
Abstract
Abstract
Objectives:
This study examined how group auricular acupuncture may influence sleep quality, sleep patterns, and hypnotic medication use associated with PTSD-related insomnia in Operation Enduring Freedom and Operation Iraqi Freedom veterans.
Design:
This study was a randomized controlled trial with sham acupuncture and wait-list controls.
Setting:
This study took place at the Washington, DC, Department of Veterans Affairs (VA), Medical Center.
Subjects:
Thirty-five subjects were randomized to participate in the study, but only 25 subjects completed the study.
Interventions:
Subjects were randomized to one of three groups: (1) true group auricular acupuncture; (2) sham auricular acupuncture; or (3) wait-list control.
Outcome Measures:
The primary outcome measure was perceived sleep quality (as measured by Insomnia Severity Index (ISI) questionnaires and Morin Sleep Diaries [MSDs]). Secondary outcome measures were total sleep time (TST), sleep efficiency, sleep latency, naps (as measured by MSD and wrist actigraphs [WAs]), hypnotic medication use, veteran satisfaction, and attrition rates.
Results:
Subjects in the true auricular acupuncture group had a statistically significant improvement (p=0.0165) in sleep quality as measured by the ISI at time (t)=1 month. This group had a trend toward lower MSD TST at t=2 months (p=0.078), lower WA TST at t=1 month (p=0.0893), and toward higher MSD nap times than the other two groups post-treatment (p=0.0666). No statistically significant association between group assignment and hypnotic medication use and satisfaction scores were noted.
Conclusions:
Acupuncturists should consider incorporating sleep hygiene education into their clinical practices and/or collaborate with insomnia health care professionals when working with individuals with insomnia. This study also supports the finding that perceived sleep quality and objective WA measurements are not significantly correlated.
Introduction
M
The conceptual framework for this study was based on Spielman's 3-P Model of Insomnia (Fig. 1).18,19 Research has shown that perceived sleep quality has a significant impact on overall well-being20,21 (i.e., if an individual believes that s/he is experiencing poor sleep quality, this perception may aggravate some of the symptoms associated with insomnia). Consequently, perceived sleep quality was the study's primary outcome variable. The research questions for this study were:

Study model developed by research team and adapted from Spielman's 3-P Model of Insomnia. 18 TST, Total sleep time; SL, sleep latency; SE, sleep efficiency; PTSD, post-traumatic stress disorder.
(1) How does group auricular acupuncture influence the maladaptive perpetuating factors associated with PTSD-related insomnia, compared to sham acupuncture and wait-list controls? Maladaptive perpetuating factors were defined as:
(a) Perceived sleep quality; (b) Fragmented sleep patterns; and (c) Hypnotic medication use.
(2) What is the degree of veteran acceptance for group auricular acupuncture for PTSD-related insomnia? Veteran acceptance was measured using satisfaction scores and attrition rates.
Methods
The Washington, DC, Department of Veterans Affairs (VA) Medical Center's institutional review board and research and development committee granted full approval for this study prior to its commencement. This study was a randomized controlled trial (RCT). Realizing that time and attention could be confounding variables, sham acupuncture and wait-list controls were selected to optimize the likelihood that the true effects of acupuncture could be identified and that attention factors could be controlled. The wait-list control served as a strict control (i.e., this group received only conventional care with no acupuncture or sham acupuncture until time in the study was complete).
Recruitment
Letters, study flyers, and web sites were used to recruit veterans. Veterans who met initial telephone screening requirements were asked to participate in the full screening process. The main reasons for ineligibility were being a non-OEF/OIF veteran, having a history of substance abuse, having received acupuncture in the past 3 months, and having no PTSD diagnosis. The main reasons for declining to participate were scheduling conflicts, being unable to commit to study for 2 months, or study locale was too far from home. Table 1 lists inclusion and exclusion criteria.
Veterans already on an established, stable regimen of CPAP or BiPAP were eligible for study.
DSM-IV-TR is American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 4th Ed—text rev. Washington, DC: American Psychiatric Association, 2000.
OEF, Operation Enduring Freedom; OIF, Operation Iraqi Freedom; PTSD, post-traumatic stress disorder; ISI, Insomnia Severity Index; CPAP, continuous positive airway pressure; BiPAP, bilevel positive airway pressure; Audit C, Alcohol Use Disorders Identification Test—Consumption.
Group Assignments and Treatments
Table 2 describes the three study groups. All participants were followed for 2 months. Participants in true and sham acupuncture were offered two treatments per week for 8 consecutive weeks for a total of sixteen treatments. No other treatments were administered during the sessions. All sessions took place in a quiet conference room at the Washington, DC, VA Medical Center.
PTSD, post-traumatic stress disorder; CBT, cognitive–behavioral therapy.
The true and sham treatments were performed by a physician with advanced training in auricular acupuncture. A second senior-licensed acupuncturist with more than 20 years of acupuncture experience provided consultative expertise on the development of the true and sham control protocols and served as the backup acupuncturist. All acupuncture services were performed in accordance with the established principles and practices of the National Certification Commission for Acupuncture and Oriental Medicine.
To minimize variability between the true and sham groups, a standardized script was used for all study sessions. This script was also helpful on the rare occasions when the backup acupuncturist performed treatments. A critical aspect of this protocol was that the acupuncturist encouraged all subjects at the onset to engage in a state of mindfulness by noting their level of awareness of the surrounding environment and any feelings they might be experiencing. Furthermore, calming background music was played to enhance this milieu. At the end of the sessions, participants were encouraged to take a moment to reflect on their acupuncture experiences and to recall these experiences when needed. These effects were incorporated into the protocol because they are often used in clinical acupuncture sessions. Verbal communication between the participants was kept to a minimum to minimize the potential influence of group dynamics on study outcomes. A group ear acupuncture approach was adopted primarily for efficiency and to broaden access to care, as VA medical centers care for large numbers of veterans with PTSD-related insomnia. In addition, based on clinical experience, the research team believed that a group setting might also have the added benefit of serving as a possible therapeutic resource for veterans who shared similar sleep difficulties. Both the true and sham groups were structured identically to control for potential intervention effects.
Using a Traditional Chinese Medicine (TCM) map as a guide, the true acupuncture intervention used five specific auricular acupuncture points (Fig. 2) that are thought to help promote sleep. Selection of these points was based on acupuncture interventions for insomnia22–25 and the study acupuncturist's experience with OEF/OIF veterans with PTSD-related insomnia.
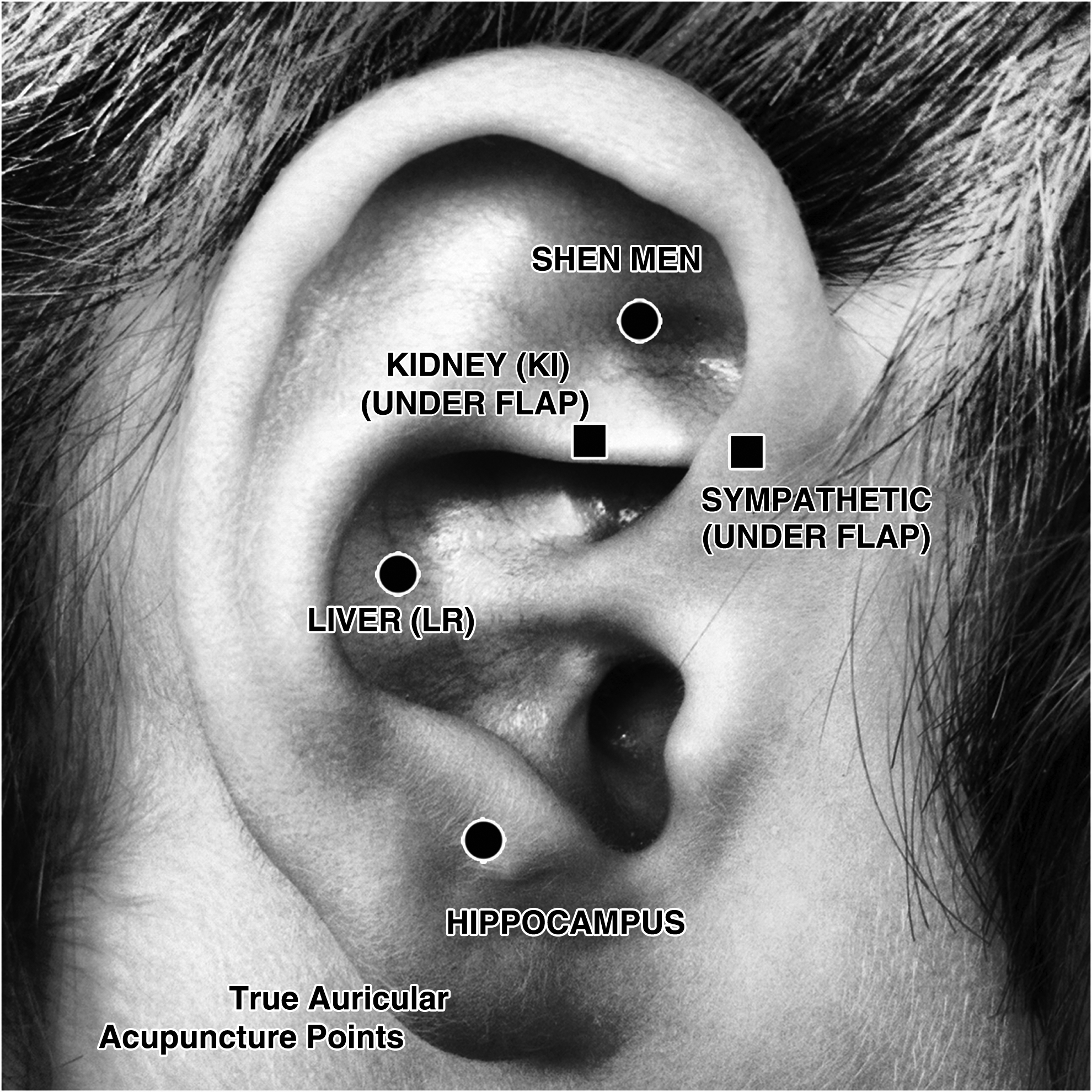
True auricular acupuncture points.
The sham intervention involved using nonacupuncture points located on the helix of the ear (Fig. 3). Selection of these points was based on consultation with the study acupuncturists and on acupuncture interventions for insomnia. 23 Delivery of this sham acupuncture was similar to the delivery of the true acupuncture in all aspects except for the points that were needled.

Sham auricular acupuncture points.
All acupuncture and sham acupuncture sessions lasted 45 minutes. The same needle type and size was used for all true and sham sessions. The needles were DBC Brand Spring Handle Needles, size 0.16×15 mm. For each of the two groups, five needles per ear were placed on the corresponding group assignment points. Needle depth for both the true and sham acupuncture depended on the auricle thickness of each participant. Needles were inserted until they reached the ear cartilage and to the depth that the needle could stand by itself. No De Qi response was sought during needle insertion, and needles were inserted straight in with no needle manipulation. No guide tubes were used. No additional needling techniques were used after needle insertion. Needles were replaced if they fell out immediately after insertion but were not replaced if they fell out during the remaining treatment time.
Table 3 shows the theoretical and operational definitions for the outcome variables.
ISI, Insomnia Severity Index; MSD, Morin Sleep Diary; WA, Wrist Actigraph; TST, Total Sleep Time; SL, Sleep Latency; SE, Sleep Efficiency.
Study Instruments
The study instruments are outlined in the sections below.
Morin Sleep Diary
The Morin Sleep Diary
Insomnia Severity Index
The Insomnia Severity Index (ISI) is a 7-item, self-report questionnaire based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revised, criteria for insomnia. 31 * It measures recent problems with (1) sleep onset, sleep maintenance, and early morning awakenings; (2) satisfaction with current sleep pattern; (3) interference with daily functioning; (4) noticeable impairment caused by sleep problems; and (5) level of distress caused by sleep problems. 31 Each item is rated on a 5-point Likert scale. Scores range from 0 to 28, with higher scores reflecting greater insomnia. 31 Good internal consistency, test–retest stability, and validity have been reported. 31 Per scoring guidelines, a cutoff total of>8 is indicative of symptoms of insomnia. In addition, 5-point improvements in ISI scores may be clinically significant as these improvements may result in better mood, sleep, and overall well-being.31,32
Wrist Actigraphy
The Wrist Actigraphy (WA) device is similar to a wristwatch and is usually worn on the nondominant wrist. Wake and sleep patterns are inferred, based on the presence or absence of limb movements. The WA detects this motion by using a piezoelectric transducer. WA is used in many studies to evaluate: (1) Sleep Latency (SL); (2) wake-after-sleep onset; (3) Total Sleep Time (TST); (4) Sleep Efficiency (SE); and (5) naps. Using polysomnography as the gold standard, the WA has been successfully validated among subjects with insomnia on a number of important sleep measures including TST (r=0.70, p=0.01); SE (r=0.43, p=0.01), wake-after-sleep onset (r=0.48, p=0.01), and number of midsleep awakenings (r=0.49, p=0.01). 33 Sleep measurements that indicate decreased TST and SE and increased SL are often used clinically to suggest poorer sleep quality. Clinical interventions that decrease sleep-onset latency or increase TST by 30 minutes may be considered clinically significant, 34 as these changes may result in improved sleep and overall well-being.
Demographic Questionnaire
A demographic questionnaire developed by the research team was used to collect information on potential confounding variables.
Satisfaction Survey
The research team developed a satisfaction survey with several key questions extrapolated from the Veterans Health Administration (VHA) Survey of Healthcare Experiences of Patients (SHEP) ambulatory-care satisfaction survey. Modifications to the survey were made based on the War Related Illness and Injury Study Center's clinical experience with the group acupuncture protocol and the need to condense the satisfaction survey to minimize respondent burden. The SHEP survey has been used widely throughout the VHA to measure veteran satisfaction and is based on the Picker patient satisfaction survey, which was developed for the general patient population. 35 Cronbach's αs range from 0.59 to 0.81 for inpatient dimensions and from 0.35 to 0.89 for outpatient surveys. 35 Veteran satisfaction ranges of 77%–80% with overall satisfaction as Very Good or Excellent are considered to be clinically significant, as these ranges represent the VA's satisfaction target ranges for ambulatory care. 36
Study outcome data were collected during three timepoints: baseline (time [t]=0 months), midintervention (t=1 month), and postintervention (t=2 months). These timepoints were selected, based on consultation with CAM researchers, a review of the acupuncture literature,37–40 and empirical evidence from the War Related Illness and Injury Study Center's acupuncture clinical program.
After completing the baseline evaluation, veterans were randomized to one of three treatment groups, using a computer-generated randomizer table. Because this was a pilot study, the research team was generally only able to conduct study groups 2 days per week. As a result, participants were randomized into two treatment groups at a time (i.e., first true acupuncture versus the wait-list control, then sham acupuncture versus the wait list control, then true acupuncture versus sham acupuncture). This was a single-blinded study in which participants were blinded to the true auricular acupuncture protocol versus the sham auricular acupuncture protocol. The study coordinator and treating acupuncturist were not blinded to the intervention; however, quality-assurance protocols were in place to minimize this bias.
Statistical Analyses
Statistical analyses were conducted using SAS 9.2. Baseline characteristics were compared using an analysis of variance (ANOVA) for continuous variables and a χ2 test for association of categorical variables to confirm that randomization resulted in three homogenous study groups. Differences in changes over t between treatment groups were assessed by examining the group×t interaction term in a repeated-measures ANOVA. Tukey's method was used to adjust for multiple comparisons. The interaction effect size was indicated by the % of total within-group variance accounted for by the interaction. This was computed by SSinteraction/SSerror. A group×t interaction accounting for 10% of total variance can be considered to be clinically meaningful. Because this was a pilot study, significance levels of p≤0.20 were considered as trends that should be followed up with further study, while those of p≤0.05 were considered as likely to be true positives.
Results
Figure 4 outlines the flow of study participants from recruitment through group assignment to study completion. The primary reasons for dropping out once being randomized were job schedules, family commitments, school commitments, and lack of interest. One veteran discontinued the study before receiving any treatment because of an exacerbation of PTSD symptoms. Of those who did receive the allocated intervention, only 2 subjects did not complete the study (1 developed an exclusionary criteria and the other veteran felt that the acupuncture needles were uncomfortable.)
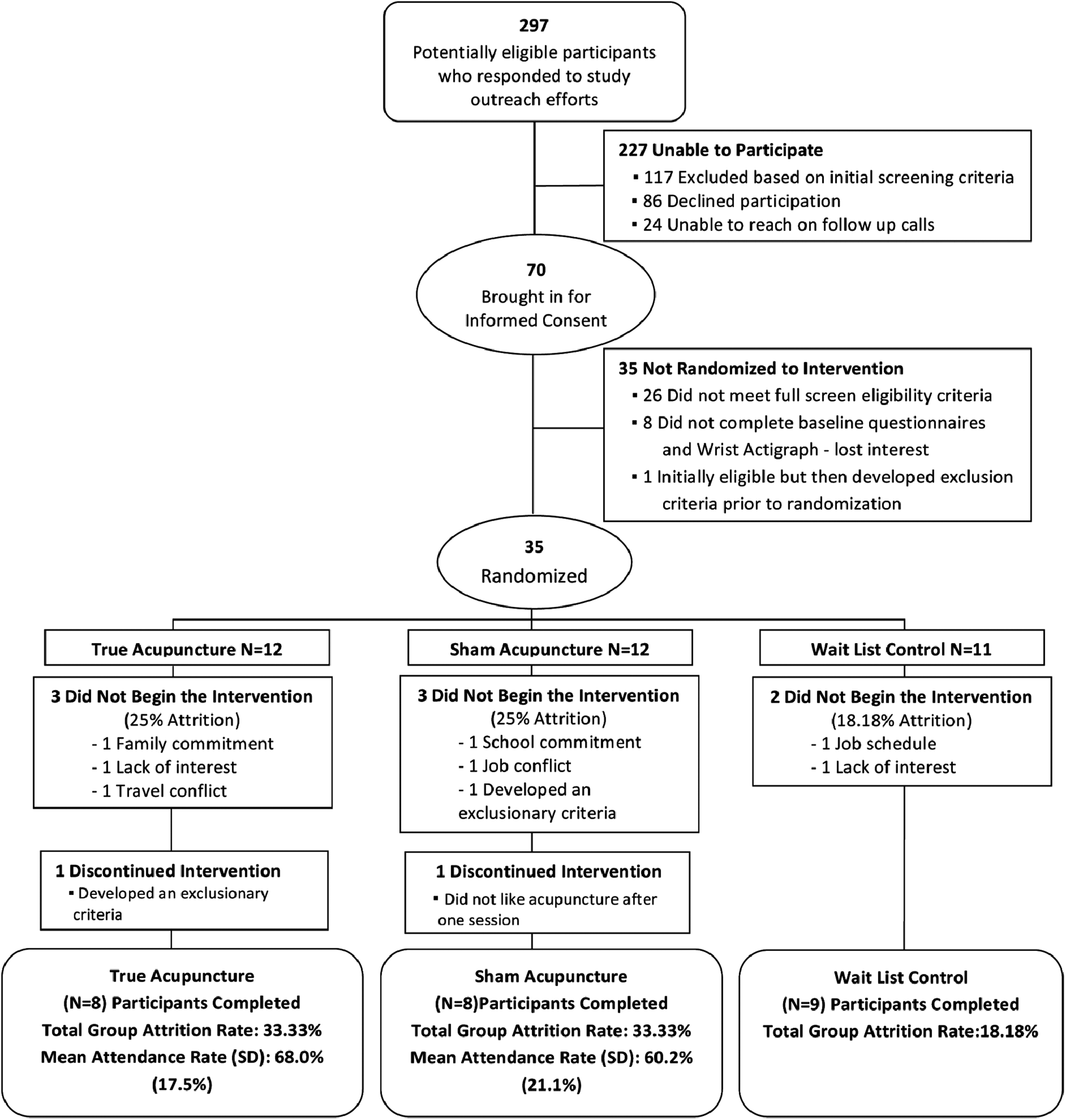
Study participants flow diagram SD, standard deviation.
Baseline characteristics for each of the three groups are outlined in Tables 4 and 5. There were no statistically significant associations at baseline, indicating that randomization created roughly equivalent groups. Table 4 lists the p-values for all of the baseline demographic variables analyzed for each of the three groups.
Chi-square test for association, p≤0.20.
avg, average; COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease.
SD, standard deviation; PCL-M, PTSD checklist—military version; PTSD, post-traumatic stress disorder.
Outcomes and Estimation
Using intent-to-treat analyses, the research team analyzed the results of group assignment on outcome variables. Table 6 shows effect sizes and significance of group×t interaction for the outcome variables for Research Question 1. MSD TST was significant (p=0.0195), with 29% of the variance explained by group assignment. MSD SE and naps trended toward significance, with small-to-moderate effect sizes. Perceived sleep quality, measured by MSD refreshness rating and ISI total score, also trended toward significance.
n=23 for WA.
†p≤0.05; ‡p≤0.20.
MSD, Morin Sleep Diary; ISI, Insomnia Severity Index; TST, Total Sleep Time; SL, Sleep Latency; SE, Sleep Efficiency, WA, Wrist Actigraph.
Table 7 outlines the group differences in mean outcomes at each timepoint. The breakdown of participants by group at each timepoint was as follows:
ANOVA values shown in italics.
n=23 in WA.
Between–group means statistically significant, p≤0.05
†Between–group means statistically different, p≤0.20
ANOVA, analyse of variance; CI, confidence interval; ISI, Insomnia Severity Index; TST, Total Sleep Time; MSD, Morin Sleep Diary; WA, Wrist Actigraph; SL, Sleep Latency; SE, Sleep Efficiency.
(1) Baseline—12 participants in the true auricular acupuncture group, 12 participants in the sham auricular acupuncture group, and 11 participants in the control group
(2) 1 month—9 participants in the true auricular acupuncture group, 8 participants in the sham auricular acupuncture group, and 9 participants in the control group
(3) 2 months—8 participants in the true auricular acupuncture group, 8 participants in the sham auricular acupuncture group, and 9 participants in the control group.
With respect to perceived sleep quality, the true auricular acupuncture group had a statistically significant improvement (p=0.0165) as measured by ISI at t=1 month and had a significant group×t interaction. The true auricular acupuncture group had a trend toward lower MSD TST at t=2 months (p=0.078), compared to the other two groups. The true auricular acupuncture group also had a trend toward lower WA TST at t=1 month (p=0.0893), compared to the other two groups. The true auricular acupuncture group had a trend toward higher MSD nap times than the other two groups post-treatment (p=0.0666). This higher nap t was also corroborated by the WA for the true auricular acupuncture group, compared to the other two groups; however, the group×interaction effect was not statistically significant. Figures 5–9 illustrate mean values with 95% confidence intervals (CIs) for the outcome variables. Table 8 shows that there was no statistically significant association between group assignment and change in hypnotic medication status.

Baseline, 1 month, and 2 month means with 95% confidence intervals for ISI total score. ISI, Insomnia Severity Index
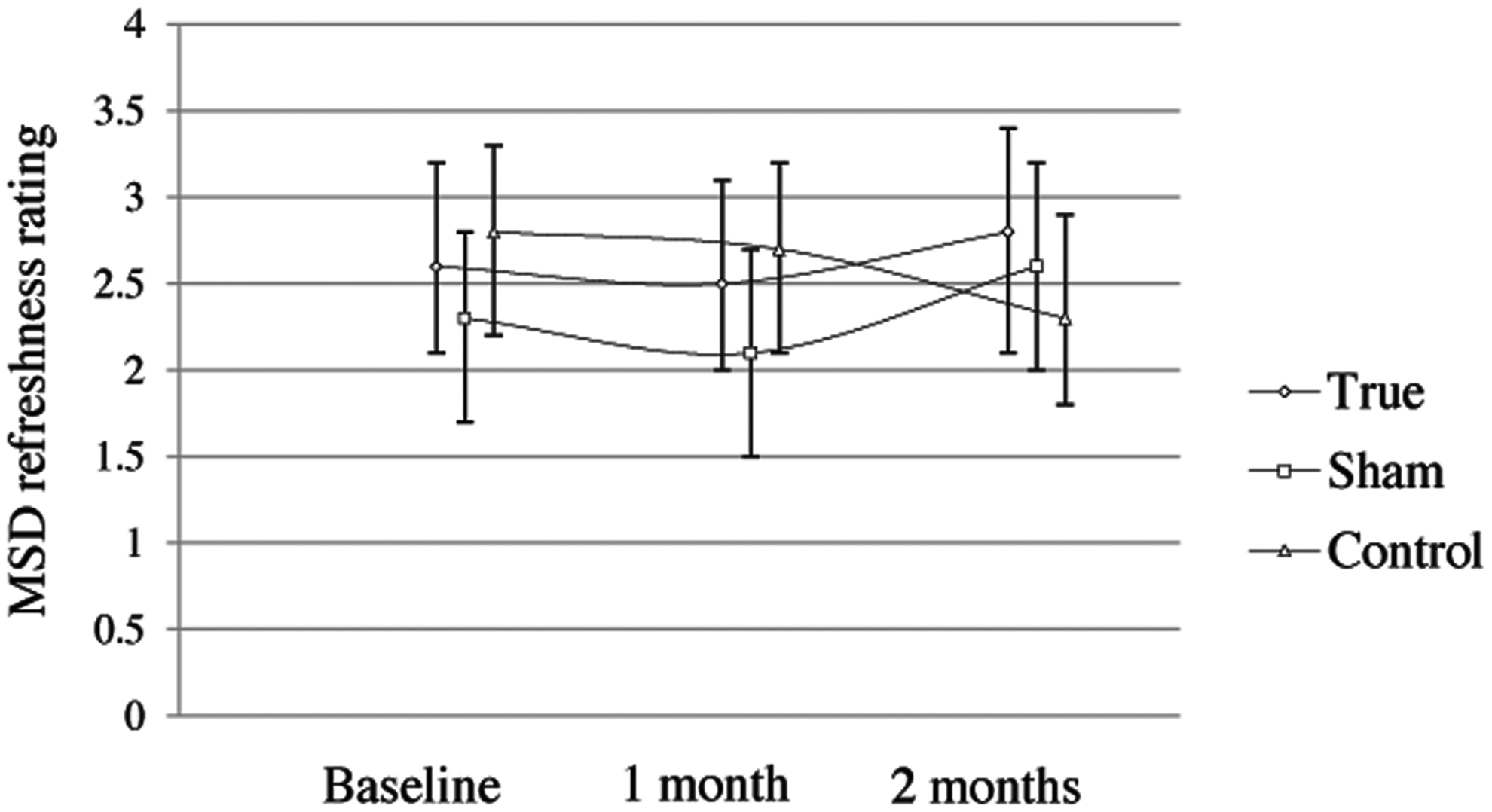
Baseline, 1 month, and 2 month means with 95% confidence intervals for MSD refreshness rating. MSD, Morin Sleep Diary.
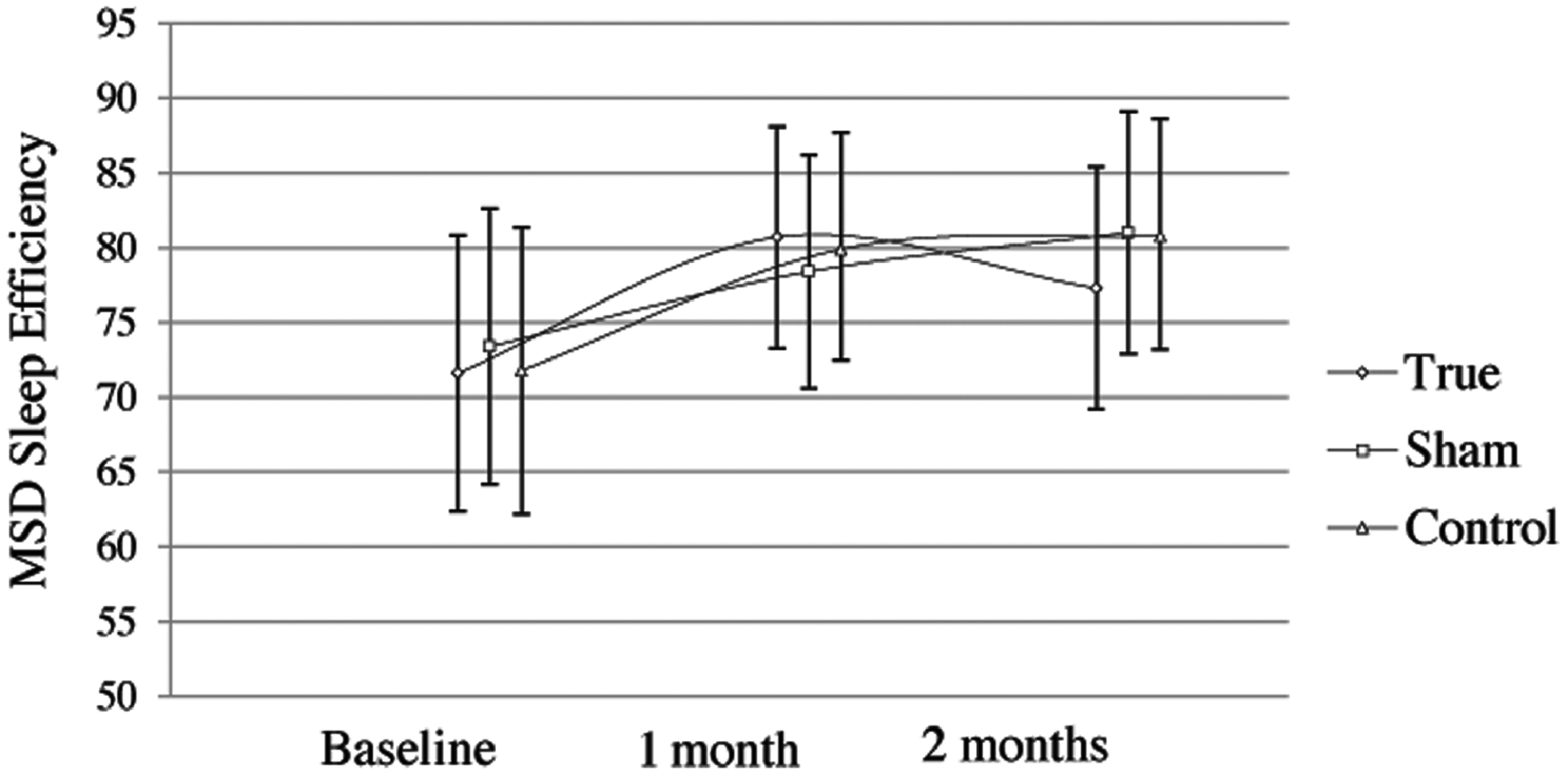
Baseline, 1 month, and 2 month means with 95% confidence intervals for MSD Sleep Efficiency. MSD, Morin Sleep Diary.
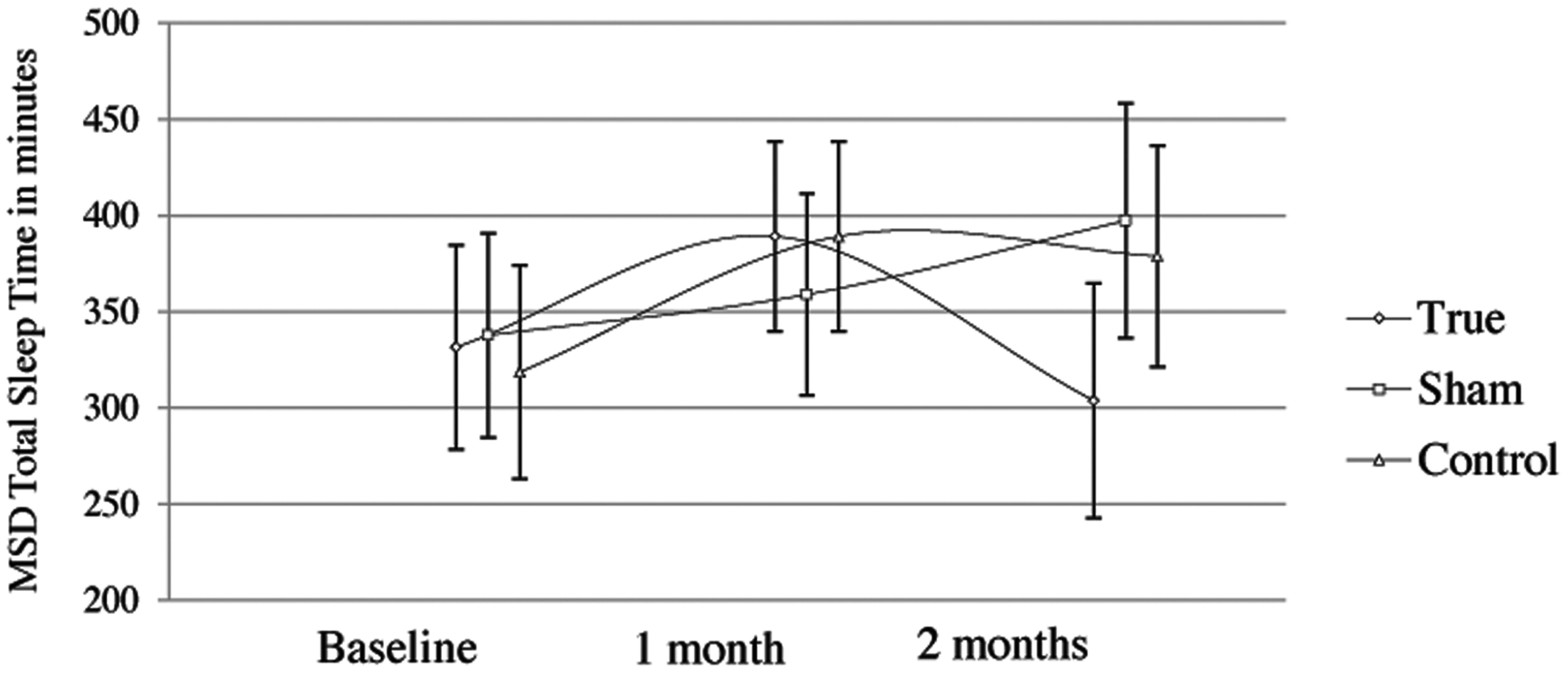
Baseline, 1 month, and 2 month means with 95% confidence intervals for MSD Total Sleep Time in minutes. MSD, Morin Sleep Diary.

Baseline, 1 month, and 2 month means with 95% confidence intervals for MSD daily nap time in minutes. MSD, Morin Sleep Diary.
The research team looked at the correlation between objective and subjective measures of sleep. Correlation coefficients for the MSD and WA scores for TST, SL, SE, and naps are outlined in Table 9. Modest, statistically significant correlation coefficients were noted for MSD TST and WA TST at t=2 months (p=0.0091), and MSD naps and WA naps at baseline (p=0.0153) and t=2 months (p=0.0236).
p≤0.05; †p≤0.20
MSD, Morin Sleep Diary; WA, Wrist Actigraph; TST, Total Sleep Time; SL, Sleep Latency; SE, Sleep Efficiency.
Veteran acceptance was measured through analysis of satisfaction scores and attrition rates. With respect to satisfaction scores, the researchers looked at several variables (i.e., confidence and trust in the acupuncturist, courtesy of acupuncturist, quality of the intervention, if acupuncture addressed the veteran's main concern, the veteran's willingness to recommend acupuncture to a friend, and the veteran's willingness to try acupuncture again). These satisfaction surveys were completed by true auricular acupuncture and sham auricular acupuncture participants at 1 and at 2 months (Table 10). Veterans in both groups expressed overall satisfaction with the intervention, and a high percentage of the participants stated that they would recommend acupuncture and try it again. A χ2 test for association showed no statistically significant differences between the two groups in terms of satisfaction ratings.
To examine attrition rates, attendance rates were compared between the sham auricular acupuncture and true auricular acupuncture groups at 1 and at 2 months. At 1 month, the true auricular acupuncture group attended an average of 75.0% (95% CI 59.8–90.2) of the sessions, while the sham auricular acupuncture group attended an average of 57.8% (95% CI 38.5–77.1) of the sessions (Table 11). This difference approached statistical significance (F=2.738, p=0.119). There was no statistically significant difference in attendance rates of total sessions attended at 2 months.
SD, standard deviation.
Adverse Effects
One veteran in the sham auricular acupuncture group reported that the needling was uncomfortable and requested withdrawal from the study. No other adverse effects were reported by the participants.
Discussion
To the authors' knowledge, this is the first RCT that examined the effect of group auricular acupuncture on PTSD-related insomnia. Veterans reported significantly improved perceived sleep quality, as measured by ISI, compared to the sham auricular acupuncture and wait-list control groups, after 1 month of acupuncture with a moderate effect size. With respect to group×t interaction, another perceived sleep quality variable (MSD refreshness ratings) trended toward significance. This result is supported by literature that suggests that acupuncture may influence sleep quality perceptions positively. 41 It is reasonable that, with a larger sample, this variable may have resulted in significant findings.
While the positive findings on perceived sleep quality are encouraging, this study did not demonstrate that group auricular acupuncture improved scores on MSD or WA measures for TST, SE, and naps for this cohort of veterans. When looking at the objective sleep data, the research team noted that WA TST decreased at t=1 month, compared to baseline, and then returned closer to baseline at t=2 months in the true auricular acupuncture group. The results also indicate that the true auricular acupuncture group had significantly more objectively measured naps at t=2 months, compared to the other two groups. This may have occurred for several reasons. First, it is possible that increased napping may be a positive effect of acupuncture, while at the same time, affecting TST negatively. The research team postulated that veterans in the true auricular acupuncture group may have been more relaxed during the acupuncture sessions and, hence, were more prone to napping. However, a χ2 test for association showed no statistically significant difference between true auricular acupuncture and sham auricular acupuncture groups in session nap time. In addition, the research team looked at cumulative sleep times (CST: combining naps and TST) for each of the three groups to determine if increased naps for the true auricular acupuncture group may have resulted in increased overall CST and thus may have played in a role in the increased sleep quality perceptions reported by the true auricular acupuncture group. Figure 10 shows the mean CST for each group, as measured by MSD, and found that the group×t interaction for CST had an effect size of 0.17, which trended toward statistical significance (p=0.1242). CST, as measured by WA, did not have a statistically significant group×t interaction. While veterans in the true auricular acupuncture group napped more, they did not have higher CST than the other two groups. Given that it is common clinical practice to educate patients with insomnia about sleep-hygiene practices (e.g., refraining from daytime naps because of interference with night-time sleep), a take-home lesson from this pilot study may be that acupuncturists should incorporate sleep-hygiene education into their clinical practices.

Baseline, 1 month, and 2 month means with 95% confidence intervals for MSD Cumulative Sleep Time. MSD, Morin Sleep Diary.
Second, sample-related factors may have contributed to the lack of positive findings for the TST, SE, and naps outcome variables. One veteran in the true auricular acupuncture group had very fragmented sleep patterns on both the MSD and the WA with large standard deviations. These were difficult to interpret and, given the small sample size of this study, this may have affected the results.
Third, this was a standardized group intervention, and some researchers have suggested that acupuncture may work best when it is tailored to individual health concerns. 42
Fourth, given the pilot nature of this study, the authors were not able to quantify the amount of conventional care treatment that veterans received. There may have been variability in conventional care treatment that affected the study outcomes (i.e., degree of individual or group counseling).
Finally, it is important to note sample-size limitations. Our initial power analysis determined that a minimum sample size of 20 veterans per treatment group was needed to achieve an 80% chance of detecting an effect size of 0.24–0.34 significance at the 0.05 level using a 2-tailed F test. This study did not achieve that desired sample size given some of the recruitment issues mentioned earlier. As a result, interpretation of the study results was limited.
This study also corroborated the finding that subjective and objective sleep measures often do not show high levels of correlation.43–45 In fact at the t=1 month measurement, the true auricular acupuncture group reported significantly less insomnia severity (as measured by the ISI), while, at the same time, that group had the lowest objectively measured TST. This brings into question certain assumptions when treating clinical patients. Because TST may not necessarily correlate with perceptions of sleep quality, it is important for clinicians to address sleep perceptions as well as sleep quantity when working with veterans with insomnia. It is also possible that perceived sleep quality may be influenced by what sleep stage is reached and for how long, and that this may have been improved by acupuncture. If this is the case, measurement of sleep quantity via wrist movement (WA) would not be expected to offer insight into this or correlate with perceived sleep-quality rating reports.
Another factor that may have played a role in the discrepancies between sleep diaries and WA data is the suggestion that analyzing sleep diaries and WAs in the PTSD population can be difficult, given the complicated sleep patterns that many patients with PTSD experience.46–48 Given these difficulties, it is not surprising that some of the participants may have found it difficult to record their sleep accurately. In this study, several participants had numerous wakings that made it difficult at times to interpret the MSD and WA data. This was complicated further by the facts that some of the MSD information was illegible, missing, or poorly documented; some of the WA data showed that the WA was taken off at times; and participants slept with the lights on. The research team had to make follow-up calls for clarification on the above results, and information obtained through these telephone calls may have been influenced by recall limitations.
With respect to veteran satisfaction, both the true auricular acupuncture and sham auricular acupuncture groups scored high on a number of satisfaction variables. While there was no statistically significant difference between the two groups, the true auricular acupuncture participants did report higher acupuncture quality, stated that they felt that the auricular acupuncture addressed their main health concerns more completely, and were more willing to try acupuncture again. With a larger sample size, these findings may have trended toward significance. With respect to attrition rates, a considerable number of veterans expressed interest in acupuncture (Fig. 4). However, this pilot study was unable to accommodate the scheduling needs of many interested veterans. Although groups were conducted at times deemed most preferred on an informal survey, (late afternoon, weekdays were most preferred), there were still a considerable number of veterans who preferred other times and who were thus unable to participate in the study. In addition, this was a one-site study, and, as a result, some interested veterans were unable to travel to an urban medical center because of work conflicts, traffic patterns, and family commitments. However, once veterans were allocated to the intervention and started receiving the treatments, the attrition rate was low with only 2 veterans not completing the study. Attendance rates for the 16 study sessions were slightly higher for the true auricular acupuncture group, with a mean attendance rate of 68%, compared to 60.2% for the sham auricular acupuncture group (Fig. 4).
As illustrated, the effect sizes noted in this study were mostly small-to-moderate. These effect sizes may be of assistance to researchers conducting future studies in terms of sample-size calculations. Most importantly, effect sizes that trended toward significance may warrant further exploration.
Conclusions
Veterans with PTSD–related insomnia who received true auricular acupuncture reported higher perceived sleep quality at t=1 month, compared to participants in the sham auricular acupuncture and wait-list control groups. True auricular acupuncture did not produce improvements in TST and naps, as measured by the MSD and WA. Instead, true auricular acupuncture participants had lower TST scores and more naps, as measured by both the MSD and WA, compared to participants in the sham auricular acupuncture and wait-list groups. A clinical recommendation from this study may be for acupuncturists to incorporate sleep hygiene education into their clinical practices and/or collaborate with insomnia health care professionals when working with individuals with insomnia. This study supports further the finding that subjective sleep quality measures and objective WA measurements often are not significantly correlated. It is important that researchers and clinicians address both sleep perceptions and collect objective sleep data when addressing insomnia in veterans. Satisfaction scores for participants in both the true auricular acupuncture and sham auricular acupuncture groups were high. While there was no statistically significant difference between the two groups' scores, veterans who received the true acupuncture reported higher acupuncture quality and felt that the acupuncture did a better job at addressing their main health concerns. With a larger sample size, some of the trends identified in this study may have resulted in significant findings.
Footnotes
Disclosure Statement
No competing financial interests exist.
*
Published by the American Psychiatric Association in Washington, DC, 2000.