
Abstract
Abstract
Background:
Acupoint stimulation—including acupuncture, moxibustion, cupping, acupoint injection, and acupoint catgut embedding—has shown a beneficial effect for treating acne. However, comprehensive evaluation of current clinical evidence is lacking.
Objective:
The aim of this review was to assess the effectiveness and safety of all acupoint stimulation techniques used to treat acne vulgaris.
Design:
A systematic review was conducted. It included only randomized controlled trials on acupoint stimulation for acne. Six electronic databases were searched for English and Chinese language studies. All searches ended in May 2012. Studies were selected for eligibility and assessed for quality. RevMan 5.1 software was used for data analysis with an effect estimate presented as risk ratios (RR) or mean difference (MD) with a 95% confidence interval (CI).
Patients:
Studies with subjects who were diagnosed with acne vulgaris, or papulopustular, inflammatory, adolescent, or polymorphic acne—regardless of gender, age, and ethnicity—were included.
Intervention:
Interventions included any acupoint stimulation technique—such as acupuncture, moxibustion, cupping, acupoint injection, and acupoint catgut embedding—compared with no treatment, placebo, or conventional pharmaceutical medication.
Main Outcome Measure:
Reduction of signs and symptoms and presence of adverse effects were examined.
Results:
Forty-three trials involving 3453 patients with acne were included. The methodological quality of trials was generally poor in terms of randomization, blinding, and intention-to-treat analysis. Meta-analyses showed significant differences in increasing the number of cured patients between acupuncture plus herbal medicine and herbal medicine alone (RR: 1.60; 95% CI: 1.19–2.14; P=0.002), and between acupuncture plus herbal facial mask and herbal facial mask alone (RR: 2.14; 95% CI: 1.29–3.55; P=0.003). Cupping therapy was significantly better than pharmaceutical medications for increasing the number of cured patients (RR: 2.11; 95% CI: 1.45–3.07; P<0.0001). Serious adverse events were not reported in all included trials.
Conclusions:
Acupoint stimulation therapies combined with other treatments appears to be effective for acne. However, further large, rigorously designed trials are needed to confirm these findings.
Introduction
Acne treatment is aimed at decreasing inflammation of the lesions and accompanying discomfort with the ultimate goals of improving appearance and preventing or minimizing scarring and emotional distress. 3 Effective prescription medications are available, although side-effects—such as local irritation, teratogenicity, dry skin, hyperlipidemia, and increased risk of depression—are reported.4,5 Over-the-counter preparations and herbal remedies, as well as skin- hygiene routines and dietary modifications may be recommended by dermatologists or, more often, are self-prescribed. 4
In China, in addition to prescription medications, traditional Chinese therapies are used to treat acne. One such therapy is acupoint stimulation. Several methods can be applied: acupuncture with needles; moxibustion, which involves the controlled burning of material, typically mugwort (Artemisia vulgaris) herb, at certain points or areas of the body surface; cupping therapy, which involves applying suction by placing a vacuumized, usually by fire, cup or jar on acupoints or affected body surfaces to induce local hyperemia or hemostasis; acupoint injection, which involves injecting medication into an acupuncture point; and acupoint embedding, which involves embedding in the skin over the acupoint a small needle(s), or medicated catgut.
Acupoint-stimulation methods are based on the Traditional Chinese Medicine (TCM) view that acne is caused by any or a combination of several pathogenic factors. These include intense Lung Heat or Stomach Heat, Damp–Heat with Blood Stasis, and Qi (vital energy) Stagnation. As the condition becomes protracted, pathogenic Heat rises and accumulates in the skin and tissues, which brings on the lesions. 6
Potential mechanisms of acupoint stimulation for acne are to relieve Heat toxicity, eliminate Dampness, regulate the Qi and Blood, and enhance immunologic function. 6 Some studies also mention that acupuncture can stimulate and balance androgen levels to inhibit excess secretion of the sebaceous gland. 7
Articles with clinical observations have reported the efficacy of acupoint-stimulation therapies for acne. A systematic review 7 assessing seventeen TCM randomized controlled trials (RCTs) suggests that acupuncture and moxibustion are better than conventional pharmaceutical medication for reducing symptoms of acne. Another systematic review 8 involving twenty-three trials of topical and oral complementary and alternative medicines (CAMs) concluded that, poor methodological quality aside, the evidence suggests that many of these therapies are biologically plausible. However, there has been no systematic review that evaluated the clinical evidence of all types of acupoint-stimulation therapies. This systematic review was performed to assess the effectiveness and safety of all acupoint-stimulation techniques used to treat acne vulgaris.
Methods
Inclusion Criteria
Parallel-group RCTs were included in any data analysis with interventions for the treatment of acne vulgaris using any acupoint stimulation technique—such as acupuncture, moxibustion, cupping, acupoint injection, and acupoint catgut embedding—compared with no treatment, placebo, or conventional pharmaceutical medication. Comparisons also included a combination of acupoint-stimulation techniques, plus other therapies, versus the same other therapies alone. Participants who were diagnosed with acne vulgaris, or papulopustular, inflammatory, adolescent, or polymorphic acne—regardless of gender, age, and ethnicity—were included. Primary outcome measures were reduction of signs and symptoms and presence of adverse effects. Secondary outcome measures included post-treatment evaluation, participants' self-assessment of change in lesions after treatment, psychosocial outcomes, and quality of life (QoL) measurements.
Identification and Selection of Studies
Searches were conducted in the China Network Knowledge Infrastructure (CNKI, 1979–2012), Chinese Scientific Journals Database (VIP, 1989–2012), Wan Fang Database (1985–2012), Chinese Biomedicine (CBM, 1978–2012), Cochrane Central Register of Controlled Trials (CENTRAL, 1999–2012), and PubMed (1966–2012). All searches ended in May 2012. Search terms included
Data Extraction and Quality Assessment
Three authors (H.-j.C., G.-y.Y., and Y.-y.W.) independently extracted population and intervention characteristics using self-designed data extraction templates. Disagreements were resolved by discussion with another author (J.-p.L).
Risk of bias for each study was conducted in accord with the Cochrane Handbook for Systematic Reviews of Intervention. 9 Six criteria were applied, as follows: (1) selection bias (random-sequence generation and allocation concealment); (2) performance bias (blinding of participants and personnel); (3) detection bias (blinding of outcome assessment); (4) attrition bias (incomplete outcome data); (5) reporting bias (selective reporting); and (6) other bias. There were three potential bias judgments: (1) low risk; (2) high risk; and (3) unclear risk. A study was rated unclear risk when insufficient details were reported regarding what happened in the study. A judgment of unclear risk was also made when what happened in the study was known but the risk of bias was unknown or when an item was not relevant to the study, particularly for assessing blinding and incomplete outcome data or when the outcome assessed by the item had not been measured in the study.
Data Analysis
Dichotomous data were expressed as risk ratios (RR) with a 95% confidence interval (CI). Continuous data were expressed as mean differences (MDs) with 95% CIs. Statistical heterogeneity was tested by the I2 test. RevMan 5.1 software (Cochrane Collaboration) was used for data analyses. Meta-analysis was used if the trials had acceptable homogeneity (I2<85%) of study design, participants, interventions, controls, and outcome measures. Meta-analyses were performed using fixed-effect 9 models (I2<25%) for homogeneous studies and using random-effects methods prior to fixed-effect models when there was substantial heterogeneity (25%<I2<85%).
Results
Description of Studies
After primary searches of six databases, 535 citations were identified. We excluded 484 studies because they did not meet inclusion criteria. Full-text articles for 51 studies were retrieved. Finally, 43 trials10–52 were included in this review (Fig. 1). Characteristics of included trials are listed in Table 1. Among the included trials, fourteen studies11–15,19,21,26,31,35,42,43,45,46 were unpublished master's theses.

Search strategy flow chart.
Gender numbers not reported.
M, male; F, female; y, year(s); m, month(s); w, week(s); d, day(s); min, minutes; I, intervention group; C, control group; acu., acupuncture; NR, not reported; EA, electroacupuncture; QoL or QOL, quality of life; GAGS, Global Acne Grading System; TDP, a specific electromagnetic spectrum; WHO, World Health Organization; IgG, immunoglobulin G.
The forty-three trials involved a total of 3453 patients, with an average of 40 participants in each group. Age ranged between 13 and 43, and duration of disease varied from 1 week to 17 years. Ten trials 22,23,25,27,29,38,39,47,48,50 did not report diagnostic criteria, two trials10,30 used international diagnostic criteria, and thirty-three trials reported using one of four TCM diagnostic criteria.53–56 Of the thirty-three trials, six trials 24,36,40,41,43,52 did not report sources for diagnostic criteria, and eight trials11,15,17,20,31,34,37,51 used self-established diagnostic criteria for acne.
Interventions included acupuncture (electroacupuncture, auricular acupuncture, and ear point pressure), cupping therapy, acupoint injection, acupoint catgut embedding, moxibustion, and combination of acupoint-stimulation therapies and herbal medicine. Controls included pharmaceutical medications and herbal medicine alone. Courses of treatment ranged from 1 to 12 weeks.
Degree of reduction in clinical symptoms (known as the cure rate) as the major outcome measurement was reported in all forty-three included trials. Responses to interventions were classified as cure, markedly effective, effective, and ineffective. 53 Cure was defined as lesions totally faded (or>95% faded) and only mild pigmentation and scars remaining. Markedly effective was defined as lesions faded>60% and severity of lesions was alleviated. Effective was defined as lesions faded 20%–59% and severity of lesions was reduced. Ineffective was defined as lesions faded<20% or worsening of lesions. Four trials13,19,43,45 counted the number of skin lesions, three trials14,42,45 reported QoL scores, two trials42,43 reported recurrence rates, and three trials14,42,43 listed laboratory test results.
Methodological Quality
According to the current authors' predefined quality-assessment criteria, all forty-three trials were evaluated as having a high risk of bias (Fig. 2). Study sample size varied from 20 to 112 participants, with an average of 40 patients per group. None of the trials reported sample-size calculation methodology. Fifteen trials11,12,14,15,19,21,26,30,32,35,42,44–46,48 described randomization procedures, using random number tables or computer generation of random numbers, but only 1 trial 14 reported adequate allocation concealment. The majority of trials compared acupoint stimulation therapies and pharmaceutical medication; thus, blinding could not be applied for patients and researchers. Six trials13,25,26,32,45,46 reported the number of dropouts, but none used intention-to-treat (ITT) analysis. None of the trials mentioned sources of financial support.
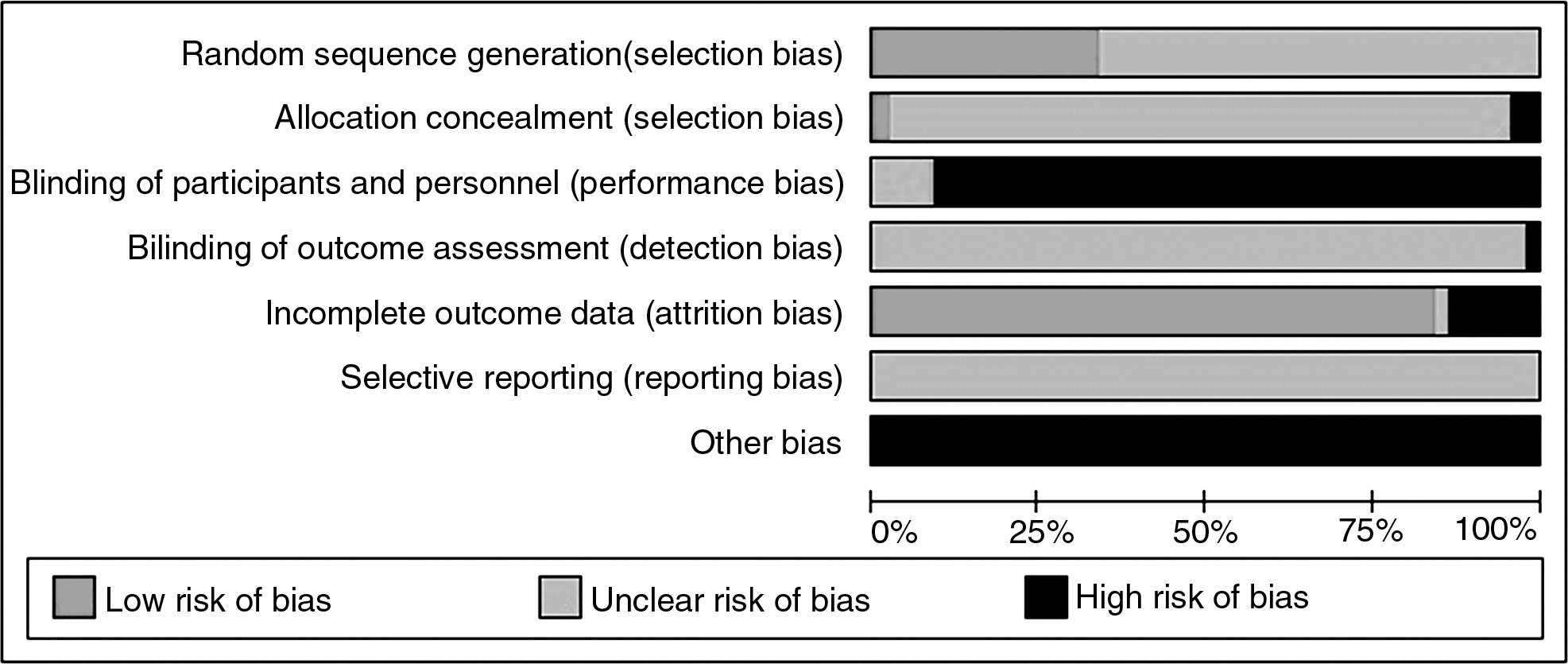
Risk of bias graph shows the review authors' judgments about each risk of bias item, presented as percentages across all included studies.
Effect Estimates
Because of variations in study quality, participant characteristics, intervention types, controls, and outcome measures, results of most trials could not be synthesized by quantitative methods. Therefore, qualitative methods were used (Table 2).
CI, confidence interval; RR, risk ratio.
Therapeutic effect of acupuncture
Therapeutic effect of acupuncture for acne was evaluated in 22 studies. Five studies13–16,32 compared acupuncture with pharmaceutical medications. Nine trials12,19,24,25,27,28,44–46 compared acupuncture plus herbal medicine with herbal medicine alone. Two trials21,33 compared acupuncture plus acupoint injection with acupoint injection alone. Two trials23,41 compared acupuncture plus a herbal facial mask with a facial mask alone. One trial 18 compared acupuncture plus cupping therapy with cupping therapy alone. One trial 35 compared acupuncture plus guasha (scraping) with guasha alone. One trial 26 compared acupuncture plus herbal medicine and acupoint injection with herbal medicine and acupoint injection alone.
Nineteen trials12–16,18,19,21,23–25,27,28,32,33,41,44–46 were included in four meta-analyses. There were a significant difference in the number of cured patients between acupuncture plus herbal medicine and herbal medicine alone (RR: 1.60; 95% CI: 1.19–2.14; P=0.002; random model; I2=46%; 9 trials), and between acupuncture plus herbal facial mask and herbal facial mask alone (RR: 2.14; 95% CI: 1.29–3.55; P=0.003; fixed model; I2=0%; 2 trials). No difference was seen in the comparison between acupuncture and pharmaceutical medications (RR: 1.49; 95% CI: 0.82–2.73; P=0.19; random model; I2=54%; 5 trials), and in the comparison between acupuncture plus acupoint injection and acupoint injection alone (RR: 2.00; 95% CI: 0.64–6.29, P=0.24; fixed model; I2=0%; 2 trials).
Three trials13,19,45 reported changes in skin-lesion count. One study 13 that used a skin-lesion scoring system, 53 showed that acupuncture was superior to pharmaceutical medication for reducing the skin-lesion area (MD: −26.95; 95% CI: −31.84 to −22.06; P<0.00001; 1 trial). The remaining two trials compared acupuncture plus herbal medicine with herbal medicine alone. One of the trials 45 found that a combination of acupuncture and herbal medicine was better than herbal medicine alone for reducing skin lesions (MD: −13.88; 95% CI: −19.17 to −8.59; P<0.00001, 1 trial), while the other trial 19 showed no difference between the comparison treatments (MD: −0.97; 95% CI: −3.06 to 1.12; P=0.36; 1 trial).
QoL (Acne-QoL) 57 was assessed in one trial, 14 finding that, compared with pharmaceutical medication, acupuncture appeared to significantly improve self-perception (MD: 3.40; 95% CI: 2.16–4.64; P<0.00001; 1 trial), social function (MD: 2.30; 95% CI: 1.23–3.37; P<0.0001; 1 trial), and emotional function (MD 2.30; 95% CI: 0.74–3.86; P=0.004; 1 trial).
Therapeutic effect of cupping therapy
Ten trials evaluated the effectiveness of cupping therapy for acne. Of the ten trials, four34,38,40,50 compared cupping therapy with pharmaceutical medications, three trials11,20,31 compared cupping therapy plus herbal medicine with herbal medicine alone, two trials30,37 compared cupping plus acupuncture with acupuncture alone, and one trial 17 compared cupping plus a herbal facial mask with herbal facial mask alone.
Meta-analysis showed that cupping therapy was significantly better than pharmaceutical medications, such as tanshinone, tetracycline, and ketokonazole (RR: 2.11; 95% CI: 1.45–3.07; P<0.0001; fixed model; I2=6%, 4 trials). Furthermore, cupping therapy combined with herbal medicine (RR: 1.91; 95% CI: 1.32–2.74; P=0.0005; fixed model; I2=0%; 3 trials) or acupuncture (RR: 1.79; 95% CI: 1.12–2.86; P=0.01; fixed model; I2=6%; 2 trials) was superior to herbal medicine or acupuncture alone. However, no difference was found between cupping plus a facial mask and a facial mask alone (RR: 1.58; 95% CI: 0.72–3.45; P=0.25; 1 trial). As each comparison had fewer than five trials, it was not meaningful to conduct a funnel-plot analysis.
Therapeutic effect of acupoint injection
Seven trials evaluated the effect of acupoint injection for acne. Of the seven trials, three22,39,48 compared acupoint injection with pharmaceutical medication, and four trials compared acupoint injection plus other treatment with other treatment alone (pharmaceutical medication,29,47 acupuncture, 42 and herbal medicine 49 ).
Meta-analysis showed that acupoint injection used alone (RR: 1.51; 95% CI: 1.13–2.03; P=0.006; fixed model; I2=0%; 3 trials) and combined with pharmaceutical medication (RR: 1.49; 95% CI: 1.12–1.99; P=0.007; fixed model, I2=0%; 2 trials) were significantly better than medication alone. However, no difference was found between acupoint injection combined with herbal medicine (RR: 1.08; 95% CI: 0.83–1.41; P=0.55; 1 trial) or acupuncture (RR: 1.45; 95% CI: 0.46–4.59; P=0.53; 1 trial) compared with herbal medicine or acupuncture alone. As each comparison had fewer than five trials, it was not meaningful to conduct a funnel-plot analysis.
One trial 42 reported QoL scores and recurrence rate. Results showed no difference between acupoint injection plus acupuncture and acupuncture alone in improving QoL (MD: −1.76; 95% CI: −3.80 to 0.28; P=0.09; 1 trial) and in reducing recurrence rate (RR: 0.22; 95% CI: 0.03–1.60; P=0.13; 1 trial).
Therapeutic effect of acupoint catgut embedding
Three trials36,43,52 evaluated the therapeutic effect of acupoint catgut embedding for acne. One study 52 showed acupoint catgut embedding was superior to pharmaceutical medication in increasing the number of cured patients (RR: 1.57; 95% CI: 1.15–2.15; P=0.004; 1 trial) and in reducing recurrence rate (RR: 0.22; 95% CI: 0.08–0.62; P=0.004; 1 trial). One trial 36 showed acupoint catgut embedding combined with herbal medicine was superior to herbal medicine alone in increasing the number of cured patients (RR: 1.85; 95% CI: 1.24–2.77; P=0.003; 1 trial). One study 43 showed no difference between acupoint catgut embedding plus pharmaceutical medication and pharmaceutical medication alone in increasing the number of cured patients (RR: 1.40; 95% CI: 0.50–3.92; P=0.52; 1 trial), reducing skin-lesion area (MD: 2.67; 95% CI: −0.07 to 5.41; P=0.06; 1 trial), and reducing recurrence rate (RR: 0.48; 95% CI: 0.12–1.88; P=0.29; 1 trial).
Therapeutic effect of moxibustion
Meta-analysis of two trials10,51 showed that a combination of moxibustion and acupuncture was better than acupuncture alone for increasing the number of cured patients (RR: 1.47; 95% CI: 1.05–2.07; P=0.03; fixed model; I2=0%; 2 trials).
Adverse events
Twenty-nine trials did not mention adverse events. Of the fourteen trials10,11,13,19,27,30,31,36,42,43,45,47,50,52 that did report adverse events, seven trials11,27,30,31,42,45,50 found no adverse events in both intervention and control groups. The remaining seven trials reported mild adverse events in the intervention and control groups (Table 1), such as thirst, dizziness, redness and swelling of the treated site, and pain or itching in the acupoint area. Serious adverse events were not reported.
Funnel-plot analysis
Funnel-plot analysis of eight trials showed significant asymmetry (Fig. 3).
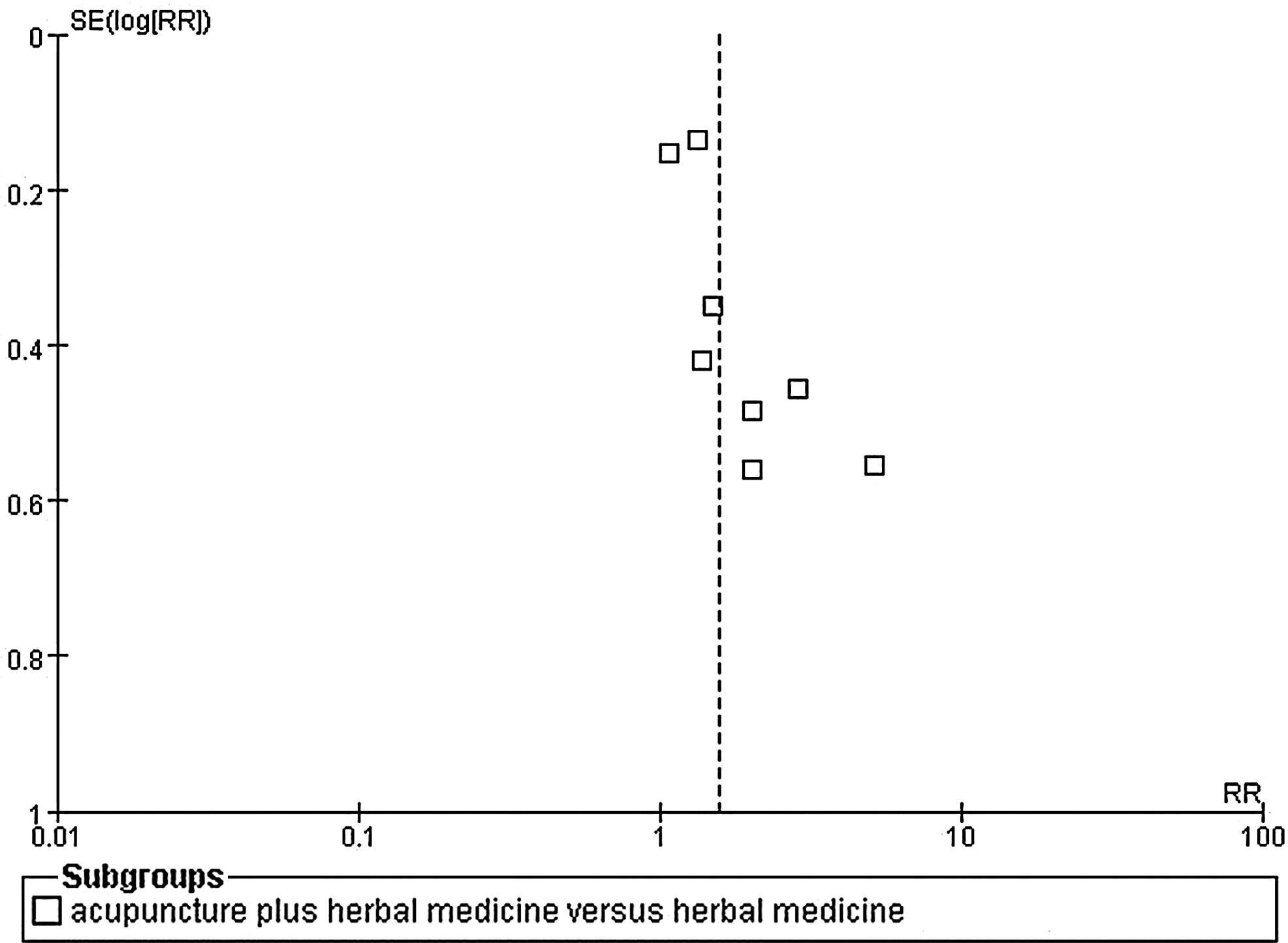
Funnel plot of eight trials for the outcome of number of patients cured of acne. SE, standard error; RR, relative risk.
Discussion
This study's data demonstrated that, in the studies that were evaluated, acupuncture and cupping therapy used alone or in combination with pharmaceutical medication appeared to be more effective than pharmaceutical medication alone in increasing the number of cured patients with acne. However, further studies are needed to confirm this finding. The therapeutic effects of acupoint injection, acupoint catgut embedding, and moxibustion were unclear because there was insufficient evidence from the available studies.
Results of nine meta-analyses found that acupoint-stimulation therapies combined with other treatments were significantly more efficacious than other treatments applied alone. Cupping therapy and acupoint injection appeared to be superior to pharmaceutical medication, whereas no difference in efficacy was seen between acupuncture and pharmaceutical medication. Although across studies, the use of pharmaceutical medication was not guideline-based or dosage-consistent (Table 1), acupoint-stimulation therapies, including acupuncture, cupping, and acupoint injection may have an equivalent therapeutic effect as medication (antibiotics, antiprotozoal, licorsinc, isotretinoin) for acne. Given that no severe adverse events were reported in the included studies, the current authors believe that it would be worthwhile to conduct further, rigorously designed trials on acupoint-stimulation therapies for the treatment of acne.
This current review revealed that there remains a lack of well-designed studies on the treatment of acne using acupoint-stimulation therapies. Methodological quality of the studies included in this review was generally poor, indicating a high risk of bias. Inadequate application of randomization and absence of blinding were evident in the majority of trials, causing potential performance bias and detection bias, because patients and researchers were aware of the therapeutic interventions. Applying proper blinding methodology remains a challenge for studies on manual-healing therapies. Even so, at the very least, blinding of outcome assessors is highly recommended in such studies. ITT analysis was not applied in most of the trials and the funnel-plot indicated that these data may have publication bias. Intervention response using the ambiguous and subjective terminology of cure, markedly effective, effective, and ineffective was difficult to interpret and validate across studies. Consequently, any positive finding needs to be interpreted cautiously. Researchers of future studies should consider applying more robustly defined intervention response measurements, such as one of the existing acne grading scales. 58 None of the trials reported sample-size calculation. The current authors strongly recommend that future RCTs include sample-size estimates to ensure adequate statistical power. Furthermore, sample-size calculation and analysis of outcomes should be based on the principle of ITT.
Twelve trials13,14,16,19,21,23,24,30,44–46,50 used skin-lesion (“ouch” point) areas as the main targets for stimulation, while other studies10–12,15,17,18,20,22,25–29,31–43,47–49,51,52 established acupoint prescriptions that were followed throughout the duration of the trials. The limited number of trials precluded the current authors from ascertaining the differences in therapeutic effects among these three types of acupoint-selection methods.
The potential asymmetry of the funnel-plot test (Fig. 3) of eight trials that examined acupuncture plus herbal medicine, compared with herbal medicine alone may have been caused by small study effects or even heterogeneity in intervention effects. Furthermore, as ongoing trials were not included, and, as all trials were conducted in China, there is a high potential for publication bias in the current review.
In summary, most of the existing trials were of small size and had a high risk of bias. Further high-quality, large-scale studies are needed to confirm the effectiveness of acupoint-stimulation therapy for treating acne. Randomization methods need to be described clearly and reported fully. Blinding of outcome assessors should be attempted as feasibly as possible to minimize performance and assessment biases. Outcome (response) measures utilizing acne-grading scales should be applied and should include contiguous data, such as skin-lesion scores from baseline to study completion. Analysis of outcomes based on the ITT principle is vital as is the application of sample-size calculation. Reporting of trials should adhere to the Consolidated Standards Of Reporting Trials (CONSORT) 59 to ensure clarity and completeness of reporting.
Conclusions
Acupoint-stimulation therapy—especially when it is combined with other treatments—appears to be effective for treating acne. However, further large, rigorously designed trials are needed to confirm these findings.
Footnotes
Acknowledgments
H.-j. Cao and J.-p. Liu were supported by the Research Capacity Establishment Grant (number 101207007) of Beijing University of Chinese Medicine. This work was also supported by the grant numbers 2009ZX09502-028 and 2011ZX09302-006-01-03(5). The authors thank Nissi S. Wang MS, for content editing of this manuscript.
Disclosure Statement
No competing financial interests exist.