
Abstract
Abstract
Background:
While the potential efficacy of EA has been investigated from a stimulation duration perspective, few studies have attempted to determine if blood flow responses differ with the sites of EA stimulation on human subjects.
Objective:
The aim of this research was to determine if blood-flow responses differed with sites of electroacupuncture (EA) stimulation in human subjects.
Methods:
Forty male students were divided into four groups (n = 10 in each group). Subjects in each group had EA at four different muscles: (1) upper trapezius; (2) lower erector spinae; (3) rectus femoris; and (4) gastrocnemius. EA stimulation was administered for 5 minutes. Changes in the skin temperature (ST), skin blood flow (SBF), and muscle blood volume (MBV) were measured before and after EA stimulation of the four different muscles.
Results:
MBV was increased significantly, compared with baseline in all 4 groups. ST and SBF responses, however, varied depending on the stimulation sites.
Conclusions:
EA administered to different muscles did not show differences in the MBV responses.
Introduction
A
The complex mechanisms behind acupuncture analgesia involve both central and peripheral effects. An increasing number of neuroimaging studies over the last few years have applied functional magnetic resonance imaging to investigate the brain's response to acupuncture stimulation.5–7 Previous studies have indicated that acupuncture could modulate the activity in multiple cortical and subcortical brain areas (i.e., brainstem, cerebellum, and limbic areas). 8 The pain-reduction effects of acupuncture could also be related to poststimulation augmentation of local blood flow, which can lead to an accelerating washout of analgesic substances. The local blood flow response after acupuncture is often considered to be induced by afferent input in somatic nerve fibers and to elicit spinal and supraspinal reflexes via A-delta and unmyelinated C-fibers. 9
It has also been suggested that regional skin and/or muscle blood flow increase in response to manual acupuncture and that EA involves cutaneous vasodilation caused by elevation of nitric oxide levels, 10 calcitonin gene–related peptide release from sensory nerve fibers via the axon reflex,11,12 and elevation of arterial blood pressure. 13
In a clinical and experimental study, Donoyama and Ohkoshi 14 reported efficacy of 15 minutes of EA application (50 Hz) on relieving symptoms related to Raynaud's phenomenon. The current authors previously reported that EA elevated skin temperature (ST) and increased muscle blood volume (MBV). 15 In that study, MBV changes were estimated before and after EA stimuli using near-infrared spectroscopy (NIRS) and a hydrogen clearance method (HCM). It was confirmed that both methods, NIRS and HCM, were useful for MBV estimation. However, there was a concern that the invasive needle electrode used for the HCM might have acted as a stimulus and modified MBV response. NIRS, however, can be used to estimate MBV noninvasively, thus the current authors consider that NIRS is less of a concern and more suitable for acupuncture experiments.
In another study, 16 the current authors also examined the effects of different durations of EA stimulation on blood flow. MBV had increases in 5-, 10-, and 15-minute EA duration groups in comparison to baseline. However, skin blood flow (SBF) yielded increases in 5- and 10-minute groups in comparison to baseline and there were no significant differences among the groups. Based on those findings, the current authors suggest that 10 minutes of EA stimulation could be a sufficient duration to induce a blood flow response when increasing blood flow is clinically desirable. This finding was supported by a clinical study demonstrating that a 10-minute EA treatment reduced pulse rate; relieved shoulder, low-back, and knee pain; and decreased natural-killer cell activity in older adults. 17
While the potential efficacy of EA has been investigated from a stimulation duration perspective, few studies have attempted to determine if blood flow responses differ with sites of EA stimulation in human subjects. This study was conducted, therefore, to examine the possible difference in muscle blood flow response after administration of EA to 4 stimulation sites.
Materials and Methods
Subjects
Healthy male students (N = 40, average age 23.5 ± 0.8 years old) were divided into 4 groups, each containing 10 subjects, using an envelope-allocation method. Subjects in groups A to D received EA at four different muscle groups, depending on their group assignments as follows: (1) Group A, upper trapezius; (2) Group B, lower erector spinae; (3) Group C, rectus femoris, and (4) Group D, gastrocnemius.
This study adhered strictly to the principles of the Declaration of Helsinki. 18 Before the study began, the participants were told about the purpose and procedures of the study, and all participants signed consent forms. This study was approved by the institutional review board of the Tsukuba University of Technology, Tsukuba, Japan. The experiments were conducted in a room with the temperature set at 25.0 ± 0.5°C and at 50.0 ± 5.0% humidity throughout the experimental sessions.
Stimulation Method
Two disposable acupuncture needles (40 mm in length and 0.20 mm in diameter, Seirin Co., Ltd., Shizuoka, Japan) were inserted at a depth of 10–15 mm into two acupuncture points. The stimulation sites used in each group are shown Figure 1 and in Table 1. An Ohm Pulser LFP-4000A (Zen Iryoki, Fukuoka, Japan) was used as the device for creating the EA stimulus. EA stimulation (1 Hz, waveform/square) was then administered for 5 minutes. The intensity of stimulation was adjusted so that muscle-twitching contractions were elicited in the targeted muscles without causing pain or discomfort to the subjects.
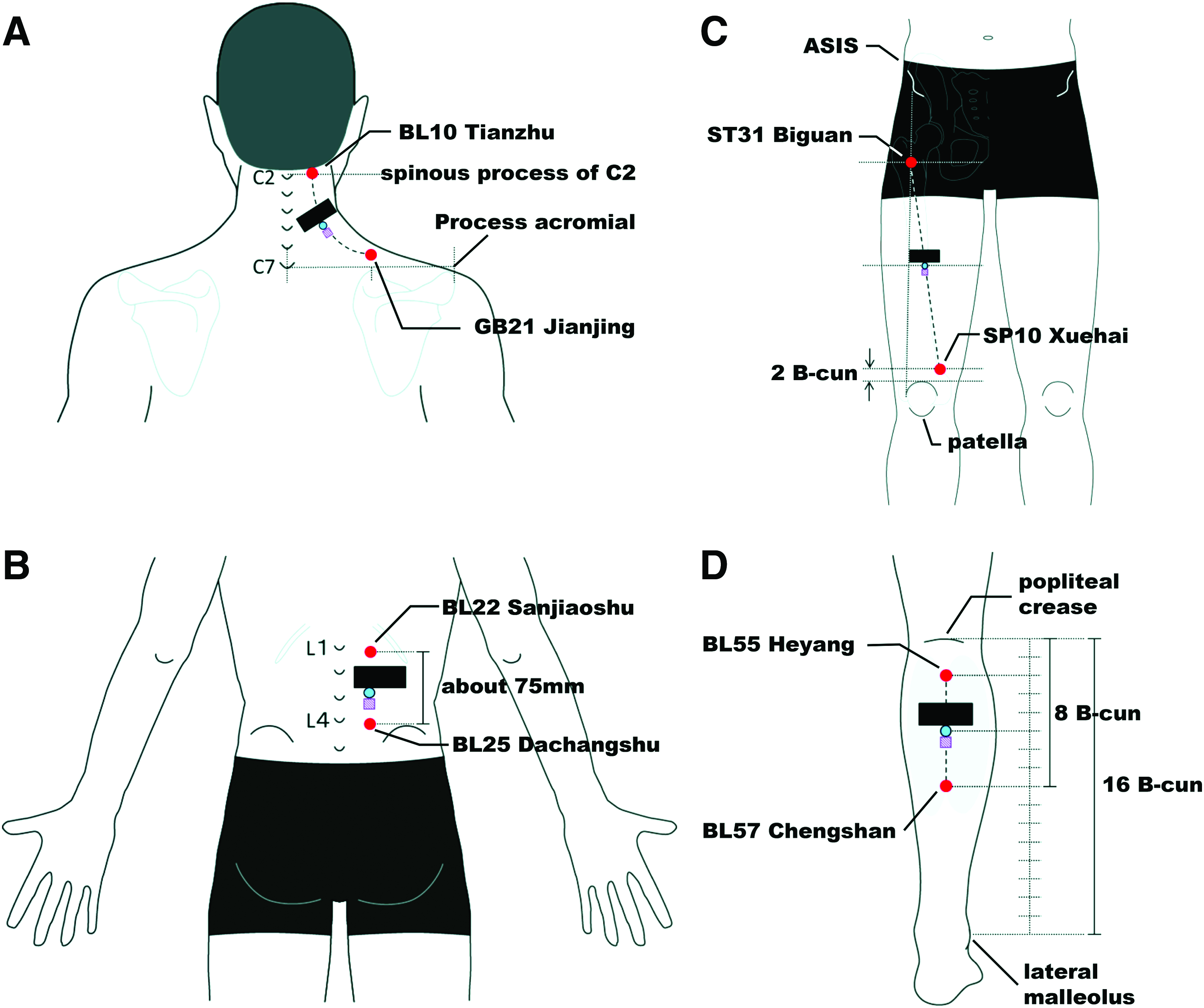
Stimulation and measurement sites used in each group.
EA, electroacupuncture.
Measurements
Measurement of ST. A thermograph (JTG-5310, JEOL Ltd., Tokyo, Japan) was used to measure ST. Subjects in groups A, B, and C were asked to lie on the table in a prone position. Subjects in Group D were asked to lie on the table in a supine position. In order to analyze ST, four arbitrary frames were made on each EA site, just inferior to the SBF measurement probe.
Measurement of SBF. SBF was estimated by using a change in the laser Doppler signal (ALF 21D; Advance Co., Tokyo, Japan). The surface electrodes (10-mm diameter) were placed with special double-stick tape at the midpoint between the two EA-stimulating sites.
Measurement of MBV. Prior to the main experiment, a preliminary study 15 was conducted to compare two commonly used methods of estimating MBV: (1) the NIRS method, which is noninvasive; and (2) the HCM, which is invasive. Based on the data from that pilot study, 15 the NIRS method was chosen for the current study, because NIRS is noninvasive and would be less stressful for the subjects. NIRS has been used noninvasively to measure local skeletal muscle deoxygenation and to estimate regional muscle blood flow. 19 For the MBV estimation via NIRS, surface electrodes (20 × 50–mm dimensions) were attached superior to the SBF probe with the special double-stick tape.
The locations of the electrodes and EA sites are shown in Figure 1 and Table 1.
Experimental Procedure
Baseline ST, SBF, and MBV were recorded following a 15-minute rest period just prior to the intervention period (Pre). ST, SBF, and MBV were estimated also for the following time periods: 3 minutes after the initiation of EA (Stim 3); immediately following EA (Post 0); and at 5 (Post 5), 10 (Post 10), 15 (Post 15), 20 (Post 20), 25 (Post 25), and 30 (Post 30) minutes afterward.
Statistical Analysis
Serial changes in ST, SBF, and MBV among the groups were analyzed using a mixed-model two-way analysis of variance (ANOVA) and Fisher's Least Significant Difference (LSD) multiple comparison test. Serial changes in each group were analyzed using a mixed model one-way ANOVA and Fisher's LSD multiple comparison test. SPSS Advanced Models, version 15, software was used for the statistical analysis. The level of significance was set at P < 0.05. The values generated were mean ± standard error.
Results
ST, SBF, and MBV responses are summarized in Figure 2 and Table 2.

The change in the skin temperature (ST), the skin blood flow (SBF), and the muscle blood volume (MBV) with electroacupuncture (EA) stimulation on the four muscles (See key at the end of this figure legend). The baselines of the ST, SBF, and MBV were recorded (Pre); 3 minutes after the start of EA (Stim 3); immediately after EA (Post 0); and at 5 (Post 5), 10 (Post 10), 15 (Post 15), 20 (Post 20), 25 (Post 25), and 30 (Post 30) minutes afterward. The level of significance was set at P < 0.05. The values presented were mean ± standard error. Key: ■, Group A (upper trapezius); ●, Group B (lower erector spinae); ▲, Group C (rectus femoris); ♦, Group D (gastrocnemius). Color images available online at www.liebertpub.com/acu
Change in ST, SBF, and MBV with EA stimulation on the four muscles (A–D). Baselines of the ST, SBF, and MBV were recorded at (Pre); 3 minutes after the start of EA (Stim 3); immediately after EA (Post 0); and at 5 (Post 5), 10 (Post 10), 15 (Post 15), 20 (Post 20), 25 (Post 25), and 30 (Post 30) minutes afterward.
Muscle groups are as follows: A, upper trapezius; B, lower erector spinae; C, quadriceps femoris; and D, gastrocnemis.
The level of significance was set at P < 0.05. *Indicates statistical significance. The values presented are mean ± standard error.
ST, skin temperature, SBF, skin blood flow, MBV, muscle blood volume, EA, electroacupuncture.
Skin Temperature
In Groups A, B, and C, ST increased significantly after EA at all measurement timepoints. In Groups A and B, ST also increased during the EA. In Group D, no significant ST change occurred after EA. No significant difference existed in the serial changes among the groups.
Skin Blood Flow
In Group B, SBF increased significantly at Post 5 and Post 10. Groups A, C, and D did not show any significant difference in SBF after EA stimulation. No significant differences existed in the serial changes among the groups.
Muscle Blood Volume
In Groups B, and D, MBV increased significantly after EA at all timepoints.
In Group A, MBV significantly increased at Post 15, Post 20, Post 25, and Post 30, while Group C showed significant MBV increases at Post 5, Post 10, Post 15, Post 20, Post 25, and Post 30.
No significant differences existed among the groups in the serial changes.
Discussion
Changes in ST, SBF, and MBV (measured before and after EA stimulation) were compared on four different muscles. MBV increased significantly, compared with baseline in all 4 groups.
Previous studies in rats 20 and humans 16 have shown that varying lengths of time of EA stimulation did not result in different SBF or MBV responses. A study by Mori et al. (the current authors), 16 in particular, demonstrated that while SBF increased following 10 minutes of EA stimulation, there were no significant differences in MBV responses according to different durations of EA stimulation.
In the current study, all groups with different stimulation sites showed significant MBV increases following EA stimulation. These results suggest that EA stimulation may increase MBV regardless of sites of EA administration.
The ST and SBF responses, however, varied depending on the stimulation sites.
It is not known precisely why different responses in ST, SBF, and MBV emerged in the current study. However, the current authors hypothesize that the varied responses could be related to the targeted areas of EA stimulation, such as muscles, nerves, or skin.
For instance, Chen and Yu used acupuncture-like transcutaneous electrical nerve stimulation, targeting the skin, to treat atopic dermatitis. 21 Some EA treatment specifically targets nerves. Inoue et al. reported on EA administration directed to the spinal nerve root for relieving sciatica.22,23 The current authors suggest that the EA used in this study mainly affected the muscles. This could be why the most consistent blood-flow response was seen in the muscles, while an inconsistent response was seen in the skin.
It should be noted that only local blood-flow response was evaluated in this current study. However, acupuncture has been known to elicit responses away from stimulation points, including in visceral organs. 24 Thus the conclusions (see section below) drawn from the current study are not applicable to such systemic or distant acupuncture effects.
Conclusions
Changes in the ST, SBF, and MBV on four different muscles before and after the EA stimulation were compared. MBV increased significantly, compared with the baselines in all groups. ST and SBF responses, however, varied, depending on the stimulation sites. EA administered to different muscles did not produce differences in the MBV response. Further research is needed to investigate the mechanism of acupuncture for SBF and MBV responses, considering different stimulation targets including skin, muscles, and nerves.
Footnotes
Acknowledgment
This work was supported by the Tsukuba University of Technology, Projects for Advanced Education and Research.
Disclosure Statement
No competing financial interests exist.