
Abstract
Abstract
Background:
Burning mouth syndrome (BMS) is described as a sudden bilateral orofacial pain characterized as burning, scalding, tingling, or numbness. Diagnosis remains challenging and therapeutics are equally difficult. Complete spontaneous remission is rare. This article reports a case of BMS managed successfully with acupuncture.
Case:
A 53-year-old woman presented with a 3-year history of orofacial pain described as “burning, tingling, pins, scalded, numbness and electric shock” sensations, with a profound impact on her daily activities. A physical examination showed no visible lesions and examinations yielded unremarkable results. She was diagnosed with BMS and prescribed pregabalin and tramadol, as she had no benefits from rescue therapy after 6 months. She was then offered 8 acupuncture treatment sessions with a weekly frequency. Points used were local points of the trigeminal innervation (ST 5, ST 6, ST 7, SI 18, GB 2, and TE 21) and systemic action points (GV 24, LI 4, ST 44, and ST 36).
Results:
At her 3-month follow-up, she presented with mild, episodic pain that disappeared spontaneously. She did not need rescue medication and had significant clinical pain relief and global improvement of her health status. At her 6-month follow-up, she was not experiencing any pain, was not taking any medications, and had been sleeping well. She reported a global improvement of her health status and rated her change as “very much improved.”
Conclusions:
This case highlights the utility and effectiveness of acupuncture for BMS. Acupuncture, with few side effects and high tolerability, is a valid and effective therapeutic option for patients presenting with BMS.
Introduction
B
BMS can be organized into two main clinical forms based on etiology: (1) essential/idiopathic, wherein no cause can be identified; and (2) secondary, resulting from local factors or systemic conditions, such as diabetes mellitus, hypothyroidism, systemic lupus erythematosus, candidiasis, or medications. 2 Another classification system has been proposed based on the diurnal fluctuations on symptoms: type 1 (35%) is characterized with progressive pain (patients wake up without pain that then occurs and increases throughout the day (this is associated with systemic diseases); type 2 (55%), wherein the symptoms are constant during the day (patients find it difficult to fall asleep; this is associated with psychologic disorders); and type 3 (10%), with intermittent symptoms (atypical location and pain; this is associated with allergic reactions). 3 Although the etiology is unknown, BMS appears to be multifactorial. A neuropathic mechanism for BMS is currently favored. However, whether a peripheral or central dysfunction prevails is still debated. 2
There are at least 3 distinct subclasses of idiopathic BMS subclinical neuropathic states that have been identified: (1) peripheral small-diameter fiber neuropathy of the intraoral mucosa (50%–65%); (2) subclinical lingual, mandibular, or trigeminal system pathology (20%–25%); and (3) hypofunction of dopaminergic neurons in the basal ganglia (20%–40%). 4
Diagnosis remains challenging, as diagnostic criteria are not sufficiently defined or universally accepted. There are several confounding diagnoses, and the clinical presentation is often variable. 2 Because idiopathic BMS is an exclusion diagnosis, a thorough investigation for local and systemic factors associated with secondary BMS is necessary. Therapeutics are equally controversial and difficult due to lack of evidence, few case reports on alternative therapeutic options, and the existence of several pharmacologic therapies. A complete spontaneous remission within 5 years is rare (3%), 5 and moderate improvement is achieved in only 30% of patients. 6
This article reports a case of idiopathic BMS that was managed successfully with acupuncture.
Case
A 53-year-old woman was referred by the Department of Oral and Maxillofacial Surgery Porto, of the Centro Hospitalar do Porto, in Portugal, to the hospital's Chronic Pain Unit. She had a 3-year history of orofacial pain. She also had a history of migraines, anxiety, and panic attacks (with regular follow-ups with her psychiatrist), allergic rhinitis, chronic gastritis, epilepsy, and a radical thyroidectomy 2 years before for a thyroid follicular carcinoma. Her medications were levothyroxine (137 μg), levetiracetam (250 mg), omeprazole (40 mg), and alprazolam (0.75 mg). With no obvious precipitant factors preceding the event, she started to complain of orofacial pain that had become intolerable in the preceding year. The pain was mainly restricted to the right palate, gum, and tongue. It was described as “burning, tingling, pins, scalded, numbness and electric shock” sensations. The numbness initially started at the gum and spread up to the temporomandibular articulation. This pain had a spontaneous onset with no known precipitant factors and started mainly during the morning, progressively worsening throughout the day. This pain was aggravated by cold temperatures, spicy foods, and stress, and there were no relief factors.
The patient considered that this symptomatology had a profound impact on her everyday life. According to the Brief Pain Inventory, she rated, in the last 7 days, pain severity, using a numerical scale (NS), as 10/10 for the worst pain, 9/10 for the average pain, and 6/10 for the least pain. For daily interference, her NS rating was >7/10 for general activity, mood, normal work, relations with other people, sleep, and enjoyment of life. She scored 9/21 for anxiety and 9/21 for depression on the Hospital Anxiety and Depression Scale. Her score for the DN4 (Douleur Neuropathique) questionnaire was 4/10.
Objectively, this patient presented with a partial edentulous upper maxillary arch with no visible lesions on inspection of the oral cavity. The physical examination also revealed hypoesthesia to a prick test with no other abnormalities. Laboratory investigations, including thyroid hormones, yielded unremarkable results, as did orthopantomography, an electroencephalogram, computed tomography, and magnetic resonance imaging of her head and neck. She had had a previous clinical observation by a dentist, which excluded any dental pathology that could explain the symptoms. After a thorough and extensive search for other causes of her orofacial pain, this patient was diagnosed with BMS. She was prescribed pregabalin (75) mg twice daily and tramadol (50 mg) as rescue therapy. After 6 months, on her reevaluation consultation, her symptomatology remained the same. She also reported intolerable side effects of the pregabalin (dizziness, nausea), rated her worst pain as 9/10, and according to the Patient's Global Impression of Change (PGIC), scale she reported no change in her condition.
After a multidisciplinary discussion, the patient was offered acupuncture treatment. Eight treatment sessions were provided, lasting 30 minutes each, on a weekly basis. Needles with silver-plated handles, round heads, and guide-tubes were used (Ener-Qi 0.26 × 25 mm and 0.26 × 40mm). The acupuncture points used (Fig. 1) were local points of the trigeminal innervation ST (Stomach Meridian) 5, ST 6, ST 7, SI (Small Intestine Meridian) 18, GV (Governor Vessel–Dumai) 24 (0.3 cun depth of insertion), GB (Gallbladder Meridian) 2, and TE (Er Men) 21 (0.5 cun depth of insertion). Due to their systemic action and autonomic modulation properties, points, such as GV 24, LI (Large Intestine Meridian) 4 (0.5 cun depth of insertion), ST 44 (0.3 cun depth of insertion), and ST 36 (1.0 cun depth of insertion), were used. The patient completed the 8 sessions of acupuncture successfully, weekly, with no perceived side effects.
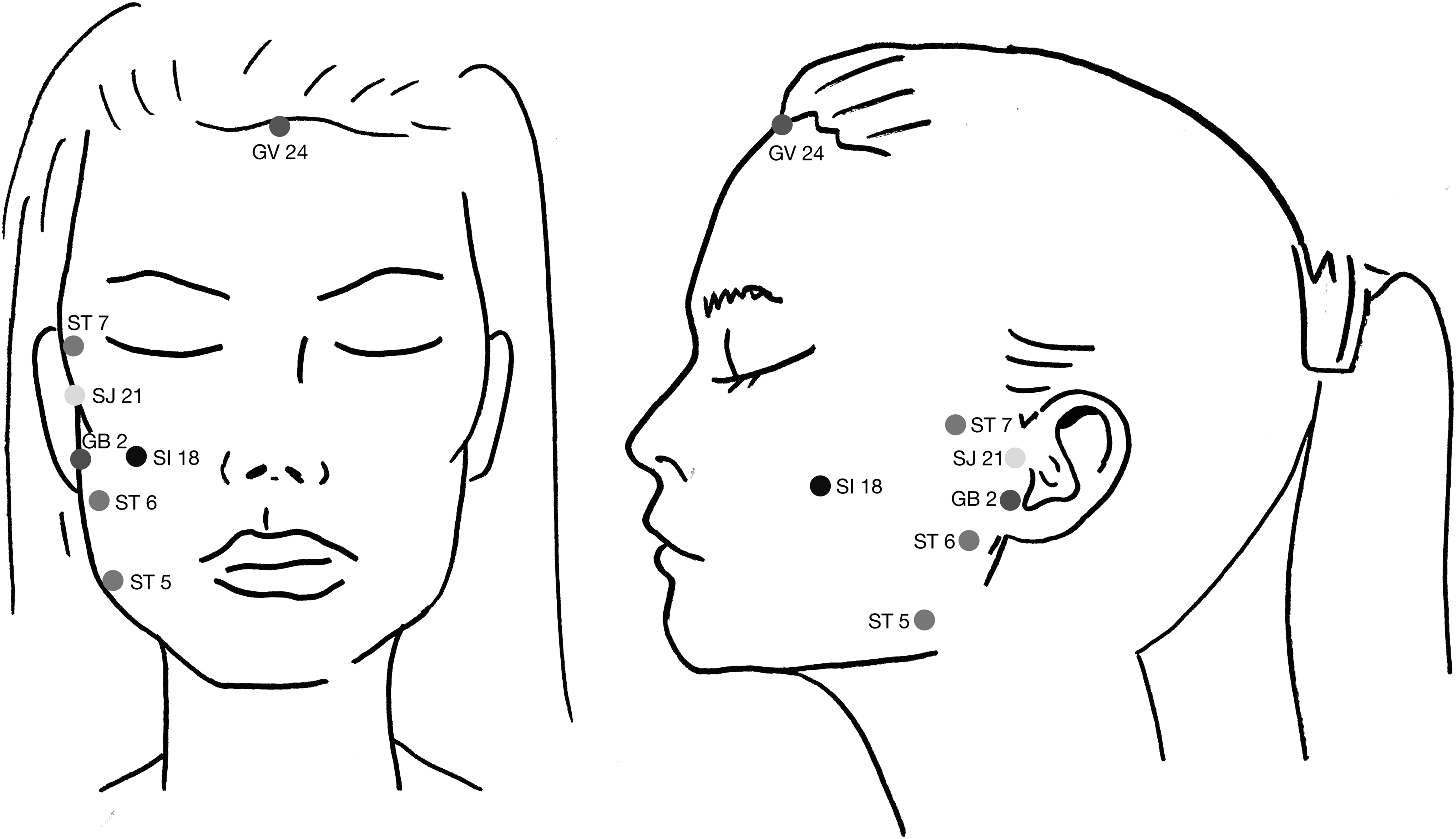
Face diagram with the acupuncture local points of the trigeminal innervation (ST 5, ST 6, ST 7, SI 18, GB 2, and SJ 21).
Results
After 3 months, the patient had mild, episodic pain that disappeared spontaneously, with no need for rescue medication. She had significant clinical pain relief (NS rating of 2/10) and a global improvement of her health status to 70/100 on the EuroQol 5-D measure of health outcome. After the 6-month follow-up, the patient was not experiencing any pain, was not taking any medications, and had been sleeping well. She reported a global improvement of her health status, with a 80/100 on the EuroQol 5-D measure of health outcome (mobility–1, self activity–2, walking hability–2, pain–2, and anxiety/depression–2). She rated her change as “very much improved” on the PGIC scale.
Discussion
This case report highlights the utility and effectiveness of acupuncture in a case of idiopathic BMS. Acupuncture had been proposed as a therapeutic possibility for the management of BMS. Scardina el al. 7 reported that, after 6 months of acupuncture on a monthly basis, a capillaroscopic observation of a patient's lower lip mucosa showed a modification of the vascular pattern, with a diminution of the arboresecent loops and an increase in vascular density. This was shown to be associated with a significant long-term reduction of the burning sensation (from a mean pain level of 8 on the numerical rating scale [NRS] to a 3 NRS rating after completion of treatment).
In a randomized controlled trial to assess the effectiveness of acupuncture versus clonazepam, researchers concluded that there were significant improvements with both treatments, albeit acupuncture showed fewer side effects. 8
Besides its analgesic properties due to segmental and central modulation, acupuncture has also vasomotor effects that improve microcirculation, namely the increment of arteriolar diameter, blood flow, and flow rate. 9 Acupuncture also influences sympathetic control on peripheral vascular activity, which might also explain the outcome achieved in this patient. 10 As BMS is a complex multifactorial syndrome, a cohesive multidisciplinary approach must be carried out in order to exclude potentially local or systemic etiologies of secondary BMS. In this case report, acupuncture provided an effective symptomatic relief of BMS. The patient reported substantial pain relief with no need for rescue therapy and a significant improvement in her quality of life.
Conclusions
This case report highlights that acupuncture may be a valid and effective therapeutic option for patients with BMS; this option presents few side effects and has high tolerability, compared to other therapeutic options. Acupuncture was helpful for this patient who had BMS. It will be valuable to explore whether other patients with BMS will also benefit from acupuncture.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest and no financial interests related to the material in this article.