
Abstract
Abstract
Background:
Acupuncture is being used increasingly to treat gynecologic and obstetric disorders.
Objective:
The aim of this review was to determine the efficacy and safety of acupuncture for treating pelvic and low-back pain during pregnancy, pain during labor, primary dysmenorrhea, and menopausal symptoms.
Design:
This is an overview of systematic reviews (SRs) and randomized controlled trials (RCTs).
Search strategy:
A literature search was conducted, in July 2010, in MEDLINE,® the Cochrane Database of Systematic Reviews, CENTRAL, the Database of Abstracts of Reviews of Effects, and Tripdatabase.
Selection criteria:
Published SRs and RCTs found during the literature search were included as well as RCTs that were published after completion of the literature search.
Analysis:
Data from SRs and RCTs that provided quantitative information were pooled.
Results:
Eight SRs and nine RCTs were included. One SR and 4 RCTs showed that acupuncture reduced pelvic and low-back pain, compared to physiotherapy or usual prenatal care. Results were contradictory when interventions were compared with sham acupuncture. With respect to reduction of pain during labor, two SRs showed no differences between acupuncture and sham acupuncture. None of the three SRs included on primary dysmenorrhea produced conclusive results. Two SRs of studies on menopausal symptoms showed no differences between acupuncture and sham acupuncture. A meta-analysis of three additional RCTs identified a favorable effect of acupuncture for reducing frequency and intensity of hot flashes. Adverse effects were mild and infrequent.
Conclusions:
Evidence for the efficacy of needle acupuncture for treating the disorders evaluated remains inconclusive. The intervention showed promising results for reducing pelvic and back pain during pregnancy and climacteric vasomotor symptoms, although well-designed studies are needed to make the results more precise and reliable.
Introduction
G
Acupuncture is based on the principles of Traditional Chinese Medicine, according to which the functioning of the body is under the control of Qi, which flows through meridians. This theory posits that disease is an imbalance in the flow of Qi; acupuncture is used to correct this imbalance via insertion of needles that stimulate skin spots located along the meridians. 3 There are other acupuncture-like techniques that do not involve using needles. Instead, stimulation is applied through pressure (acupressure), a laser, or by combustion of the root of Tanacetum parthenium, commonly known as feverfew (moxibustion).
Acupuncture is increasingly being recommended worldwide, especially for treating pain. Several hypotheses have been proposed to explain acupuncture's analgesic effect. Some researchers suggest that acupuncture activates A-δ fibers, which are involved in release of endorphins and are associated with an increase in levels of 5-hydroxytryptophan (a serotonin precursor) in the brain. 4 It has been found that acupuncture points correspond to anatomical and physiologic characteristics, such as the areas of the body where peripheral nerves connect. An alternative mechanism is that needles may inactivate highly sensitive neuralgic areas in the muscles responsible for causing referred pain in a body area.
An increasing number of health care centers offer acupuncture for treating various ailments, including some gynecologic and obstetric disorders. Given the increasing use of this technique, it is essential to perform an objective and rigorous evaluation of its effectiveness and efficiency by conducting well-designed studies. In recent years, several clinical studies have been published on the use of acupuncture for treating obstetric and gynecologic disorders, such as pelvic and low-back pain during pregnancy, pain in labor, primary dysmenorrhea, and climacteric symptoms. However, these studies have produced inconclusive results. The objective of this overview was to determine the efficacy and safety of needle acupuncture for managing these disorders.
Methods
Inclusion and Exclusion Criteria
The current authors included systematic reviews (SRs) of randomized controlled trials (RCTs) on the efficacy and safety of acupuncture with needles in women, age 16 or older, who were affected by the following gynecologic and obstetric disorders: (1) low-back and pelvic pain during pregnancy; (2) pain during labor (excluding patients who assessed pain associated with interventions such as surgical repair of lacerations or episiotomy); (3) primary dysmenorrhea, and (4) climacteric symptoms. For the latter disorder, women with spontaneous or surgical menopause were included, but those with menopause caused by cancer treatment were excluded. To increase the comprehensiveness of this review, RCTs were also included that published after the date of completion of the literature search of the included reviews.
Studies that had the following controls were assessed: (1) sham acupuncture or placebo, which deviates from the theory of acupuncture in at least one of the aspects that is considered to be crucial, such as penetration of the skin or needle placement in the correct acupuncture points or (2) no acupuncture, defined as any standard treatment prescribed for the disorder of interest. Studies that used the experimental treatments as controls were excluded, as well as studies in which the control group received different care than the treatment group. 5 Studies on electroacupuncture (EA) were excluded as well as studies or that assessed other methods of stimulation that did not involve insertion of needles (e.g. laser, transcutaneous electrical nerve stimulation, moxibustion, or acupressure). Also excluded were narrative reviews and SRs that did not specify a search strategy or that did not assess the risk of bias of included studies. RCTs that did not use an adequate method of randomization were also excluded.
The outcomes of interest were pain and menopausal symptoms. Studies that assessed pain should have used a measure of pain as the main outcome, preferably reported by patients using a visual analogue scale (VAS). 5 Studies that evaluated menopausal symptoms should have used, preferably, changes in scores of menopausal symptoms (e.g., Kupperman Index, Menopause Rating Scale Score Nordin, or Mac Lennan Score). 6 The frequency and intensity of vasomotor symptoms were also considered.
Literature Search
In July 2010, a literature search was conducted in MEDLINE,® the Cochrane Database of Systematic Reviews, CENTRAL, the Database of Abstracts of Reviews of Effects (DARE), and Tripdatabase. Health technology assessments were identified to detect additional RCTs and SRs, and references lists of included studies were also reviewed. Studies published in English, Spanish, French, Italian, Portuguese, and German were included. Two of the current authors reviewed the titles and abstracts independently of all retrieved references to select those that were potentially eligible for this review. Subsequently, the 2 authors evaluated the full-text publications of the selected studies to determine whether or not to include them. Disagreements were solved by consensus or by consulting with a third reviewer (a detailed search strategy is provided in Appendix 1; online only). 7
Two reviewers assessed the risk of bias independently of the included studies. Any disagreement was solved by consensus or by consulting with a third reviewer. Risk of bias was assessed using the AMSTAR [
Data were extracted from included studies in descriptive tables (see Appendix 3; online only ) with information regarding risk of bias, interventions, characteristics of the participants, outcomes, and main study results. A collection was performed of effect estimates (and their 95% confidence intervals [CIs]) expressed as relative risk (RR) for dichotomous outcomes and mean differences (MD) for continuous outcomes and for outcomes of interest from included SRs. The latter were standardized (standardized mean difference [SMD]) when the same outcome was measured using different scales.
Whenever possible, quantitative data were combined from new RCTs using meta-analyses. In accordance with the Cochrane Collaboration approach, 7 a Mantel-Haenszel model was used, which applies a random-effects model, given the expected heterogeneity between the included studies. Heterogeneity was assessed using the I 2 statistic, with a threshold of 50%–70% as a sign of substantial heterogeneity. 7 In these cases, data were not combined in meta-analyses, and results were presented in narrative form. All statistical calculations were conducted using RevMan 5.0.
Results
The literature search yielded 728 references, of which 614 were excluded based on the information contained in their titles and abstracts. The full texts of the remaining 114 articles were assessed, of which 17 were included. These were eight SRs10–17 and nine RCTs18–27 (Fig. 1). Excluded studies and reasons for exclusion are listed in Appendix 4 (online only ).
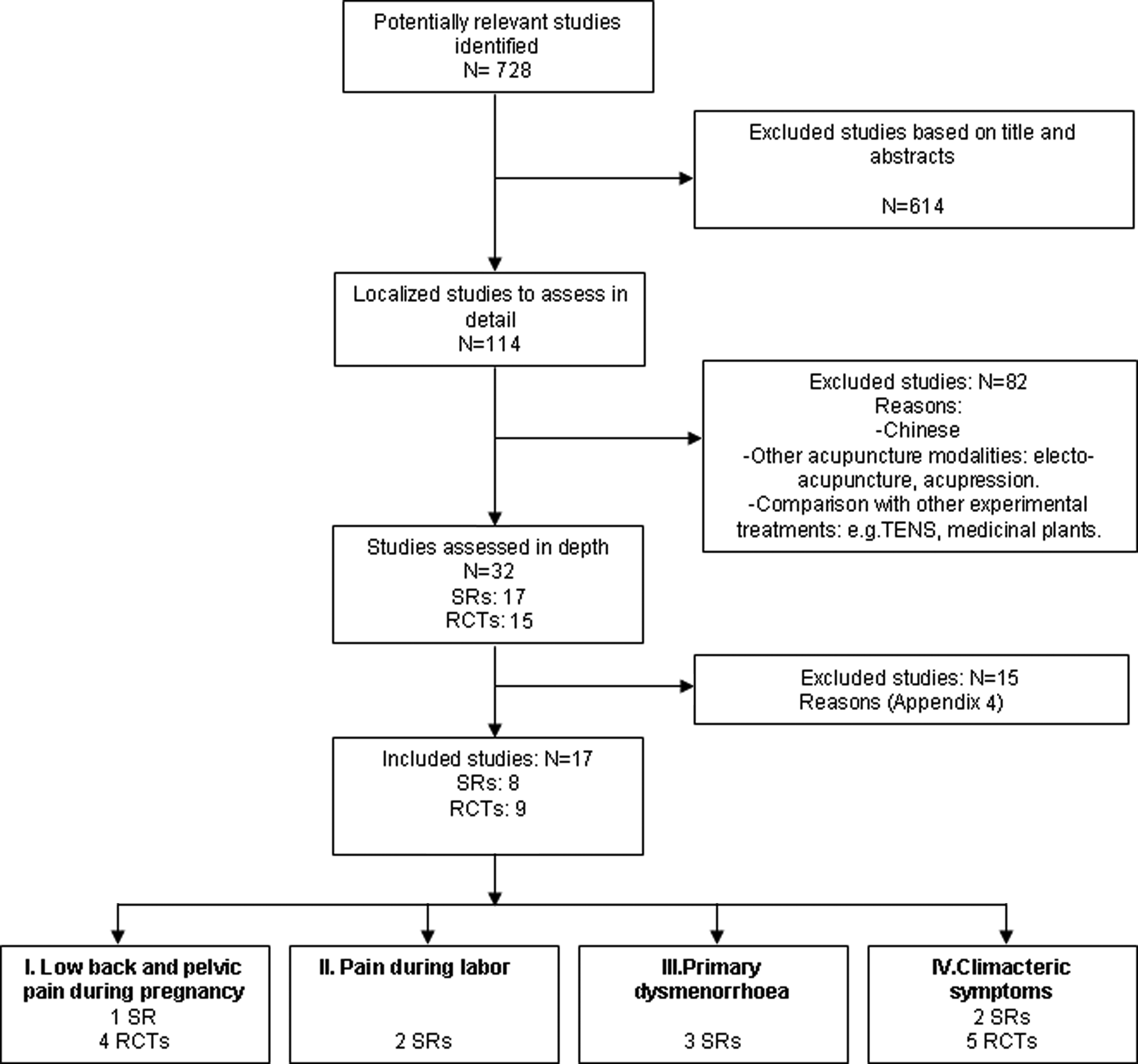
Identification of eligible studies for the overview. TENS, trancutaneous electrical nerve stimulation; RCT, randomized controlled trial; SR, systematic review.
Of the eight SRs included, five were of high methodological quality (AMSTAR scores 9–10).10–12,15,16 Three Cochrane reviews10,11,15 showed the highest quality. The remaining SRs did not provide lists of excluded studies and did not assess publication bias.13,14,16 The characteristics of the included SRs are shown in Table 1.
AMSTAR [
For full references for these RCTs, consult the references in the first column of this table.
RCT, randomized controlled trials; SR, systematic review; VAS, Visual analogue scale; ADLs, activities of daily living; MDQ, menstrual discomfort questionnaire; HRQoL, Health-Related Quality of Life.
The assessment of the risk of bias of the nine RCTs included are in Table 2. The main source of bias among these RCTs was the lack of blinding of interventions. Only three studies blinded participants and evaluators,19,20,23 the rest were open studies.18,21,22,24–27
For quality assessment, the Jadad scale is used to assess five items: (1) Was the study described as randomized?; (2) Was the method of randomization described in the article, and was that method was appropriate?; (3) Was the study described as double-blinded?: (4) Was the the method of blinding described, and was it appropriate?; (5) Was there a description of withdrawals and dropouts? See Appendix 2 (online only )
VAS, visual analogue scale; N/A, not available; TCM, Traditional Chinese Medicine.
Low-Back and Pelvic Pain During Pregnancy
For this outcome, a Cochrane review 10 of high quality was identified; it included three RCTs (a total of 356 women). Four more RCTs18–21 were added that had been published after the literature search was conducted for this review.
Two of the RCTs included in the Cochrane review compared acupuncture with usual care.28,29 One study showed that women treated with acupuncture had less pelvic pain in the morning than those who only exercised. 28 Mean differences with respect to baseline were 12 mm on a 100-mm VAS (95% CI: 5.9–17.3; p<0.001) and 9 mm (95% CI: 1.7–12.8; p=0.031) for both groups, respectively. When assessing pain intensity in the afternoon, the results also favored acupuncture. There was a follow-up to this study published after the SR, which showed a 99% decrease in pain at 12 weeks after birth, regardless of treatment group. 18 The other study included in the Cochrane review 29 showed results that favored acupuncture, with a decrease in pain in 60% of women treated with acupuncture, compared to 14% of those who received usual prenatal care. This study, however, did not report treatment duration.
The third study included in the SR, compared acupuncture versus physiotherapy and found a greater reduction in pain intensity both during the day and at night in an acupuncture-treated group. 30
With respect to the four RCTs published after the literature review, three compared verum acupuncture versus sham acupuncture. One of the RCTs included 70 women and compared classical acupuncture (with deep stimulation) to acupuncture with surface stimulation. 21 Pain intensity decreased in the classical acupuncture group, but the small size of the groups did not justify a conclusion that there were any differences between the two kinds of treatment. Another study that included 115 women did not find differences in pain reduction between the groups treated with verum acupuncture and sham acupuncture. 19 The last study (N=159) compared verum auricular acupuncture with sham auricular acupuncture and self-care. 20 After 1 week of treatment, 80% of the participants treated with verum acupuncture had a significant reduction in pain, compared with 56% of the subjects in the sham acupuncture group (p=0.001) and 36% of the self- care group (p<0.001). There was no difference in pain reduction between the sham acupuncture group and the self-care group (p=0.46). More women in the verum acupuncture group had a reduction of pain that could be considered clinically significant (a 30% reduction) than in the sham acupuncture and the self-care groups (81% versus 59% versus 47%; p=0.015).
The results of two RCTs19,28 were pooled for the proportion of women with pelvic pain when rolling over in bed (Fig. 2). Data were included from 370 women, and the results favored acupuncture (RR=0.85, 95% CI: 0.74–0.98). Two other RCTs18,29 provided data on pain reduction reported by pregnant women, but these data could not be combined because of the presence of statistical heterogeneity, possibly caused by differences in time of evaluation. Data from two RCTs19,30 were also pooled for the proportion of women that assessed the treatment as good or excellent. This analysis included 161 women and did not yield differences between the groups (RR=1.12, 95% CI: 0.92–1.35).

Low-back and pelvic pain while turning in bed. CI, confidence interval; Mantel-Haenszel model.
Pain During Labor
Two SRs11,12 were included that included, globally, seven RCTs on acupuncture with needles. The main comparisons were acupuncture versus standard analgesic treatment, no treatment, and sham acupuncture.
One SRs was a Cochrane review that included three RCTs. 11 Two of these compared acupuncture with no treatment (N=288), which were combined in a meta-analysis that showed greater use of analgesics in the untreated group (RR=0.70, 95% CI: 0.49–1.00). The other RCT compared acupuncture with sham acupuncture. Use of analgesics was lower in the acupuncture group (RR=0.72, 95% CI: 0.58–0.88).
The other SR 12 included seven RCTs (a total of 1483 women), three of which had also been included in the Cochrane review. 11 The researchers conducted a meta-analysis of three of the seven RCTs, and found no differences in mean pain between a verum acupuncture group and a sham acupuncture group at 30 minutes (MD: −10.79 mm using a VAS of 100 mm, 95% CI: −35.16 to −13.58), 60 minutes (MD: −8.02 mm, 95% CI −1.88 to −5.84), or 120 minutes (MD: −10.15 mm, 95% CI −23.18 to −2.87). Another study compared acupuncture with no treatment, finding no difference in pain reduction at 60 minutes (MD: 2.60 mm, 95% CI −6.29 to −11.49) and 120 minutes (MD: 5.50 mm, 95% CI −3.34 to −14.34). There was also a meta-analysis of the remaining studies, which compared acupuncture and conventional analgesia, and this analysis showed a lower requirement for meperidine in women treated with acupuncture (RR=0.20, 95% CI: 0.12 to −0.33) but there were no differences between groups regarding epidural analgesia (RR=0.68, 95% CI: 0.46 to −1.00).
Primary Dysmenorrhea
This outcome was assessed in three SRs that included a total of 16 RCTs.13–15 Four studies compared acupuncture against standard therapy (nonsteroidal anti-inflammatory drugs [NSAIDs] and/or oral contraceptives) found that acupuncture contributed to a reduction of symptoms measured with different pain scales (SMD: 0.92 [95% CI: 0.20–1.65], SMD: 0.69 [95% CI: 0.31–1.07], SMD: 0.73 [95% CI: 0.36–1.10], and SMD: 0.59 [95 CI: 0.22–0.96]).14,15 With respect to the percentage of women experiencing pain relief as a dichotomous outcome, five comparisons found that acupuncture was better than pharmacologic therapy, but another five comparisons did not find any differences.13–15
Two studies evaluated the use of acupuncture applying heat. One of the studies found that acupuncture was superior to treatment with NSAIDs (RR=1.39, 95% CI: 1.09–1.76), but the other did not find any differences. 14
Four studies compared verum acupuncture to sham acupuncture, and all reported a reduction in pain in both study groups. One study with 48 women included in the three SRs,13–15 found that acupuncture was associated with greater pain reduction (90.9% versus 36.4%; p<0.05). In contrast, the remaining three studies found no differences between the groups.14,15
Quality of life was assessed in two trials. 15 One identified an improvement among women treated with acupuncture, compared with usual care in the areas of body pain, mental health, vitality, social function, and emotions. The other study found no differences in these parameters, compared to sham acupuncture.
Climacteric Symptoms
Two SRs were included: one coverd four RCTs 16 and the other covered seven RCTs. 17 In addition, five more RCTs22–27 were included; these were published after the literature search for these SRs. The outcomes measured in most studies were vasomotor symptoms.
Of the seven studies included in the one of the SRs, 17 two used hormone therapy as a control group, whereas another used oryzanol, an antioxidant found in rice bran oil. The remaining four trials, also included in the other SR, 16 used sham acupuncture. In three of these studies, there was no difference between verum acupuncture and sham acupuncture regarding frequency, severity, or rate of hot flashes. However, the results of a pilot study of 29 women that also compared verum acupuncture with sham acupuncture suggested favorable effects of verum acupuncture on the severity of hot flashes.
Three of the five RCTs published after the aforementioned SRs compared verum acupuncture and sham acupuncture.22,23,27 One of the RCTs 22 found that the severity of nocturnal hot flashes decreased significantly in a verum acupuncture group (27.84±6.26 versus 30.67%±18.49%; p=0.017), although there was no statistically significant difference in the frequency of hot flashes (23.72±45.68%; p=0.170). Another trial 23 found that a verum acupuncture group had a reduction in severity of hot flashes from baseline to the second (p=0.05), third (p=0.005), and fourth (p=0.019) months, while a sham acupuncture group had no change. The third study 27 found no difference between groups in any of the parameters measured, although both groups improved significantly after 2 weeks of treatment.
The remaining RCTs compared acupuncture with self-care or usual care.24–26 One of the RCTs 26 found that, after 4 weeks of treatment, the reduction in score for hot flashes at 24 hours was higher in an acupuncture group than in a control group (−16.57 versus −6.93; p<0.0001). The frequency and severity of hot flashes was also lower in the acupuncture group. The other trial24,25 noted that the frequency of hot flashes decreased by 5.8% and 3.7% in 24 hours in an acupuncture group and a control group after 12 weeks of treatment, respectively (p<0.001), although the differences did not remain at 6 and 12 months (p=0.3 and 0.2, respectively).
Only three studies of those published after the literature search of the SRs could be pooled for assessing frequency and intensity of hot flushes.22,24–26 For the former outcome, data from 452 women were combined, showing favorable results of acupuncture (SMD=−0.59; 95% CI: −0.79 to −0.39; Fig. 3A). For the latter, data from 422 women were combined, also showing favorable results of acupuncture (SMD=−0.56; 95% CI: −0.76 to −0.36; Fig 3B). Two studies26,27 reported the outcome “hot flush score,” but their results could not be combined because of heterogeneity of the studies.
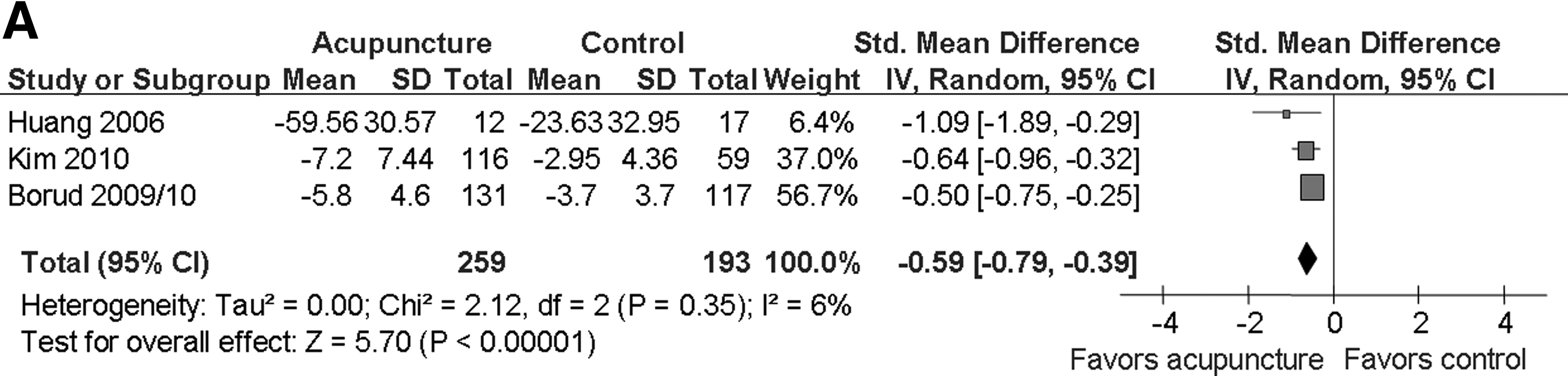
Frequency
Adverse Effects
Few studies provided data on adverse effects (AEs). AEs were uncommon in these studies, and, when these effects did occur, they were mild and transient. Data from only two studies could be pooled.18,22 Data from two RCTs (144 women) showed no difference between verum acupuncture and sham acupuncture in proportion of women that complained of pain when needles were being inserted (RR=0.94, 95% CI: 0.48–1.63; Fig. 4A). For insomnia (2 RCTs, 144 women), no differences were observed between the groups (RR=1.45, 95% CI: 0.41–5.12; Fig 4B).

Adverse effects.
Discussion
This overview was performed to examine the effectiveness and safety of acupuncture for treating some common gynecologic and obstetric disorders. The results of this review showed that acupuncture seems to alleviate pelvic and low-back pain during pregnancy, compared to usual prenatal care or physiotherapy. However, when verum acupuncture was compared with sham acupuncture, the results were conflicting. The results of the two SRs on acupuncture for pain relief during labor showed no differences when comparing verum acupuncture versus sham acupuncture.12,13 However, verum acupuncture was associated with a lower use of analgesics. None of the three SRs that evaluated the use of acupuncture for treating primary dysmenorrhea could reach conclusions about acupuncture's effectiveness. With respect to the effect of acupuncture on climacteric symptoms, none of the reviews found any differences between verum acupuncture and sham acupuncture in severity and frequency of hot flashes. Data from three newer RCTs (one of which was published in 2009 and had follow-up results published in 2010)22,24–26 were combined in a meta-analysis, which showed a favorable effect of acupuncture for reducing frequency and intensity of hot flashes. However, the outcome assessment was blinded only in one of the included trials. 22
Overall, it appears that acupuncture's main benefit involves reducing pelvic and low-back pain during pregnancy and primary dysmenorrhea, compared with usual care or no treatment. However, when verum acpuncture was compared with sham acupuncture or a proven treatment (such as NSAIDs in the case of the primary dysmenorrhea), the results were contradictory.
Similarly, a recent published study that performed an individual patient data meta-analysis of RCTs of acupuncture for chronic pain also found a greater effect of acupuncture when it was compared with a nonacupuncture control than when verum acpuncture was compared with sham acupuncture. Although the researchers found that verum acupuncture was superior to sham acupuncture, these differences were relatively modest and much lower than differences from comparison of acupuncture with a nonacupuncture control. 31 Other SRs that assessed the use of acupuncture for treating different conditions also found an acupuncture effect when acupuncture was compared with usual treatment, but there were no significant differences when verum acupuncture was compared with sham acupuncture.32–34
The results of three more-recently published SRs on gynecologic and obstetric disorders35–37 drew similar conclusions to this overview. One 35 evaluated the use of acupuncture and acupressure in pain management during labor, and another SR 36 evaluated the use of acupuncture for treating common reproductive health disorders, including primary dysmenorrhea and climacteric symptoms. Both reviews concluded that there was insufficient evidence to make recommendations for or against using acupuncture to treat these conditions. The third SR was a comprehensive review that included 16 SRs 37 on the effectiveness of acupuncture and EA for treating various gynecologic disorders. With respect to primary dysmenorrhea and climacteric symptoms, this review included the same SRs identified in the current overview,13,14,16,17 and the researchers of the third SR concluded that there was insufficient evidence for the effectiveness of acupuncture for treating primary dysmenorrhea and vasomotor symptoms.
Few studies included in the current overview reported on the safety of acupuncture adequately. However, acupuncture can be considered a safe procedure with a low incidence of AEs; those AEs that did occur were mild.
It is noteworthy to mention the short follow-up of participants in the included RCTs, precluding any conclusion about the long-term benefit of acupuncture for these conditions. Even some studies on low-back and pelvic pain during pregnancy followed-up patients just for 1 week. For studies on primary dysmenorrhea and climacteric symptoms, which are two conditions that can linger over time, most studies followed up patients for less than 3 months, and only three of the studies had long-term follow-ups (12 months).
Although the methodological quality of the included reviews was high or very high, the RCTs included had important methodological limitations. With respect to the newer RCTs included, there were adequate concealment of randomization sequence, handling of dropouts, and reporting of results, although two studies did not describe the method of randomization.
The design and implementation of RCTs on acupuncture is challenging, especially with respect to blinding these trials. This is particularly important when assessing subjective outcomes such as pain. In the case of acupuncture, it is impossible to blind the acupuncturist, and therefore it is essential that both patients and staff responsible for assessing outcomes be unaware of the intervention allocation.
Another issued related to RCTs on acupuncture is the choice of a comparison group. Ideally, sham acupuncture must be used to demonstrate the effectiveness of the intervention (verum acupuncture). This has been proposed to offset the potential “placebo effect” of acupuncture, 38 although some researchers suggest that sham acupuncture can stimulate production of opioids in the body in a manner similar to conventional acupuncture, and therefore have an analgesic effect. 39 Consequently, the best design to evaluate the efficacy of acupuncture would be a three-armed RCT that compared groups treated with verum acupuncture, sham acupuncture, and no treatment. However, blinding of the patients in such a study would not be possible.
One of the main strengths of this overview is that a comprehensive literature search was conducted. In addition, to increase its comprehensiveness, RCTs were also included even if they were published after the date of completion of the literature search of the included SRs. Whenever possible data were extracted and combined from primary studies to provide new results. Studies conducted in various countries and published in different languages were included, although, this was not the case for Eastern languages. However, some of the SRs did include RCTs conducted in Eastern countries, which ruled out the impact of geographic or linguistic bias.
Conclusions
The available evidence on the effectiveness of acupuncture for treating gynecologic and obstetric disorders remains inconclusive and, therefore, does not yield conclusions about acupuncture's benefits. It may have some effect for reducing pelvic and low-back pain during pregnancy and also may reduce frequency and intensity of hot flashes during menopause. However, the small sizes of the studies included in this review and the difficulties related to masking the outcome assessment prevented the current authors from drawing any firm conclusions.
Footnotes
Acknowledgments
The authors thank Hector Pardo for the editing support.
This project was funded by the Instituto de Salud Carlos III (record number PI09/90578), in Spain.
X.B.C., M.J.M.Z., and Z.S. conceived the study. I.S. performed the search. Z.S. and A.S.O. selected the included articles and extracted data. M.J.M.Z., Z.S., and A.S.O. analyzed data. A.S.O. S.M.U., and I.S. updated the SR. A.S.O. wrote the first draft of this article. All of the authors reviewed this article critically for important intellectual content and gave final approval of the version to be published.
Disclosure Statement
No competing financial interest exists.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.