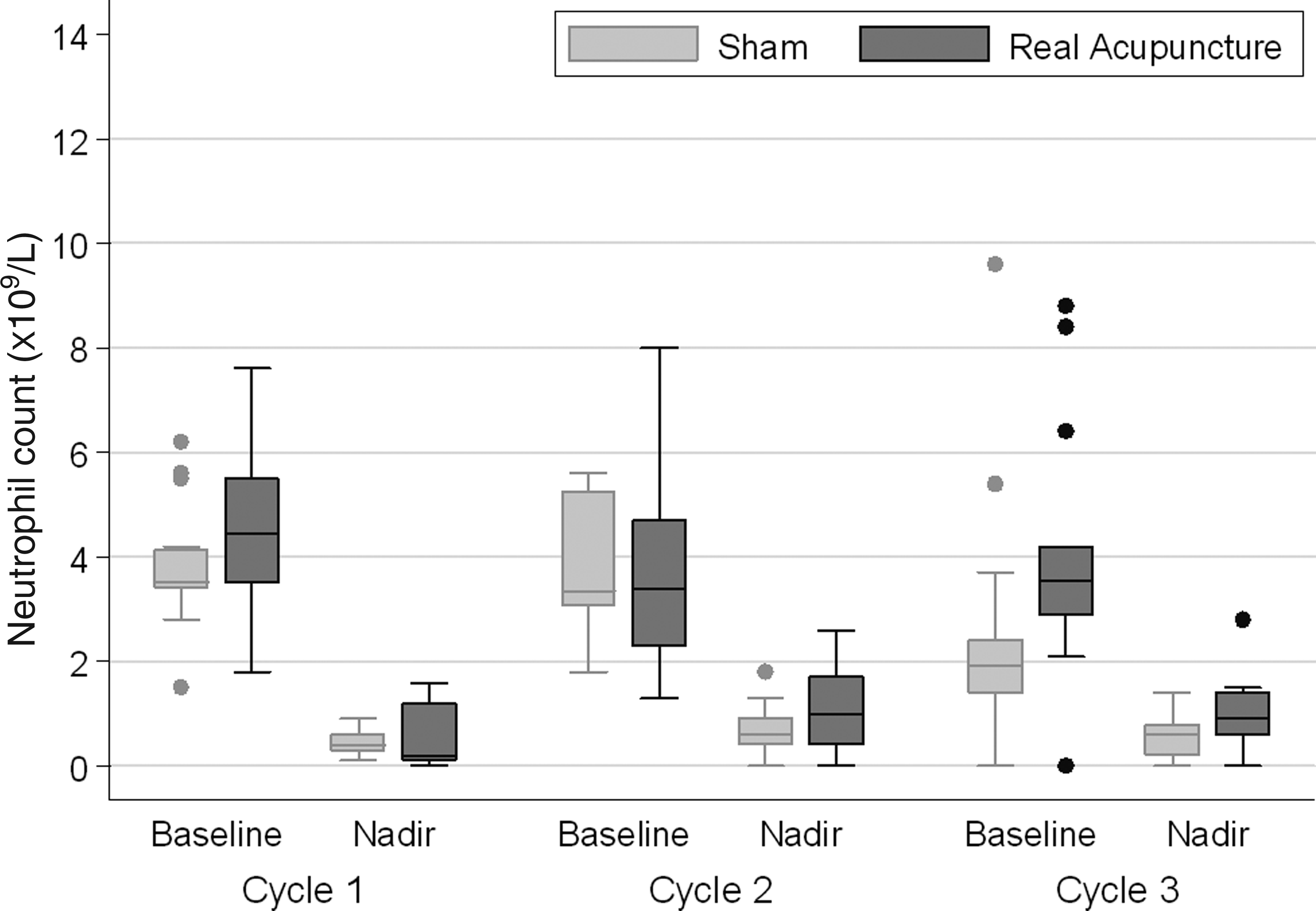
Neutrophil count (× 109/L) of true EA group versus sham EA group. EA, electroacupuncture.
Febrile Neutropenia and Growth Factors
After receiving the first chemotherapy treatment, 2 patients in the sham EA group experienced febrile neutropenia (FN), compared to 1 patient in the true EA group. Another patient in the sham EA group experienced FN after the third cycle of chemotherapy. Three patients in the sham EA group received GCSF and 1 in the intervention group received GCSF because of having FN or a low neutrophil count. There was no significant difference in GCSF administration between the groups in the two study arms (p=0.19).
Discussion
This study demonstrated that a sham-controlled study evaluating EA for chemotherapy-induced emesis and neutropenia is feasible and that further investigation is warranted. Although these results must be interpreted cautiously, because of the small sample size and other limitations discussed below, the results did indicate that, while true EA was not effective for decreasing acute and delayed nausea and vomiting, compared to sham EA, true EA did appear to provide patients with some protection against neutropenia.
The lack of effect on nausea and vomiting is contrary to the findings reported in previous studies, although trends in those studies indicated that fewer patients experienced acute vomiting and nausea in particular cycles when receiving true EA, compared to sham EA.19,29 A likely explanation for this discrepancy is that the current study was designed to evaluate the feasibility of EA with minimal acupuncture intervention, while patients were using optimal antiemetics. The acupuncture may have been more effective if patients had been allowed to have additional acupuncture points treated based on symptoms of individual patients rather than adhering to only points outlined in the protocol. A general treatment effect may also explain the discrepancy, as previous studies did not utilize sham EA groups consistently. Considering also that the current study lacked power, it is not surprising that a significant effect was not found. Therefore, investigation of the effect of EA on nausea and vomiting with a larger sample size is necessary before definitive conclusions cann be made. It would also be of interest to explore the effect of individualized acupuncture treatment on reducing side-effects experienced by women undergoing chemotherapy.
A significant finding of this study was that acupuncture appeared to minimize the decrease in WCC and neutrophil counts resulting from chemotherapy. This is consistent with findings from previous studies conducted with patients with ovarian cancer receiving chemotherapy 21 and with patients who did not have cancer but who had impaired immune function. 30 The lower rates of leukopenia and neutropenia seen in the true EA group suggest a potential myeloprotective effect of acupuncture. Interestingly, this effect was only evident at week 6, which probably represents a delayed physiological effect. Future studies are recommended to investigate the potential mechanisms behind the effectiveness of EA on WCC and neutrophil counts, taking into consideration dosage and length of EA treatment time. It is also worth considering that patients in the current study experienced no side-effects of the acupuncture treatment—a finding documented in previous studies.31,32 The current study's results indicate that EA may be a viable alternative to GCSF for improving neutrophil count and preventing FN among patients receiving chemotherapy.
Although the current study suggests that there is a possible benefit of EA in decreasing myelosuppression caused by chemotherapy, this study had limitations. As it was a pilot study, the analyses were underpowered and therefore reduced the ability to detect any differences between the true EA and sham EA groups. In addition, while the sham EA was designed to control for placebo effect, it did not control for the true effect of acupuncture. A recent study measuring brain activity during sham and true acupuncture indicated that the procedures activated very similar areas of the brain.33,34 Other researchers have also concluded that sham needles produce benefits beyond the placebo effect, 35 with some degree of efficacy, compared to true acupuncture. Therefore, to assess the true effect of acupuncture and minimize the acupuncture placebo effect, future studies are recommended to comply with the latest acupuncture research guidelines, which suggest an RCT with three arms: (1) true acupuncture; (2) sham acupuncture; and (2) and standard care or wait-list group.36,37
Despite these limitations, the current study also had a number of strengths. Perhaps the most prominent strength was the double-blinded RCT design with sham EA, as most previous studies did not include proper control groups. 19 In addition, measurement of both acute and delayed nausea and vomiting resulted in a longer follow-up, compared to most previous studies. 19 Furthermore, the confounding factor of anticipatory nausea and vomiting was reduced by including only women with early breast cancer undergoing their first chemotherapy treatments.
Conclusions
Overall, the current study showed that an evaluation of EA treatment given in conjunction with chemotherapy is safe and feasible in a hospital environment. The study also shows preliminary evidence that EA has the potential to reduce side-effects caused by chemotherapy and may, therefore, provide a much-needed treatment that can relieve these chemotherapy-related symptoms in many women with breast cancer. Thus, it is argued that a larger RCT with three arms (true EA, sham EA, and standard care or wait-list) is warranted to make stronger conclusions about the effect of EA on chemotherapy-induced nausea, vomiting, and mylosupresson.
Footnotes
Acknowledgments
This study was supported by the Area Health Services of New South Wales and Sydney Cancer Foundation. The authors would like to thank the medical oncologist team of Sydney Cancer Centre, Royal Prince Alfred Hospital, and to Benjamin Kim, LAc, assistant acupuncturist. Finally, thanks are extended to all participants of this study.
Disclosure Statement
No competing financial interests exist.