
Abstract
Abstract
Background:
Aneurysmal subarachnoid hemorrhage (SAH) is a medical emergency characterized by extravasation of blood into the subarachnoid space after the rupture of a cerebral aneurysm and presents a high risk of complications and death.
Case:
A young patient (a previously healthy 32-year-old man) presented with SAH accompanied by a severe headache and vasospasm (as shown on a transcranial Doppler scan). The objective was to use integrative medicine to treat his SAH in an intensive care unit (ICU). Conventional and traditional Chinese Medicine (TCM) practices were used. The TCM treatment consisted of electroacupuncture (EA) in BL 2/TE 23 and BL 10/GB 20 at 2/100 Hz during his stay in the ICU.
Results:
EA inhibited the increase of blood flow speed in the middle cerebral and basilar artery and alleviated the patient's severe headache and vasospasm. Thus, among the possible mechanisms of EA that account for our results, we propose that its effects on humoral adjustment mechanisms and neurogenic factors contribute to modulation of the imbalance between the sympathetic and parasympathetic nervous system activities and thereby results in improved endothelial dysfunction and modulation of the cytokine profile and inflammatory mediators.
Conclusions:
The results achieved with this patient suggest that EA was able to reduce headache in addition to reducing cerebral blood flow speed with improvement in brain perfusion. Controlled prospective studies are required to reaffirm and consolidate EA as an important technique for addressing SAH.
Introduction
A
SAH can be diagnosed by computed tomography, magnetic resonance imaging (MRI), and evaluation of the cerebrospinal fluid, but these tests cannot detect the occurrence of vasospasm. Cerebral angiography is the gold standard test because it defines the location of the aneurysm and identifies vasospasm even when no clinical evidence is present,1,2 but this procedure is invasive and not devoid of risks. Therefore, the noninvasive nature of transcranial Doppler (TCD) makes it an attractive technique for confirming the clinical diagnosis of vasospasm and should be performed every 24 or 48 hours.1,4–6
The efficacy of medical treatments based on Traditional Chinese Medicine concepts has been increasingly recognized worldwide.7,8 Acupuncture has been used to relieve pain for >2000 years in Asian countries.8,9 Electroacupuncture (EA) is the electrical stimulation of acupoints with acupuncture needles through which a short current pulse is applied at various frequencies. 10 Experimental and clinical studies have demonstrated that the anti-inflammatory actions of acupuncture are mediated by central inhibition of the innate immune system as a result of vagal activity.9,11 This report presents a case of SAH in a young man with a severe headache and intracranial vasospasm (demonstrated by TCD) who benefited from treatment with EA during his stay in the intensive care unit (ICU) at the medical center of the Centro Hospitalar Unimed Joinville, Joinville, SC, Brazil.
Case
A previously healthy 32-year-old man was admitted to the hospital with a complaint of a holocranial headache. He was found unconscious on his bathroom floor with a cut in the frontal region of his head and was taken to the hospital. There was no previous history of head trauma or neck manipulation, no past medical or surgical history, and no use of medications or infectious symptoms. The patient was a nonsmoker, did not have diabetes mellitus, and was normotensive. There was no family history of thrombophilia or venous thromboembolism. On medical examination, he was noted to be conscious and oriented, presented 15 points on the Glasgow scale (GCS), and had no meningeal signs and no focal motor deficit. He had initial event amnesia (sudden loss of consciousness). The initial diagnosis was mild brain trauma and spontaneous SAH (Fig. 1). Neurologic evaluation showed Hunt-Hess I and Fischer III.

Brain computed tomography of subarachnoid hemorrhage on the left supracerebellar cistern.
On the third day, the patient was transferred to the ICU to be managed appropriately and to investigate the SAH. He remained at GCS 15, without motor deficit, clinically with a moderate-to-severe headache and mild neck stiffness. A TCD examination was performed and showed flow velocity in the anterior circulation within normal limits. However, flow speed increased in the basilar artery distal segment (73 cm/second) with a Soustiel index of 2.1, suggesting vasospasm in this segment. TCD was repeated every day, showing flow speeds and the Lindeggard index within normal limits for anterior circulation and stable and close-to-normal limits regarding vertebrobasilar circulation with a maximum Soustiel of 2.2. The sonographic diagnosis was mild vasospasm in the basilar artery, which was clinically asymptomatic.
A cerebral digital subtraction angiography (Seldinger technique via the right femoral artery) was performed on the fifth day and revealed a saccular aneurysm in the distal segment of the superior cerebellar artery with a typical aspect of an adissecting aneurysm (Fig. 2). Given that endovascular treatment was unsuccessful, occlusion of the immediately proximal vessel to the aneurysmal neck of the aneurysm was performed.
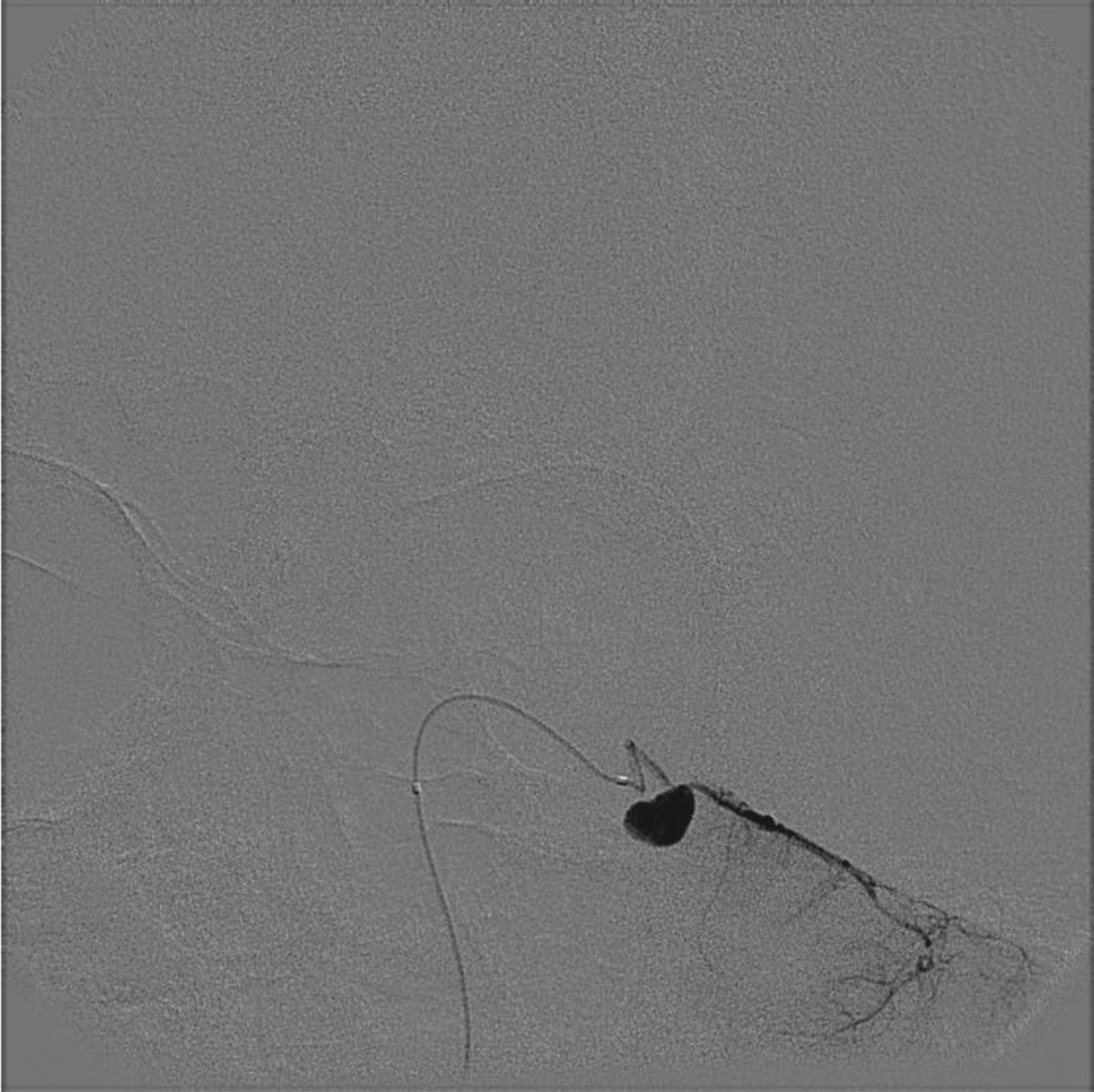
Preoperative angiography. Preoperative angiography showing the upper cerebellar artery aneurysm via micro catheter for superselective catheterization of the distal segment of the left superior cerebellar artery and the injection show the sacular image of the dissection aneurysm.
During his stay at the ICU, the patient complained of his severe headache, which was not responsive to fentanyl in a patient-controlled analgesia (PCA) regimen (40 mcg/hour with a bolus of 20 mcg) and presented with psychomotor agitation.
EA was started on the sixth day to help control the patient's severe headache. The procedure involved 30 minutes at points BL 2/TE 23 (ophthalmic and maxillary branches of the trigeminal nerve), and BL 10/GB 20 (C-1 and C-3 nerve roots) with 2/100 Hz at 4-second intervals (NKL530, Brusque/SC, Brazil, with DongBang 0.25 × 40 sterile needles). A TCD was performed before and 2 hours after the EA session to monitor the safety of the procedure. TCD data are shown in Figures 3 and 4.
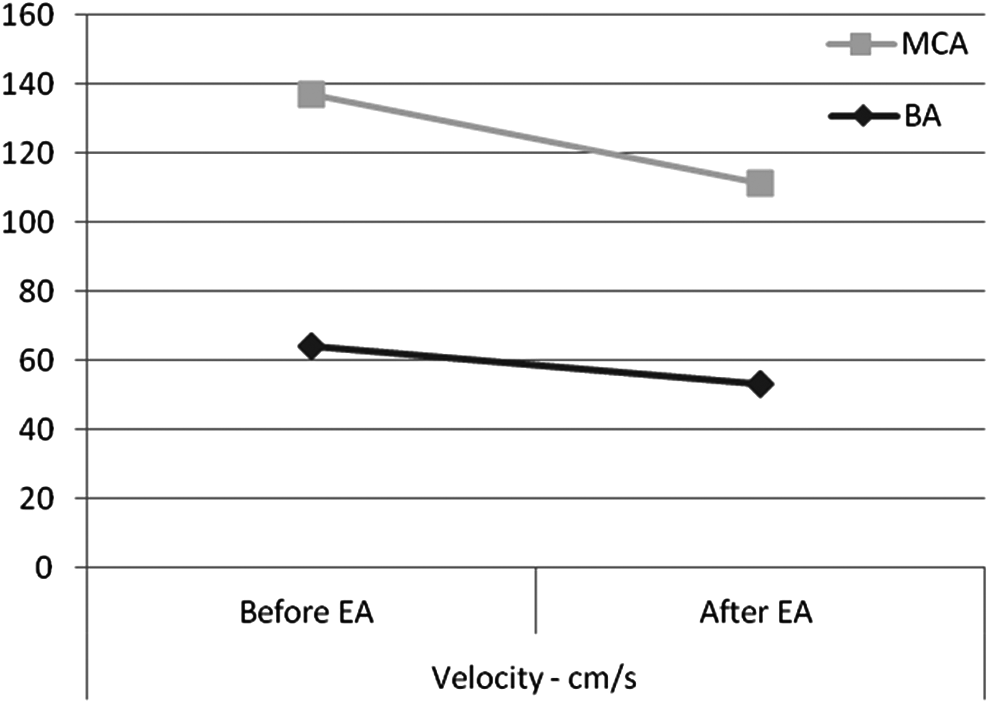
Transcranial Doppler data before and after EA in anterior and vertebrobasilar circulation. EA, electroacupuncture; MCA, middle cerebral artery; BA, basilar artery; s, second.

Lindeggard Index and Soustiel Index before and after EA. EA, electroacupuncture; BA, basilar artery; MCA, middle cerebral artery.
There was a significant reduction of the patient's headache after the procedure, which allowed him to sleep without agitation and PCA withdrawing 20 hours after EA, For the rest of his hospitalization the patient had rescue doses of opioids.
On the seventh day, MRI showed a hyperintense signal on T2 flair image sequences and restriction of concomitant diffusion in the left cerebellar hemisphere, suggesting a recent ischemic event on the left superior cerebellar artery territory without evidence of a mass effect or hemorrhagic transformation.
On the eighth day, the patient developed pain of moderate intensity and an additional session of EA was performed, which produced symptomatic improvement.
Results
EA inhibited blood flow speed increase in the middle cerebral and basilar arteries and alleviated the patient's severe headache and vasospasm. On the twelfth day, the patient left the ICU without any deficit and with adequate pain control. Four days later, the patient was discharged from the hospital without deficit and without a headache. He is currently being followed up in an outpatient clinic and does not present with any neurologic deficit. He carries on with his normal life.
Discussion
This article reported on the case of a young patient with SAH accompanied by a severe headache and vasospasm and treated with EA at points BL 2/TE 23 and BL 10/GB 20 with 2/100 Hz. EA alleviated his severe headache and vasospasm. Acupuncture has been used for centuries in East Asian countries to treat strokes, and confers neuroprotection. 12
As cerebral blood vessels are highly innervated by the autonomic nervous system to ensure blood flow autoregulation in various daily activities, 13 this could be the explanation for the benefic effects of EA. EA inhibits sympathetic activity, and this inhibition may last for more than 12 hours.13,14 Several mechanisms of action may account for this effect, including modulation of sympathetic activity in the raphe nucleus through opioid and serotonergic actions14–17 and an increase in expression of neuronal nitric oxide synthesis at the nucleus gracilis.9,18
In a case–control study, 20 patients diagnosed with SAH received manual acupuncture and had a significantly lower incidence of delayed ischemic neurologic deficit and significantly improved function at discharge, suggesting that acupuncture is effective for preventing cerebral vasospasm. 12
Researchers stimulated the acupuncture points ST 36 and PC 6, which are believed to improve endothelial dysfunction and decrease systemic inflammatory activity.19,20 In addition, the influence of the trigeminal sensory fibers in the cerebral blood flow has been demonstrated,21–23 justifying the points selected in this present case.
The concentration of P substance in pial vessels was reduced in cats who had their trigeminal ganglia removed, as well as when the ganglia from the C-1 to C-3 nerve roots were removed, 24 thus, showing the influence of these structures in the innervation of the meninges and pial vessels. 13 Transcranial electrical stimulation with 5 Hz in rats has increased the diameter of the middle meningeal artery by 119%. 25
Studies show increased cerebral blood flow in patients with ischemic cerebral vascular accident in volunteers 27 and in anesthetized rats after an acupuncture session.26,28 Furthermore, EA controls pain in clinical and surgical situations.10,29,30 The use of high- and low-frequency EA increases the concentration of dynorphin A, β-endorphin, and enkephalins.29,31,32 Low-frequency EA increases enkephalin release by 49% and dynorphin by 29%.32,33 According to Han, and Han and Sun, EA at 2/100 Hz in different parts of the body activated the k, δ, and μ opioid receptors to induce a synergistic analgesic effect, releasing opioid peptides.29,31 Thus, among the possible mechanisms of EA that account for the current results, the current authors propose that its effects on humoral adjustment mechanisms and neurogenic factors contribute to modulation of the imbalance between sympathetic and parasympathetic nervous system activities and thereby results in improved endothelial dysfunction and modulation of the cytokine profile and inflammatory mediators.
Conclusions
EA alleviated headache and reduced cerebral blood flow speed with probable improvement of cerebral perfusion in a SAH case. The mechanism involved in the treatment of vasospasm after SAH with EA appears to include modulation of the imbalance between vasodilatation and vasoconstriction in cerebral vessels, possibly through an effect of normalizing endothelial dysfunction. These findings might justify further studies to confirm the clinical applicability of EA and help to expand our understanding of the pathophysiology of SAH.
Footnotes
Author Disclosure Statement
No competing financial interests exist.