
Abstract
Abstract
Background:
Randomized controlled trials show therapeutic effectiveness often for both verum and sham acupuncture. Yet, limited research suggests that verum acupoints are electrophysiologically distinguishable from sham points.
Objective:
This work investigates changes in the bioelectric potential at acupoints and control sites at site of stimulation and distal to that site.
Design, Setting, and Subjects:
At the New England School of Acupuncture, needles were inserted at four sites on 14 healthy volunteers, two proximal sites (PC 4 and PC 4cont [control]), and two distal sites (PC 6 and PC 6cont). Bioelectric potentials from all four sites were measured.
Main Outcome Measures:
Bioelectric potential (peak voltage in mV) during the three stimulations was averaged to provide a single measurement.
Intervention:
PC4 and PC4cont were stimulated three times in random order with a 3-minute interval between stimulations; each stimulus lasted 10 seconds.
Results:
A translation phenomenon (an induced polarization) was seen at the distal site when the proximal site was stimulated. At PC 6 with PC 4 stimulated there was a larger amplitude (p<0.05), compared to the control response.
Conclusions:
These findings suggest electrophysiological uniqueness in the form of a greater bioelectric potential amplitude when a proximal acupoint is stimulated and the response is measured at a distal acupoint along the associated meridian.
Introduction
When measuring electrical impedance, a large exogenous current is applied to the tissue at one site and current and voltage measurements are obtained at another site. Subtleties of bioelectric change, however, are difficult to measure with this method because of the large current source applied. 2 Endogenous bioelectric potentials, however, reflect small changes in amplitude without the confounding influence of an external electrical current.3–5
Randomized clinical trials (RCTs) of acupuncture often include stimulating verum acupoints and nearby so-called “sham” acupoints. Clinical effectiveness has been reported with both verum and sham stimulation. The verum acupuncture is often only marginally better than the sham acupuncture.6–8 This leads researchers to question if sham acupuncture is indeed a physiologically inactive control placebo. 9 An electrophysiological correlate of these clinical findings would be eliciting from the sham acupuncture at a nonacupoint a bioelectrical response that is nearly as strong as the bioelectrical response from stimulating a verum acupoint.
The aim of this study was to document changes in the bioelectric potential that occur in response to needling Pericardium 4 (PC 4) and PC 4cont (control) at four sites on the forearm PC 4, a nearby nonacupuncture point (PC4cont) and two distal points (PC 6 and a nearby nonacupoint (PC 6cont) It was hypothesized that a greater bioelectric potential amplitude was induced distal to the point of stimulation only when the needling site was on the acupuncture point and the distal measured site was on the meridian.
Methods
Participants
Fourteen participants were recruited from the New England School of Acupuncture (NESA) student body and faculty to take part in the study; their ages ranged from 24 to 52. Participants stated that they had no chronic or acute illnesses; and all participants provided written consent to participate in the study. Five different acupuncturists, whose role was to perform acupuncture needle stimulation, were recruited from the NESA faculty and alumni. All were licensed acupuncturists. Numerous acupuncturists participated to ensure a range of acupuncture styles and limit any confounding effects from any one person's acupuncture method. Previous to study implementation, protocol and informed consent forms were approved by the New England Institutional Review Board.
Equipment
The bioelectric potential was recorded on a ML138 Bio Amp (ADInstruments, Colorado Springs, CO). The Bio Amp consists of eight electrically isolated differential input instrumentation amplifiers. Each amplifier has a differential input impedance of 200MΩ ensuring a miniscule current into the equipment from the electrode on the acupuncture needle (<0.5 nA). The BioAmp was connected to a ML880 PowerLab 16/30 data-acquisition unit which connected to a personal computer (PC) run on Labchart software. During testing, realtime data was seen on the PC by the acupuncturist, participant, and operator, and the data were concurrently saved on the PC's hard drive. Data analysis, signal processing, and statistical analysis were performed in Matlab and Excel.
The current authors' preliminary work suggested that they should should investigate slow-moving signals (<1 Hz). A fast Fourier transform (FFT) was calculated to investigate the frequency domain of the signals; because there was interest in slow-moving signals, a low sampling rate was used to have an accurate FFT. Because of the Nyquist frequency phenomenon it was also of interest to choose a low sampling rate to use digitizing and subsequent low-pass filtering to inherently filter out any 60-Hz background noise. The sampling rate was therefore set to 10 Hz. Because the interest was in very slow–moving signals, it was considered ideal to ascertain the DC response as well. However, because the ML138 Bio Amp has an adjustable input high-pass filter (that was set at its minimum of 0.02 Hz), DC measurements were attenuated.
One-inch, stainless steel acupuncture needles were used as electrodes at the interface from the tissue to the crocodile clips on the cables leading to the BioAmp (Fig. 1). Surface electrodes (Ag/AgCl 10-mm contact diameter electrodes) were used for the reference and the ground connection.
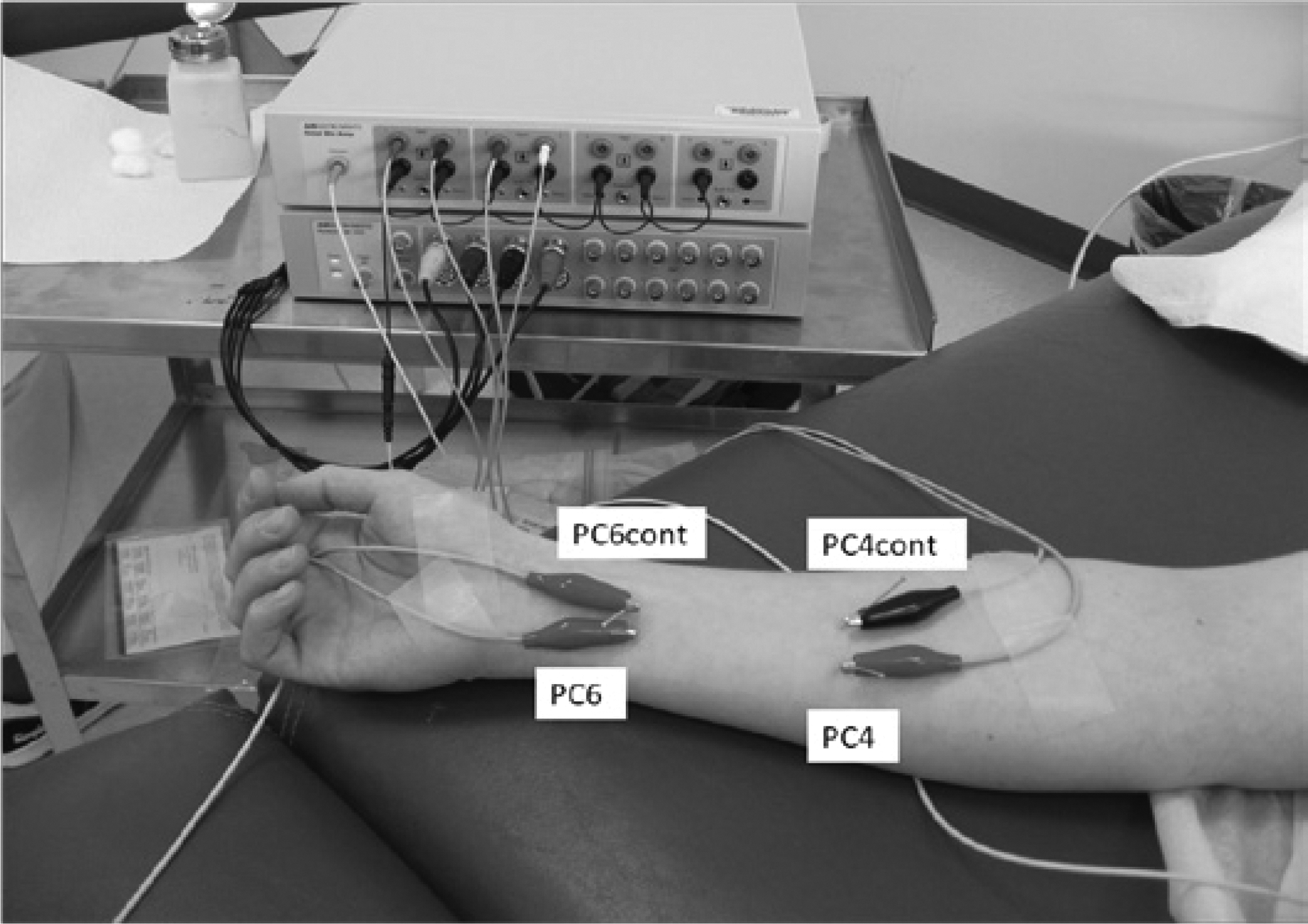
Positioning of the needles and electrodes on the anterior forearm.
Protocol
Each study subject had four needles inserted on either the right or left forearm (PC 4 and a nearby nonacupoint (PC4 cont), PC 6 and a nearby nonacupoint (PC 6cont). The nearby nonmeridian points were located halfway between the PC and Triple Energizer (TE) meridians (Fig. 1). The proximal needle electrodes at PC 4 and PC 4cont were stimulated three times each for 10 seconds with a 3-minute interval between stimulations. Continuous measurements of the bioelectric potential were recorded at all four needle electrodes.
The four needles were inserted in random order according to a Matlab randomization program. Each participant had a unique sequence. In addition, the order of needle stimulation of the proximal needles was performed randomly; another Matlab program accomplished this randomization of the order with a minimum of three stimulations for each PC 4 and PC 4cont.
All participants were lying supine for the whole study. Participants rested for 5 minutes after the needles were inserted, prior to stimulating the needles and recording measurements.
The BioAmp ground-reference electrodermal electrode was placed just proximal to the medial malleolus on the opposite side of needle stimulation (side was determined randomly). In addition, a common-reference electrodermal electrode was placed just below each paraticipant's umbilicus, providing the negative input to the four instrumentation amplifiers for all bioelectric potential measurements.
Four needles (PC 4, PC 4cont, PC 6, and PC 6cont; Fig. 1) were inserted unilaterally in each participant in a random order. Exact needle placement and depth of the insertion was determined by the experienced acupuncturists, who were informed ahead of time of the sites to be needled.
Crocodile clips were attached to all needles and not allowed to touch the skin. Each associated lead was input to the positive terminal of the four instrumentation amplifiers. Bioelectric potential measurements were taken, and data were acquired throughout the duration of the protocol. The subjects were instructed to wait for 5 minutes
Needle stimulations were implemented on the proximal needles (randomly chosen between PC 4 and PC 4cont). A thrust-needle stimulation was performed on the first choice for 10 seconds, with the acupuncturist's intention of producing a De Qi response. After a wait of 3 minutes, the next randomly chosen proximal needle was stimulated. This was continued until there were three stimulations for each of the two points. All needle-insertion depths and thrust stimulations were determined by the experienced acupuncturists. The time to start and stop stimulation was determined by an operator; the same operator worked for for all 14 participants.
At the completion of the test, after ∼20 minutes, data acquisition was stopped, and the crocodile clips, the acupuncture needles, and the two electrodermal electrodes were removed.
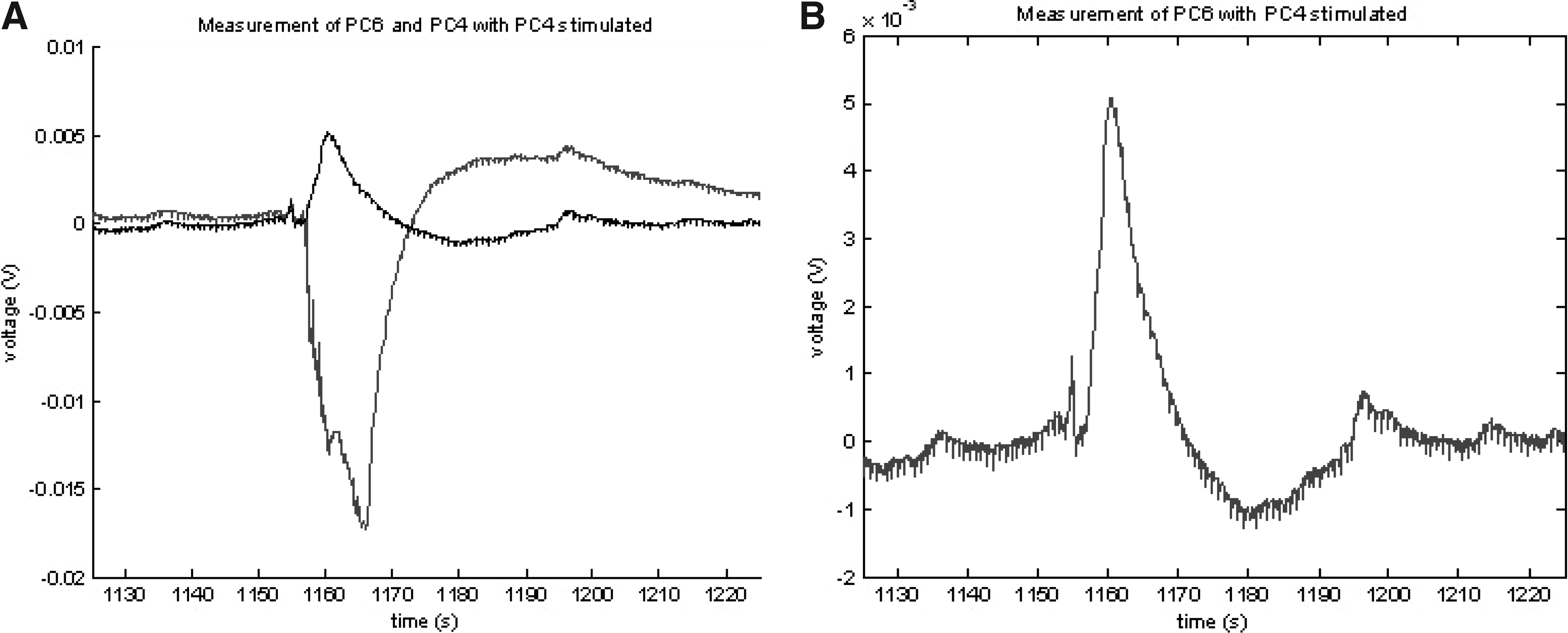
Measured outcomes of the bioelectric potential measurements were in real time. Depolarization peak voltage (mV) at the site of stimulation (PC 4 with PC 4 stimulated and PC 4cont with PC 4cont stimulated) was averaged over the three measurements. Figure 2A, illustrating data obtained from 1 participant (#12), shows a depolarization peak of 45 mV for this event. Other outcomes observed were the induced polarization peak voltage at PC 6 when PC 4 was stimulated and at PC 6cont when PC 4cont was stimulated averaged over the three measurements (In Fig. 3A and B, that is 5mV). Finally, polarization peak voltage was induced at PC 6, when PC 4cont was stimulated, and at PC 6cont, when PC 4 was stimulated. To determine if the amplitude of the two responses were statistically different, a Student's t-test was performed in Matlab.

Bioelectric potential change at the site of stimulation, whole period
Polarized potential change distal to the site of stimulation, whole period
Results
The results are presented in two ways. First, graphic examples of the depolarizations (at the site of stimulation, PC 4 or PC 4cont) and induced polarization (which occurred distally from the site of stimulation) are shown in this article. These illustrations highlight the bioelectric potential shape change as well as the change in signal period. Second, the measured outcomes are presented in tabular form in this article.
Bioelectric Potential Measurements at the Site of Stimulation
While the acupuncturist stimulated the needle at the proximal point (PC 4 or PC 4cont) the BioAmp acquired the bioelectric potential at PC 4 and PC 4cont. Graphic examples of the depolarizations and polarizations are shown in Figures 2A and B, 3A and B, and 4A and B.

Bioelectric potential change at the site of stimulation, whole period
Figure 5 shows the average of the three peak depolarization of the bioelectric potential at PC 4 when PC 4 was stimulated and at PC 4cont when PC 4cont was stimulated for all 14 participants.

Peak depolarizations at site of stimulation for all participants.
Induced Bioelectric Potential Distal to the Site of Stimulation
While the acupuncturist stimulated the proximal sites (PC 4 or PC 4cont) the BioAmp acquired the bioelectric potential at PC 6 and PC 6cont. Figures 3A and B exemplify the timing of the induced signals that occurred at two sites distal to the site of stimulation. The signal began almost immediately as the acupuncturist started stimulation but showed a much shorter time of returning back to 0V (∼40–50 seconds, compared to 3 minutes for the signal at the site of stimulation). Also the amplitude is much smaller (in the 1–5 mV range, compared to the 40–50 mV range for the signal at the site of stimulation). Figure 3B shows a magnification of the induced polarization. The induced signal has a much smaller amplitude, a different signal pattern, and an opposite polarity away from the site of stimulation.
Figure 6 shows the average of the three peak polarizations of the bioelectric potential at PC 6 (when PC 4 was stimulated) and PC 6cont (when PC 4cont was stimulated) for all 14 participants. Although needling in some participants (#7, #10, #13) elicited larger bioelectric potentials at PC 6cont than at PC 6, the majority of participants had a larger signal at PC 6. In addition, Fig. 6 highlights that 7 of the 14 participants had substantially greater responses to needle stimulation, which contributed to the statistical significance.

Peak polarizations at site distal to the site of stimulation for all participants, with measurements along same channel.
Finally, to determine if the increased amplitude found on PC 6 with PC 4 stimulated was the result of the site of stimulation and placement of measurement or just the site of stimulation, another analysis was completed. Figure 7 shows the average of the three peak polarizations of the bioelectric potential at PC 6cont (when PC 4 was stimulated) and at PC 6 (when PC 4cont was stimulated).

Peak polarizations at site distal to the site of stimulation for all participants, with measurements at adjacent channel.
Statistical data for all three measurement sets are shown in Table 1. The response at the distal acupoint (PC 6) versus the distal nonacupoint control (PC 6cont) when PC 4 and PC 4cont were stimulated respectively, was significantly different. However, there was no difference in the bioelectric potential response at the site of stimulation when the stimulation was performed either at a point on the meridian (PC 4) or at a control site (PC 4cont), and there was no difference in the bioelectric potential response at the distal acupoint (PC 6) when the control point (PC 4cont) was stimulated versus the potential at the distal nonacupoint (PC 6cont) when the acupoint (PC 6) was stimulated.
STD, standard deviation; w, with; cont, control.
Discussion
There are three main takeaway points from the study data. First, a large, slow-moving bioelectric potential depolarization occurs in the soft tissue at the site of needle stimulation. Once the acupuncturist removes his or her hand, this depolarization swings back past 0 and settles at 0 mV after about 3 minutes. This large depolarization (>–100mV) is not statistically greater when the acupuncture point is stimulated than when the control site is stimulated.
Second, there exists a translation phenomenon that occurs away from the site of stimulation. An induced polarized signal, up to ∼5mV, lasting for a total of 40 seconds, occurred adjacent to the site of stimulation as well as distal to the site of stimulation. This translation phenomenon also occurred if either the acupuncture point or the control site was stimulated. This may provide an electrophysiological explanation for why it is difficult to differentiate the effects of verum acupuncture from sham acupuncture. Despite clinical researchers' attempts to minimize the impact from the sham acupuncture, an electrical response may still be evoked from the sham intervention with possible clinical significance.
But what causes the induced polarization at the distal site? In typical conduction of electrical signals, a source point initiates conduction through a medium and at the receiver. The signal normally has the same general pattern but with added noise and an attenuated amplitude. The current study results are in contrast to this typical phenomenon. The signal shown in Figure 3B looks nothing like that shown in Figure 2A. The current authors postulate several individual mechanisms or combinations thereof. There may be a piezoelectric effect on the collagen fibers caused by the needle stimulation. 10 Diffusion potentials may arise from changes in the local area related to the needle stimulation, or there may be streaming potentials, with needle-induced fluid movement leading to potential changes of in different direction. 11
The third important finding is that a signal with statistically greater amplitude appeared only when a verum acupuncture point was stimulated and when the distal measurement was recorded on the acupuncture meridian. A clinically relevant correlate of the greater amplitude may be that a therapeutic effect results from stimulating both verum and sham points, but the effect is greater when the true acupoint is needled.
Why was this dramatic bioelectrical response at the needle not seen before? A waveform similar to that seen in Figure 2A has been reported. 12 This waveform pattern appears to depend on the positioning of the reference electrode. Biomedical researchers have not studied low-frequency content, generally, because they are more concerned with higher-frequency signals and consider such low-frequency spectral contents as artifacts to be filtered out with high-pass filters. In addition, as mentioned, the predominance of electrical investigation of acupuncture is concerned with measuring electrical impedance rather than endogenous bioelectric potentials.
There were a number of limitations to this exploratory study, including placement of the common reference electrode (below the umbilicus), use of an acupuncture needle as the recording electrode, and lack of blinding of the acupuncturists who performed the needle stimulations. Muscular movements in the abdomen associated with talking on the part of participants created a noise floor acting as an artifact. A better choice for reference-electrode placement for this study, and any other that used only one extremity would have been a static point on the opposite leg. If comparing a number of extremities, the forehead might be a good centralized static site for the reference point. Another limitation was the use of an acupuncture needle as a recording electrode; because the needle is conductive throughout, it is impossible to tell which layer of tissue—dermal or epidermal—may be more important for the bioelectric response at the needle stimulation as well as the bioelectric-induced signal distal to the point. Finally, the acupuncturists were not blinded to the verum acupuncture points and control sites. Athough the current authors requested that acupuncturists use the same thrust technique on the acupuncture points and control sites, the force that was actually used was not controlled.
Conclusions
This study's findings suggest electrophysiological uniqueness in the form of a greater bioelectric potential amplitude when a proximal acupoint is stimulated and the response is measured at a distal acupoint along the same meridian. This is compared to stimulation on a control site and measuring on a distal control site as well as stimulation on the control site and measuring on a distal site on the adjacent acupuncture meridian.
Numerous phenomena were seen during the investigation of the bioelectric potential. First, there was a large depolarization at the site of acupuncture-needle stimulation. Second, there were significant differences in amplitude among people and among stimulations on the same person. Third, the reference point placement played an important role in the bioelectric potential amplitude measurement.
Footnotes
Acknowledgments
The author (K.S.) would like to acknowledge the support of the NESA for providing a fellowship to undertake the investigation on the bioelectric potential of acupuncture-needle stimulation.
Disclosure Statement
No competing financial interests exist for any of the authors.