
Abstract
Abstract
Background:
Huang-Fu Mi's Jia Yi Jing (JYJ) is regarded as the earliest text (282 AD) on differential diagnosis and clinical acumoxa therapy in Chinese Medicine (CM).
Objective:
Within this Classical framework, this study examined CM clinical indications for the 20 Large Intestine (LI) channel points for evidence of possible sequence-associated patterns.
Materials and Methods:
The JYJ detailed the systematic definition and grouping of all acupoints termed “Ruling Points” (RPs) in relation to their unique patterns of signs and symptoms (“RP indications”), rather than as channel-specific lists. The JYJ includes comprehensive descriptions for RP indications for hundreds of clinical patterns for all channel acupoints, systematically categorized across six differential diagnostic books (Seven to Twelve). Two editions of the Zhen Jiu Jia Yi Jing (ZJJYJ) were scrutinized to identify all RPs for the LI channel sequence: the Song Dynasty Chinese edition (1077) and the English translation The Systematic Classic of Acupuncture and Moxibustion (1994) translated by Yang and Chace. RP indications for each acupoint were coded by ZJJYJ diagnostic Book and Chapter Part and examined for relationships between sequence position and diagnostic category of individual RP indications.
Results:
While no single category of CM indications based on the RP diagnostic system, was common to all 19 points, there were at least seven patterns involving clusters of RP indications associated with sequence positions. Most important were the first 7 acupoints together with LI 11. These contributed 49 of the 61 RPs channel points, with indications drawn from all six diagnostic Books. Overall, the RP indications for the channel focused primarily on the head and neck, as well as on generalized fever and upper-limb pain and weakness. The most frequent diagnostic indications for the channel came from diagnostic Book Twelve (head and neck) with 24 RPs being identified for 12 LI acupoints.
Conclusions:
The RP attributes and profiles for the sequence of LI points overall reflect a common clinical focus, while position effect concerns the breadth of the signs and symptoms addressed by individual acupoints. Awareness of relevant RPs from other channels could refine the differential diagnosis of complex clinical conditions and their CM treatments further.
Introduction
I
The JYJ's valuable contribution to practical application of channel-based differential diagnostics, which is still recognized in modern CM, stemmed from this systematic presentation of specific acupoints, termed “Ruling Points” (RPs) in relation to unique patterns of clinical signs and symptoms (“RP indications”), rather than as a simple channel-based list. The RP system is central to Mi's development of a detailed systematic treatise on differential diagnosis for acupuncture and moxibustion. The extent of detail and organization is impressive, with comprehensive descriptions for specific RPs from all channels for hundreds of clinical patterns, systematically and uniquely categorized across the 54 Parts of 48 Chapters in six differential diagnostic Books.
Over the centuries, successive editions of the text (henceforth denoted by ZJJYJ) became increasingly corrupted by introduced errors and distortions. This was addressed in the Song Dynasty by Royal decree with the publication in 1077 of an official restored version. 2 An electronic format of the Song Dynasty Chinese edition Zhen Jiu Jia Yi Jing (Song Dynasty 1077) manuscript was used in the present study. 3
Although the original theories on channel based acupuncture from Mi's time remain the central model in Chinese acupuncture today, surprisingly, some important aspects of differential diagnostics presented in the ZJJYJ have been overlooked. For example, why are particular acupoints included on a specific channel? Does position in a channel sequence affect its clinical applications? Examining such relationships requires extensive analysis of the unique categorization system of indications for all acupoints and the 14 channels included in the ZJJYJ. For the present preliminary study, data were restricted to the 20 Large Intestine (LI) channel acupoints. The study aims were to compare CM clinical indications among the LI channel acupoints and to determine if there are distinct patterns in indications along the length of the channel from LI 1 (fingertip) to LI 20 (face).
Materials and Methods
Two editions of the ZJJYJ were used: the Song Dynasty Chinese edition (1077) 3 and the sole English translation of The Systematic Classic of Acupuncture and Moxibustion (1994) translated by Yang and Chace, 4 together with additional translation clarification and advice with the latter editor (Charles Chace, DiplAc, DiplCH, LicAc) ). Each of the 61 RP indications described for the LI channel acupoints was coded in terms of its occurrence in the relevant diagnostic Book (B) and Chapter (C) Part (P) and the acupoint's ordinal position in the channel sequence. Quite commonly, in the ZJJYJ, individual acupoints are designated as RPs for more than one set of signs and symptoms. These may concern disease states presented in more than one diagnostic Book. Taken together, this set of RP attributes provides a clinical profile for the acupoint to determine disease states for which it is likely to serve as an appropriate intervention. The RP profiles for the LI points were also considered in relation to sequence position.
Results
Frequency Distribution of RPs by Sequence Position and Diagnostic Book
Figure 1 summarizes the relative frequencies of the 61 RP indications by acupoint and diagnostic Book. RPs were drawn from diagnostic categories from all six diagnostic Books. Note that LI 13 has been excluded because the ZJJYJ reported it as a point forbidden for acupuncture.
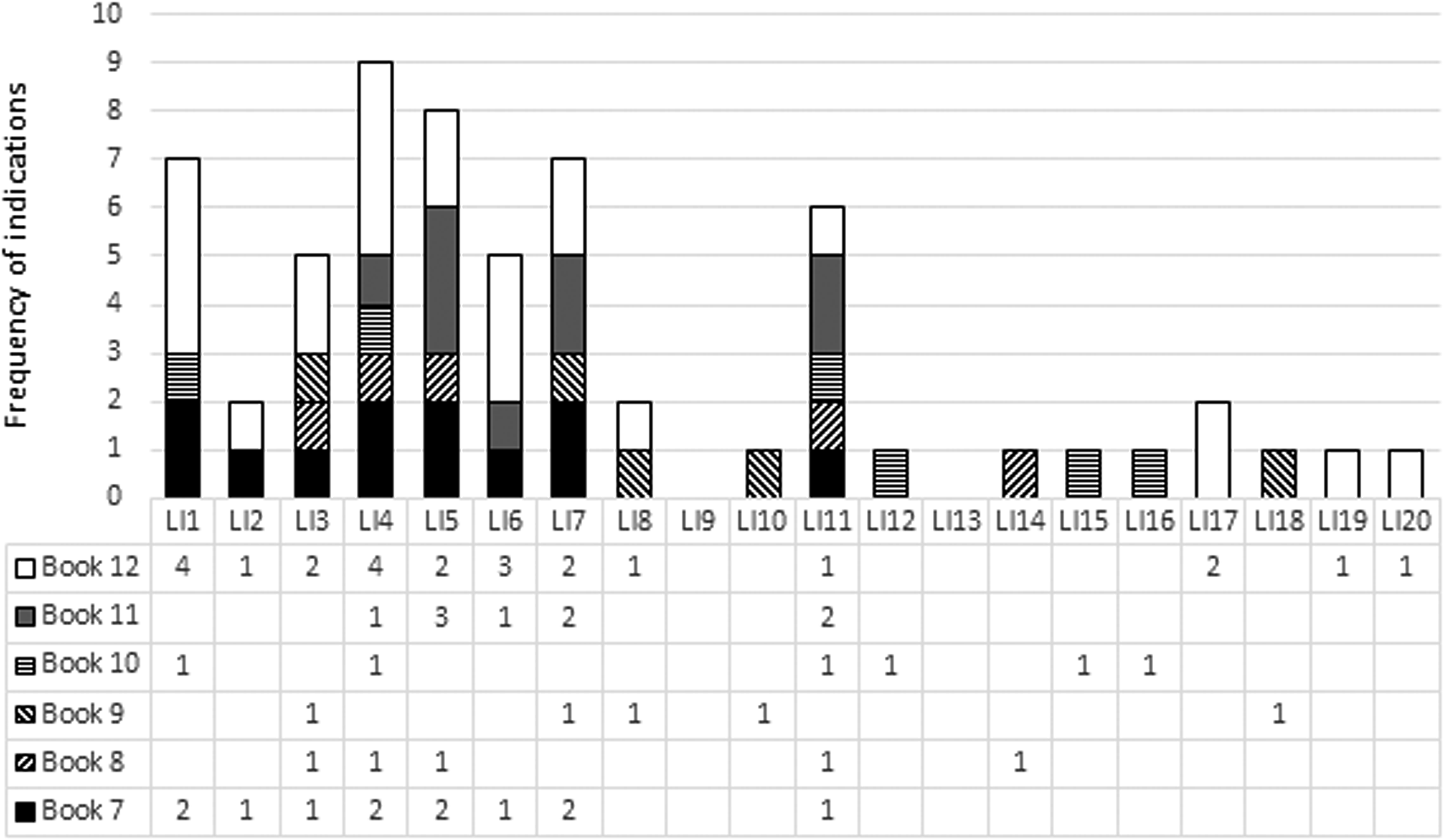
Frequency distribution of LI Channel Ruling Points. LI, Large Intestine.
As seen in Figure 1, even before considering the actual diagnostic signs and symptoms of individual RPs, it is obvious that there are distinct differences in the number and sources of RPs categorized by the ZJJYJ diagnostic Book along the acupoint sequence from LI 1 (fingertip) to LI 20 (face).
First, most RPs came from acupoints in the first third of the sequence, together with LI 11 midsequence at the elbow, while the rest of the channel acupoints have low RP contributions. LI 11's profile includes six RP indications and contrasts strikingly with the limited RPs associated with surrounding midsequence acupoints while closely resembling the RP profiles of the cluster of abundant acupoints in the first third of the channel, on the hand and wrist.
Second, the most frequent ZJJYJ diagnostic sources for the channel were from Book Twelve (white) with 24 RPs involving 12 LI acupoints; followed by 12 RPs from Book Seven (black) for 8 acupoints and 9 RPs from Book Eleven (dark gray) for 5 acupoints. While Book Twelve RPs were present for the length of the channel they were notably absent for the midsequence acupoints (apart from LI 11) from LI 9 to LI 16, whereas the 3 remaining Books (Eight, Nine, and Ten) were variously the sole sources of single RPs.
Third, there were several commonalities of source Books for subsets of acupoints. All 8 acupoints designated as RPs in Book Seven also had RP status for Book Twelve conditions. Furthermore, all 9 RPs from Book Eleven only involved 5 of this cluster of acupoints.
Comparison of RP Indications by Diagnostic Book and Sequence Position
This section concerns whether or not the RP clinical focus of the channel points is related to their sequence position. Tables 1 to 6 present the signs and symptoms stated for the complete set of RPs sourced from the six diagnostic Books.
LI, Large Intestine; RP, Ruling Point.
Book Twelve
Book Twelve (Table 1) contributed the most RPs, and all 24 of these focused on the head and throat. These RPs related to patterns of signs and symptoms of eye disorders or pain, nasal conditions, deafness/ringing in the ears, tooth decay and pain, throat pain, and inability to speak. Throat bi was specifically indicated in 8 RPs for 7 acupoints. Only the 4 RPs for the final few locally positioned acupoints had local effects on the throat, nose, and mouth. The other 20 were from the first 8 acupoints in the sequence, on the hand and wrist (and LI 11 at the elbow).
Book Seven
The only other well-represented Book was Book Seven (12 RPs) and all 8 acupoints with RP designations from it were located on the wrist, hand and elbow and, as previously indicated, were also ones with Book Twelve RPs. Book Seven's diagnostic chapters address disease caused by an external pathogen of Wind Cold and/or Heat based on the Six Divisional theory. 5 Table 2 shows the RPs for LI acupoints associated with clinical indications involving patterns of Cold damage and febrile disease (Chapter One) and various forms of nue (Chapter Five). There is a strong relationship between sequence position and Book Seven indications with RPs consistently present for the acupoints LI 1 to LI 7 and LI 11 but nowhere else in the sequence. When taken together with indications for the same acupoints in relation to, for example throat bi (see Book Twelve Table 1), fever may reflect a generalized response to severe throat and respiratory infections.
Book Eleven
Book Eleven considers various external diseases, often including signs and symptoms of cerebral involvement (seizures, deranged behavior, delirium, fever). For the LI channel sequence, this Book contributed nine RPs to only 5 LI points: LI 4 to LI 7 and LI 11 (Table 3). Eight of these RPs came from Chapter Two, which deals with Yang Inversion and Great Fright producing irrational behavior and seizure diseases. The third RP for LI 5, which came from Chapter Nine, suggests a link with severe systemic infection responsible for severe febrile and delirium symptoms. The Chapter focuses on Cold Qi intrusion producing Yong and Ju, and development of infectious infiltrating sores. Yong refers to seeping, inflammatory lesions and sores with thick painful scabs.
Notably, all 5 acupoints are also RPs for diagnostic patterns described in both Books Seven and Twelve. In addition, the RP descriptions are all consistent with compatible scenarios of advanced fever, delirium, infection of oral throat, and similar origins (see Tables 1 and 2). Therefore, these cerebral signs and symptoms might be caused by external pathogens, such as viruses and other microbial organisms, rather than by seizures and abnormal behavior of an endogenous origin.
Book Eight
All five Book Eight RP patterns were drawn from Chapter One (Table 4) and concerned transmission of disease among the five viscera producing Cold and Heat. Like Book Seven, the diagnostic focus is on febrile conditions. While the Book is a minor contributor to the channel, sequence position appears relevant; apart from LI 14, acupoints that were designated Book Eight RPs were also ones for Book Twelve and Book Seven. This is reflected in their indications that included various RPs for generalized fever and chills associated with systemic infections. Notably, the Book Eight RP signs and symptoms for LI 14 (Cold and Heat cervical scrofula [cervical TB] with [pain in and] inability to raise the shoulders) resemble a subset of signs and symptoms for LI 11 drawn from Book Eight and Book Ten (swelling in the neck, Cold and Heat) and from Book Ten (pain in the shoulders and elbows).
Book Nine
Overall, Book Nine addresses a range of internal diseases with varying pathogeneses. Table 5 shows that the 5 RPs came from four different chapters; involved 5 acupoints scattered along the channel from LI 3 to LI 18; and related variously to intestinal and urinary conditions as well as to signs and symptoms pertinent to the back, chest, arm, throat, and head. While no clustering or patterns related to sequence position among RPs was evident, the individual RP descriptors were in line with the broader clinical focus of other LI channel points, evident from among their complex sets of clinical indications.
Book Ten
Book Ten considered disease at the muscular level, and the main pathogen involved is Wind. 5 Table 6 shows that all six RP indications concerned pain or loss of function involving the shoulders and upper limbs. Three of the acupoints with Book Ten RPs were also designated as RPs for both Books Seven and Twelve (LI 1, LI 4, LI 11), while, for the remaining 3 acupoints (LI 12, LI 15, LI 16), Book Ten provided the sole RP. Spread along most of the sequence, and including three major acupoints associated with pain and fever, the notable commonality of signs and symptoms suggests an underlying systemic condition with effects on neuromuscular functions, for example, stroke-like rigidity and tremors.
Acupoint RP Profiles and Sequence Position
Each acupoint's unique clinical profile was determined from the combined signs and symptoms described by its designated RP(s) listed in Tables 1 through 6. The channel sequence included acupoints with complex clinical RP profiles (along the initial third of the channel sequence (and LI 11) and other (subsequent) acupoints with single RP foci. Comparison of the resultant clinical profiles for the two groups showed some complex sequence-linked RP relationships.
This is illustrated below using a simple example based on just one subset of LI 11's comprehensive RP clinical profile. The full profile, drawn from the following six RPs from five diagnostic Books (B) and chapters (C), comprises:
• B7C1—For Cold damage with residual Heat • B8C1—For fullness in the chest, pain (in the region) anterior to the auricles, toothache, red painful eyes, swelling in the neck, Cold and Heat, thirst, and sweating upon drinking but the skin turning dry and hot while not drinking • B10C5—For pain in the shoulders and elbows causing difficulty in contracting and stretching, inability of the hands to lift weights, and hypertonicity of the wrists • B11C2—For dim vision, hypertonicity of the wrist, generalized fever, fright mania, atonic limpness with bi heaviness, and tugging and slackening • B11C2—For madness with protrusion of the tongue • B12C8—For throat bi with inability to speak.
If comparisons are limited to the subset of the listed RPs for LI 11 to those involving shoulder and neck signs and symptoms, there are at least five such relationships with other LI acupoints. Listed below, these include the single RPs for LI 12, LI 14, LI 15, and LI 16, and both RPs for LI17.
• LI 12: B10C5—For aching, heaviness, and bi pain of the shoulder and elbow joints with inability to contract or stretch them
• LI 14: B8C1(2)—For Cold and Heat cervical scrofula with pain in (and inability to) raise the shoulders, upper arms
• LI 15: B10C5—For Heat in the shoulders and pain in the fingers and forearms
• LI 16: B10C5—For bi pain in the shoulders and upper back, inability to lift the arms, and Blood Stasis in the shoulders with inability to move them
• LI 17: B12C2—For sudden loss of voice with Qi choking, throat bi and swollen larynx, difficulty in breathing, and inability to swallow food and drink
• LI 17: B12C8—For throat bi.
Here, the RP indications for several LI acupoints with single RPs related to individual sets of signs and symptoms for LI 11. That is to say, not unexpectedly, an acupoint with multiple RP roles has a broader spectrum of clinical signs and symptoms for which it is an appropriate intervention in comparison with an acupoint with a single RP. Therefore, in keeping with the frequency distribution of RPs along the LI channel (as is evident in Fig. 1), the same division was evident with respect to RP clinical profiles. Complex clinical RP profiles were only present along the initial third of the channel sequence and LI 11, and not for other (subsequent) acupoints with single RP foci.
What is notable is that the limited array of signs and symptoms appropriate for an acupoint with a single RP designation, can serve to elaborate on (or perhaps “fine tune”) one or a few of the aspects of the multifaceted clinical scenarios covered by the compound RP profile for an acupoint with several RPs.
This synergistic possibility exists because the RP signs and symptoms and compound profiles for the sequence of LI points overall address a common clinical focus. Within this overarching framework, the position effect serves to modulate the breadth of the signs and symptoms addressed by individual acupoints. Multiple aspects are described for the initial third of the channel sequence (and LI 11), while subsequent acupoints have RP descriptions that elaborate on restricted aspects of the multifaceted clinical scenarios presented by the complex RP profiles.
Discussion
This study examined the series of 20 LI channel acupoints for evidence of relationships between sequence position and CM indications, based on the JYJ system of diagnostic RP indications. No single category of CM indications, as defined by the RP system, was common to all acupoints in the sequence. However, a series of relationships was identified, which, in general, emphasize the dominance of the initial acupoints in the channel (hand to wrist) and the closely related LI 11 at the elbow.
All but 10 of the 61 RPs for the channel came from acupoints in the first third of the sequence, together with the LI 11 midsequence. These acupoints all had multiple RPs drawn from across the six diagnostic Books. RP indications from Book Twelve were the most numerous (24), followed by Book Seven (12) and Book Eleven (9). The remaining Books (Books Eight, Nine, and Ten) all had limited presence and only contributed a single RP indication to 5 (Books Eight and Nine) or 6 (Book Ten) acupoints.
This same pattern of sequence-based RP distribution extended to the clinical intervention profiles for the acupoints. That is, acupoints in the first third of the sequence (and LI 11) had broad clinical profiles consistent with their multiple RP status drawn from across different diagnostic Books and comprising 51 of the 61 RPs for the entire channel sequence.
These profiles were consistent with sets of RP allocations to sequence-linked subgroups of acupoints. For example, there was a strong relationship among acupoints being RPs designated in Book Eleven as well as in Book Seven and Book Twelve. In this relationship, acupoints with Book Twelve RPs that address dental, and oral and throat signs and symptoms were likely to also serve as Book Seven RPs that were appropriate for dealing with fever, pain, and related symptoms that commonly accompany oral infections. In addition, while only 5 LI points (LI 4 through to LI 7 and LI 11) had RP status for Book Eleven–sourced diagnostic patterns, all 5 points were simultaneously RPs for diagnostic patterns described in both Books Seven and Twelve. These signs and symptoms were consistent with lapses into tremors, deranged behavior, and delirious delusional states that might accompany extreme fevers, stemming from advanced ear, nose, throat, and generalized infections, including respiratory, chest and gastrointestinal-related conditions.
Notably, the few RPs sourced from the remaining three Books are also in keeping with the primary focus of RPs for acupoints along the sequence. The descriptions encompass facets of advanced, significant abdominal and generalized infections with severe febrile components, including mental effects, such as agitation, tremors, delusions, and confusion.
With respect to the sequence and RP signs and symptoms, there was little or any evidence of local effects. Involvement of centrally activated or mediated effects, particularly for the frequent fever and disturbed lucidity, seem to be more likely. For example, the major source of RPs for the channel was Book Twelve, wherein the entire Book focuses upon the head and neck. However, only 4 RPs were contributed locally by three of the LI sequence acupoints in the head/neck region, with the remaining 20 coming from the hand (19) or elbow (1).
The diagnostic descriptions for all the channel points, for individual RPs drawn from all six Books illustrate appreciation of the multifaceted nature of clinical conditions and therefore of their treatment.
Importantly, these comprehensive descriptions originated many decades before Mi's systematically recording them in the JYJ. That suggests that the RP system described in the Ming Tang was itself based on extensive careful and sound clinical observations. This would have been essential for identifying and describing individual signs and symptoms; their clustering in related patterns (e.g., different forms of febrile disease); and the relationship between the presence of particular RPs and individual channel locations deemed to be acupoints.
Conclusions
On the LI channel, the sequence position was found to be relevant to CM indications in a systematic manner. While there were no diagnostically relevant attributes that were common to all 20 LI points, the RP attributes and profiles for the sequence of LI points, overall, reflected a common clinical focus, while position effect concerned the breadth of the signs and symptoms addressed by individual acupoints. Multiple RP signs and symptoms were described for the initial third of the channel sequence (and LI 11), while subsequent acupoints had generally single RP designations and thus elaborated on restricted aspects of the multifaceted clinical scenarios presented by the complex RP profiles. Different pattern clusters of RPs were evident for different subsets of acupoints and mainly concerned the RP diagnostic indications from Book Seven, Eleven, and Twelve. Another feature of the channel is the relative absence of diagnostic indications from Books Eight, Nine, and Ten.
The LI channel is only one of 14, several of which have extensive RP presence for the same or similar body regions to the LI channel. Within the LI channel alone, there were clusters of similar or related RPs from different diagnostic Books. Therefore, extension of awareness of relevant RPs to include those sourced from other channels may refine further the differential diagnoses of complex clinical conditions and their CM treatments.
Footnotes
Acknowledgment
Thanks are extended to Charles Chace for sound advice and guidance in deciphering Classical Chinese characters.
Author Disclosure Statement
No conflicts of interest exist.