
Abstract
Abstract
Background:
There is accumulating evidence from anatomical, physiologic, and neuroimaging research that demonstrate Classical acupuncture points stimulate nerve trunks or their branches in the head, trunk, and extremities.
Objective:
The aim of this research is to present novel graphic evidence that the embryologic development of the human nervous system in the extremities provides evidence that the distributions of the acupuncture Principal meridians correspond closely to those of the major nerves of the arms and legs, suggesting that the Principal meridians are representations of the human peripheral nervous system in those places.
Materials and Methods:
Using Adobe Photoshop software, anterior and posterior perspective diagrams of the adult human dermatomal patterns were modified to position the upper and lower extremities into their embryonic positions at 6 weeks' postconception. Dermatomes, major peripheral nerves, limb acupuncture points, and extremity Principal meridians were applied as separate graphic layers to this model using the anatomy texts of Netter and Clemente as anatomical references and the Shanghai College of Traditional Medicine text as the principal acupuncture reference to allow the relationships of these structures to be examined. Acupuncture cross-sectional anatomy references (Primal and Chen) were used for further confirmation of the findings.
Results:
The distributions of the acupuncture Principal meridians and their Classical acupoints in the extremities corresponded closely to those of the major nerves in these places.
Conclusions:
The marked similarities of the distributions of the Principal meridians and the peripheral nerves in the extremities advance the anatomical and physiologic evidence that acupuncture's clinical effects arise from nerve stimulation at Classical acupuncture points.
Introduction
“I
Six of these Principal meridians are located on the posterolateral aspect of the body and are termed Yang meridians, while the other six Principal meridians lie on the anteromedial aspect of the body and are termed Yin meridians. Two of the miscellaneous meridians (Governing Vessel and Conception Vessel) have clinical importance equal to the Principal meridians with their own Classical acupuncture points described, so thus are included with the twelve Principal meridians. 2
Blood and Qi (energy) in TCM physiology flow continuously through these meridians to provide nourishment to all bodily tissues. The 361 Classical acupuncture points described more than 2000 years ago were assigned on the basis of similar therapeutic properties to one of these sixteen meridians. 2
Since that time, there has been ongoing speculation about whether the Principal meridians represent only a conceptual construct 3 or have an anatomical basis. Potential anatomical bases of the meridians have been offered, such as Bonghan channels 4 and interstitial fluid channels. 5 Other researchers have postulated that the meridians may exist in the myofascial layer of the body. 6 The anatomically derived concepts of myofascial meridians described by Myers have distributions similar to those of acupuncture Principal meridians.7,8 Each of the Principal meridians is associated with a pulse, implying that they have at least some relationship to the vascular system. 2 Some degree of overlap of the meridians and the peripheral nervous system in the extremities has been described,2,9–11 and Chiang 12 has demonstrated anatomically and electrophysiologically that Classical acupuncture points are on different nerve branches and produce distinct responses to electrical stimulation.
Physiologically, human and animal experimental evidence demonstrates that anesthetic block of, sectioning of, or capsaicin application to the nerve innervating a Classical acupuncture point eliminates that point's acupuncture analgesia when it is subsequently stimulated,13,14 while occlusion or isolation of the acupoint's vascular supply has no effect on its analgesic effects. 15 These studies thus demonstrate that peripheral nerve stimulation is necessary to achieve acupuncture analgesia at Classical acupoints while their vasculature has no influence on their analgesic effects.
One of the great mysteries of TCM theory is that it describes all the major organs of the human body, yet it presents no representation of the central or peripheral nervous system. This is difficult to understand since there is evidence that the ancient Chinese had extensive knowledge of human anatomy based on dissections of executed criminals, 2 so it seems improbable that the peripheral nerves and brain were not visualized during these autopsies. Why were the central and peripheral nervous systems not described in TCM physiology?
The likely reason for this paradox can be explained by analysis of human developmental neuroanatomy. TCM had no need to describe a nervous system in its model of human physiology, as the acupuncture Principal meridians—previously thought to be only conceptual pathways that link acupuncture points with related clinical functions—are demonstrated herein to overlap fundamentally in their distributions to those of the human peripheral nervous system. This, in conjunction with corroborating anatomical and physiologic evidence, is consistent with a neurologic basis for the Principal meridians and acupuncture's clinical effects. This article also reviews this evidence for the extremities, with future articles to cover the head/neck and trunk regions separately, as, embryologically, these regions develop differently from the extremities.
Materials and Methods
Using Adobe Photoshop Elements software (Adobe Systems, Inc., San Jose, CA), anterior and posterior perspective diagrams of the adult human dermatomal patterns were modified to position the upper and lower extremities into their embryonic positions at 6 weeks' postconception. 16 Dermatomes, major peripheral nerves, limb acupuncture points, and extremity Principal meridians were applied as separate graphic layers to this model, using the anatomy texts of Netter and Clemente17,18 as anatomical references and a Shanghai College of Traditional Medicine text as the principal acupuncture reference. 2 This permitted the superimposition of dermatomes, peripheral nerves, cutaneous nerves, and/or acupuncture Principal meridians over the extremities to allow visual comparisons of the anatomical relationships of these structures. Additional confirmation of anatomic relationships with acupuncture anatomy references was obtained using the primal Anatomy for Acupuncture's 19 virtual human and Chen's 20 cadaveric analyses that provided cross-sectional anatomical analysis of acupuncture points.
Results
Developmental Evidence of the Neural Basis of the Principal Meridians in the Extremities
Human embryonic arm and leg buds in their early development 4–6 weeks' postconception can be visualized as growing in a linear manner anteriorly perpendicular to the longitudinal axis of the body, positioned so that the developing palm of the hand and sole of the foot oppose each other in a sagittal plane with the thumbs and great toes, respectively, pointing cephalad (Fig. 1). 16 This results in homologous positioning of the developing arms and legs.
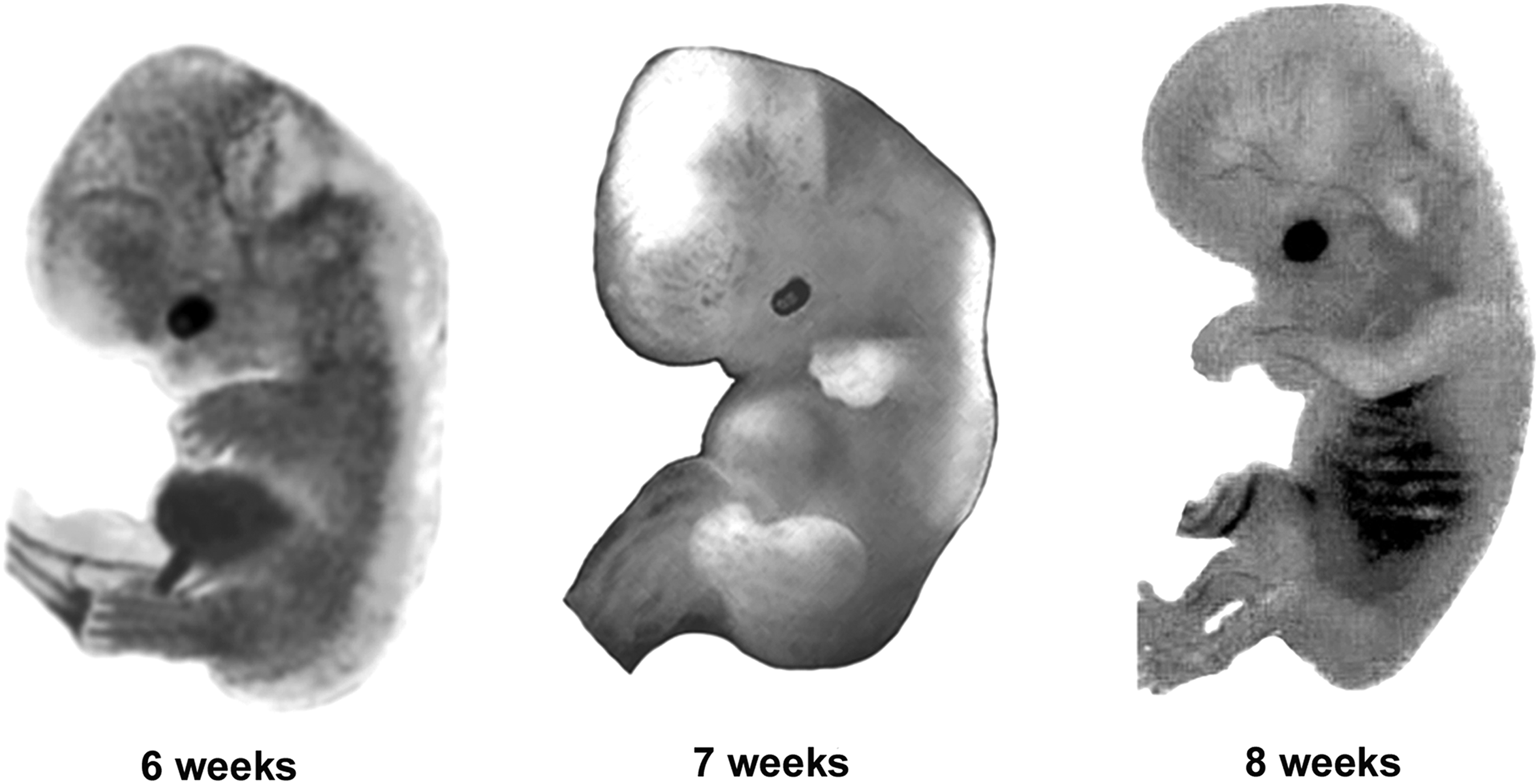
Human fetal development at 6–8 weeks' gestation.
Figure 1
During the seventh week postconception, the extremities form joint articulations. 16 In the following week, the upper extremities internally rotate and flex at the elbow to bring the hands over the chest region. At the same time, the lower extremities internally rotate, the developing knee joint flexes to ∼90°, and the developing ankle joint bends ∼90° to result in positioning of the sole of the foot inferiorly in a transverse plane, which is necessary later for the ability to stand (Fig. 1). If the adult human body is placed in 6th week developmental position (Fig. 2) by de-rotating the extremities and flexing the limbs at the shoulders and hips, important neuroanatomical relationships of dermatomes and peripheral nerves in the extremities become evident.

Adult dermatomes in derotated developmental positions (left), peripheral nerves of extremities superimposed on dermatomes (right).
Figure 2
Figure 2 shows that, in this sixth week developmental position, the dermatomes in the extremities approximate linear bands. Only on the anterior surface of the lower extremity does this relationship not hold true. Note that in this developmental position the arm and leg myotomes also will approximate linear bands lying under their corresponding segmental dermatomes. If the courses of the major peripheral nerves of the arms and legs are then applied to the model in Figure 2, then these nerves' distributions also become mostly linear and follow extremity dermatomes. This likely follows from the finding that embryologically the fetal peripheral arm and leg buds (with their developing muscles and neurovascular bundles) develop initially as linear structures until the sixth week of development.
Table 1
As shown in Table 1, the following anatomical relationships thus develop: The musculocutaneous nerve courses superiorly in the brachium and near the elbow its sensory branch, the lateral antebrachial cutaneous nerve, originates to supply sensory innervation to the superior/radial forearm to the level of the wrist (all on the ∼C6 dermatomal band). The radial nerve courses posteriorly in the brachium to become in the forearm the posterior interosseus nerve. Near the elbow, the radial nerve's sensory branch (the radial sensory nerve) originates that supplies sensation to the radial 3½ digits of the dorsal hand (all on the ∼C7 dermatomal band). The median nerve courses anteriorly in the brachium; and, near the elbow, its motor branch (the anterior interosseus nerve) originates to innervate the deep volar forearm musculature. The median nerve courses in the anterior forearm with its terminal fibers supplying sensory innervation to the radial 3½ digits of the palmar aspect of the hand (all on the ∼T1 dermatomal band). The ulnar nerve courses over the inferior brachium and forearm to the ulnar side of the hand, with its terminal fibers supply sensation to the little finger and the ulnar half of the ring finger (all on the ∼C8 dermatomal band).
In the lower extremity, the obturator nerve courses anteriorly in the thigh (over the L2 and L3 dermatomal bands). The femoral nerve and its terminal sensory branch the saphenous nerve course superiorly in the thigh and calf to the medial aspect of the foot (mostly on the ∼L4 dermatomal band). The lateral femoral cutaneous nerve and the superficial peroneal nerve course on the posterior aspect of the thigh and calf, respectively, and provide sensation to the dorsum of the foot (all on the ∼L5 dermatomal band). The sciatic nerve courses inferiorly over the thigh and calf with one terminal branch being the lateral plantar nerve which supplies sensation to the fibular/inferior aspect of the foot to the fifth toe (all on ∼S1 dermatomal band), while its other terminal sciatic branch is the medial plantar nerve that supplies sensation to the medial aspect of the heel and at times the proximal medial aspect of the plantar foot (all on the ∼S2 dermatomal band).
Note that the peripheral nerves (motor and sensory portions) overlie the appropriate dermatomes/myotomes in the 6th week developmental position. The fundamental overlap of acupuncture Principal meridians and the peripheral nervous system in the extremities as described in Table 1 is shown visually in Figure 3, where the distributions of the acupuncture Principal meridians literally superimpose on the distributions of the peripheral nerves there.
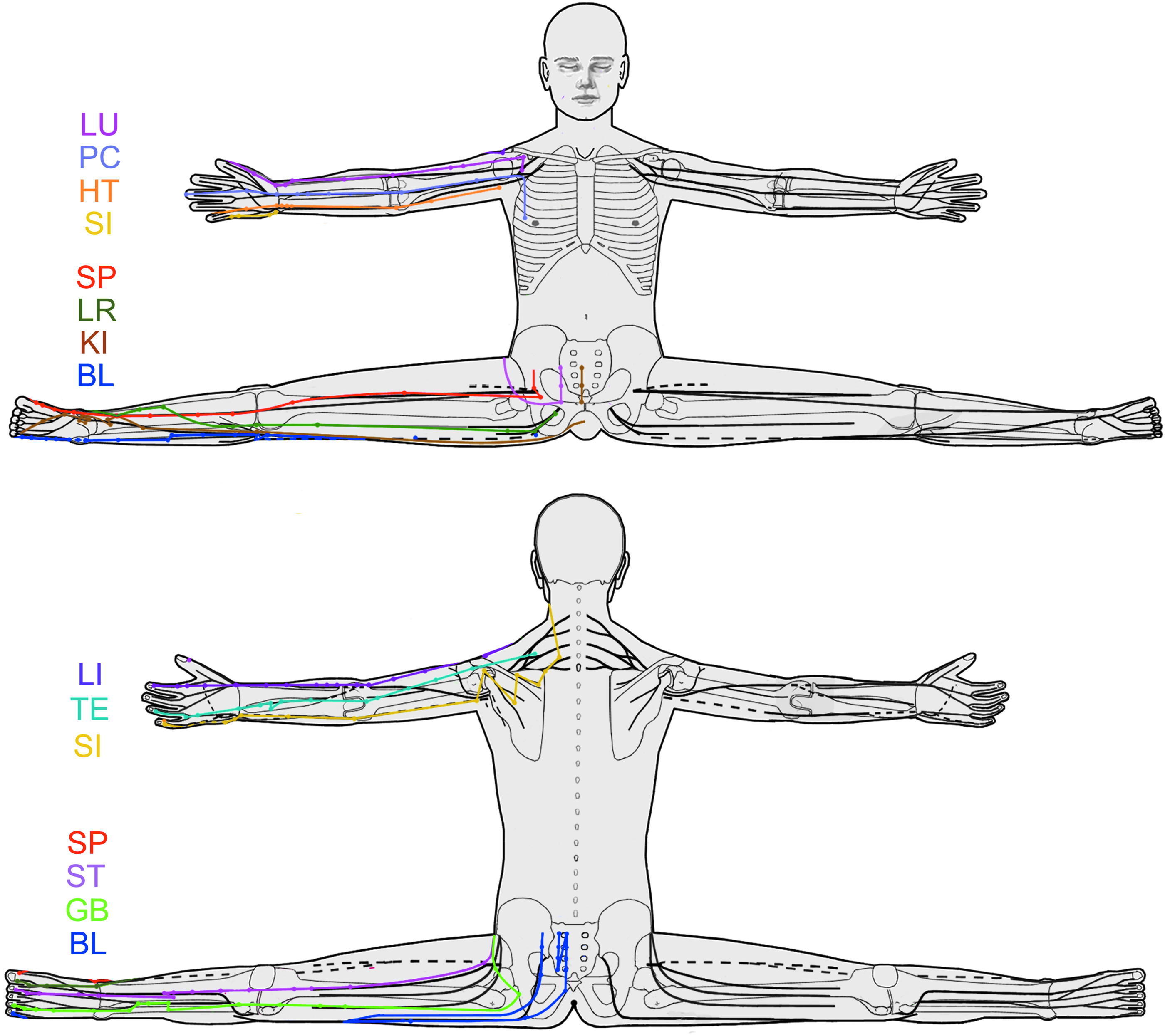
Acupuncture meridians (left) superimposed on the peripheral nerves of the arms and legs (right).
Figure 3
In this developmental position, all the Yin meridians are on the anterior surface of the body, and all the Yang meridians are on the posterior surface of the body. This is in accordance with TCM anatomy and physiology. 2 Acupuncture points on the anterior (Yin) meridians affect primarily the parasympathetic nervous system in producing their somatovisceral effects, while the posterior (Yang) meridians primarily affect the sympathetic nervous system in producing their somatovisceral effects. 11
Given that ∼20% of the spinal nerve fibers that form the peripheral nerves are autonomic nervous system fibers, 21 a plausible anatomical basis for autonomic innervation of the peripheral nerves' corresponding Principal meridians exists. The major peripheral nerves of the body are accompanied by vasculature (neurovascular bundles) as they course through the body. Sympathetic fibers invest these arterial walls,22,23 providing autonomic nervous system innervation to regulate vasoconstriction of those vessels.
Anatomical Evidence That Classical Acupuncture Points Exist on Peripheral Nerves or Their Branches
Acupuncturists have long known that some important acupuncture points are located directly on major nerve trunks. 2 For example, PC 6 is located on the median nerve above the wrist crease, BL 40 is located in the popliteal crease and contacts the tibial nerve, and KI 3 is located posterior to the medial malleolus and contacts the tibial nerve. 2 The Anatomy for Acupuncture virtual human anatomical software 19 and Chen's cross-sectional anatomy of acupoint reference 20 provide independent lines of evidence demonstrating that needles entering the Classical acupuncture points approximate peripheral nerves whose anatomic distributions match those of their corresponding Principal meridians.
Figure 4
As examples, for the head and neck region, BL 2 above the orbit approximates the supratrochlear nerve and GB 14 approximates the supraorbital nerve (Fig. 4). 19 The supratrochlear nerve courses over the medial aspect of the frontal region mirroring the distribution of the Bladder meridian there, while the supraorbital nerve courses more laterally over the frontal region mirroring the distribution of the Gallbladder meridian there. 19
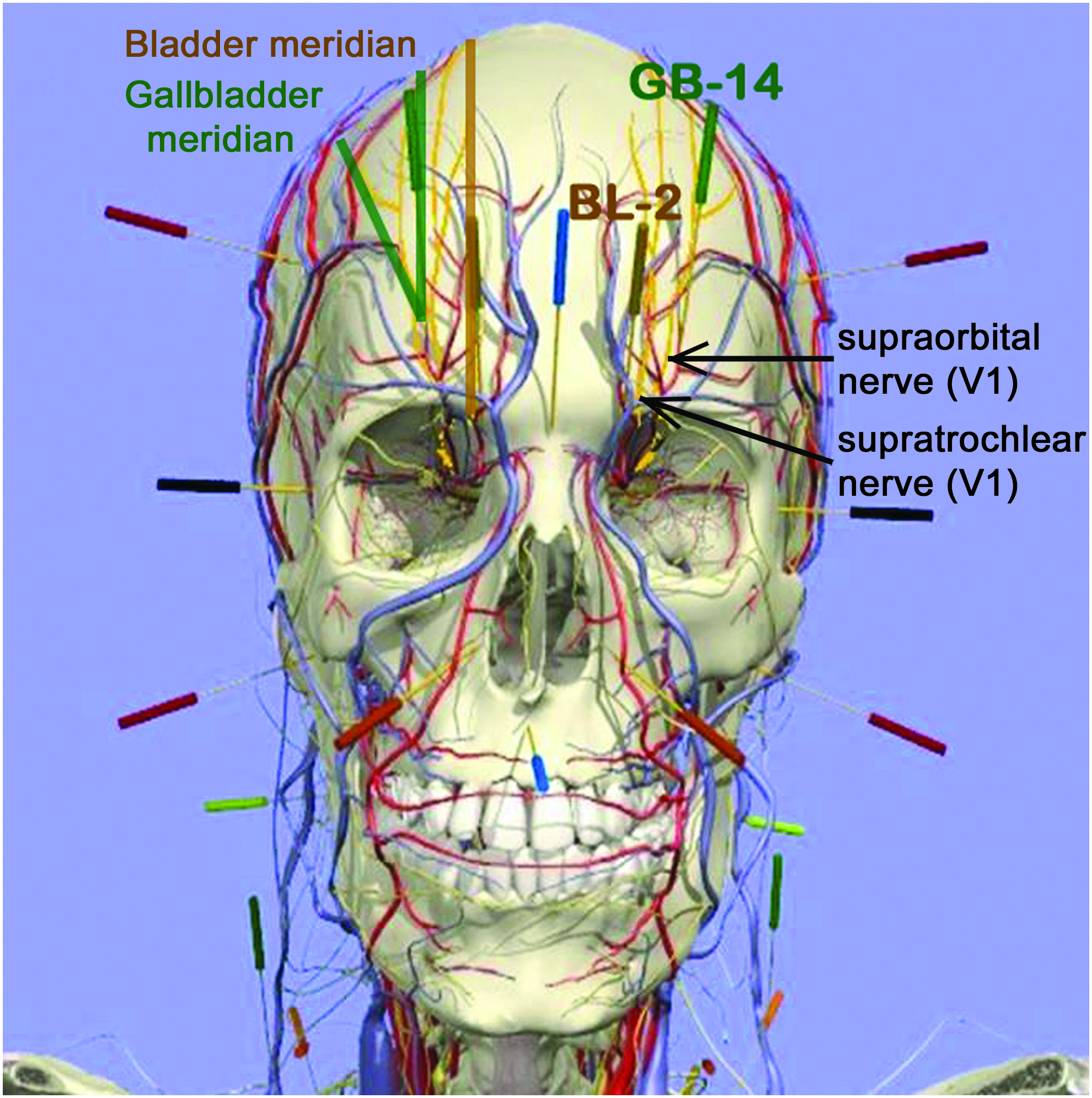
BL 2: Anatomical relationship to supratrochlear nerve (V1) and GB 14 anatomical relationship to supraorbital nerve (V1).
Figure 5
In the trunk, LU 2 is near the coracoid process and approximates the lateral cord of the brachial plexus (Fig. 5), 19 from which arises the musculocutaneous nerve in the upper arm whose lateral antebrachial sensory nerve innervates the radial forearm to the wrist, mirroring the distribution of the Lung meridian in those regions.

LU 2: Anatomical relationship to lateral cord of brachial plexus (in anterior view of left shoulder).
Figure 6
In the posterior shoulder, SI 9 in its deep position approximates the ulnar nerve (Fig. 6), 19 which extends along the posteromedial arm and medial forearm to innervate the last two fingers. This nerve distribution mirrors that of the Small Intestine meridian in these regions.
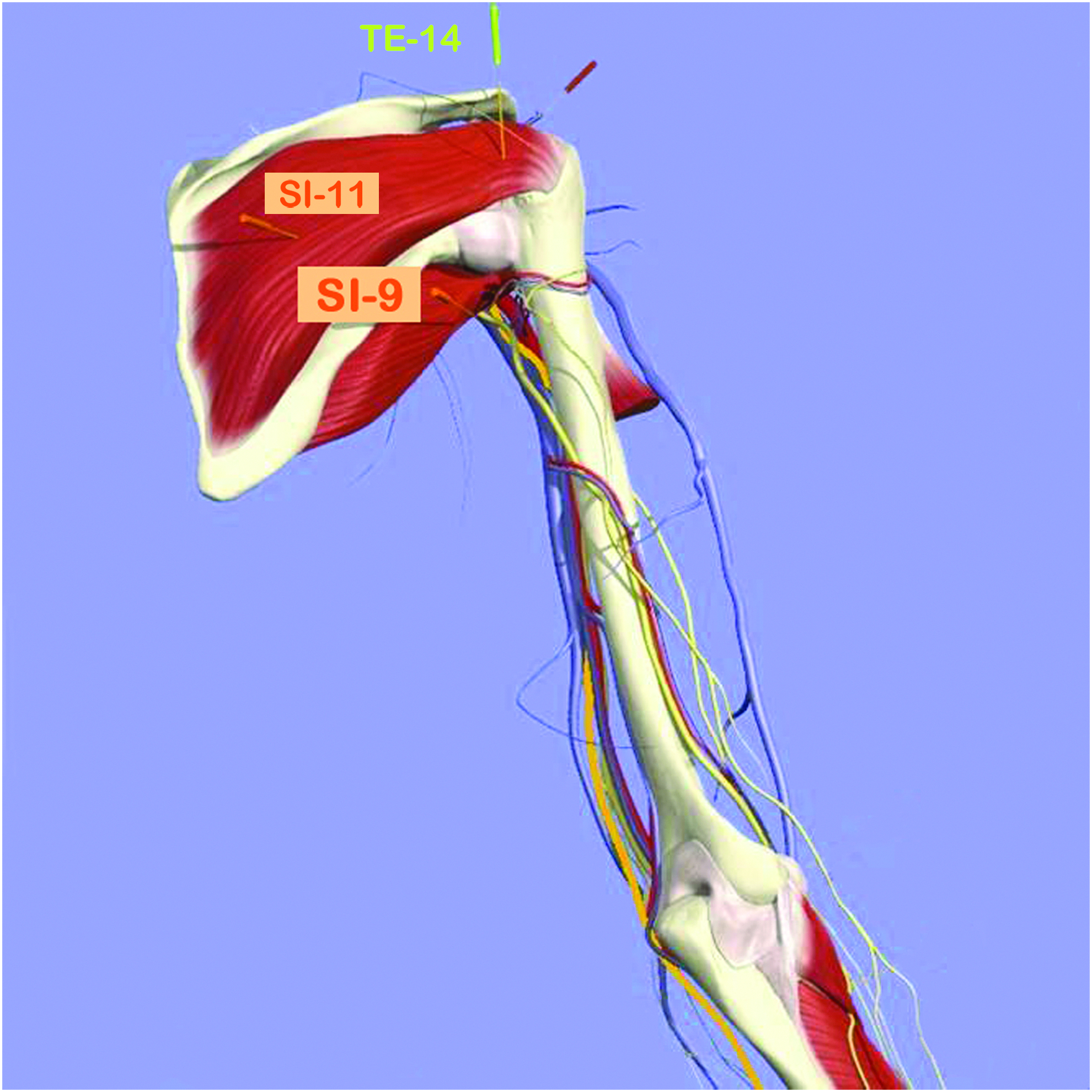
SI 9: Anatomical relationship to ulnar nerve (in posterior view of right shoulder).
Figure 7
In the lower extremities, GB 27 near the anterior superior iliac spine approximates the lateral femoral cutaneous nerve (Fig. 7), 19 whose distribution in the lateral thigh mirrors that of the Gallbladder meridian there. SP-12 is below the inguinal ligament and approximates the femoral nerve, 19 whose distribution extends along the anteromedial thigh to the medial knee with its sensory saphenous nerve branch extending along the anteromedial calf to the instep of the foot. This distribution mirrors that of the Spleen meridian in these regions.
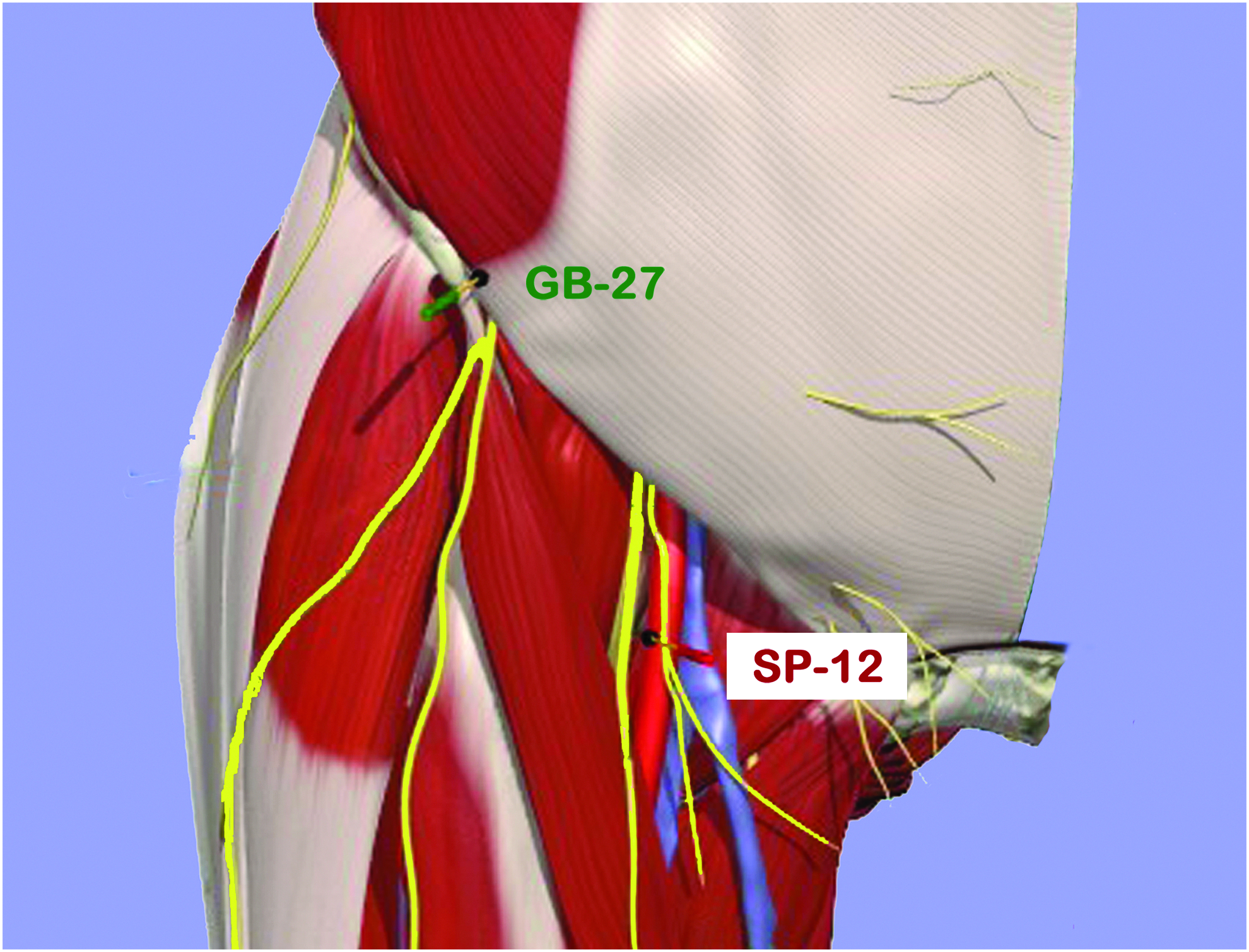
GB 27: Anatomical relationship to lateral femoral cutaneous nerve. SP 12: Anatomical relationship to the femoral nerve (anterolateral view of right hip).
Figure 8
BL 60, which is located posterior to the lateral malleolus, approximates the sural nerve (Fig. 8), 19 which courses along the posterolateral calf to the lateral ankle and foot. This distribution mirrors that of the Bladder meridian in the lateral calf and foot.
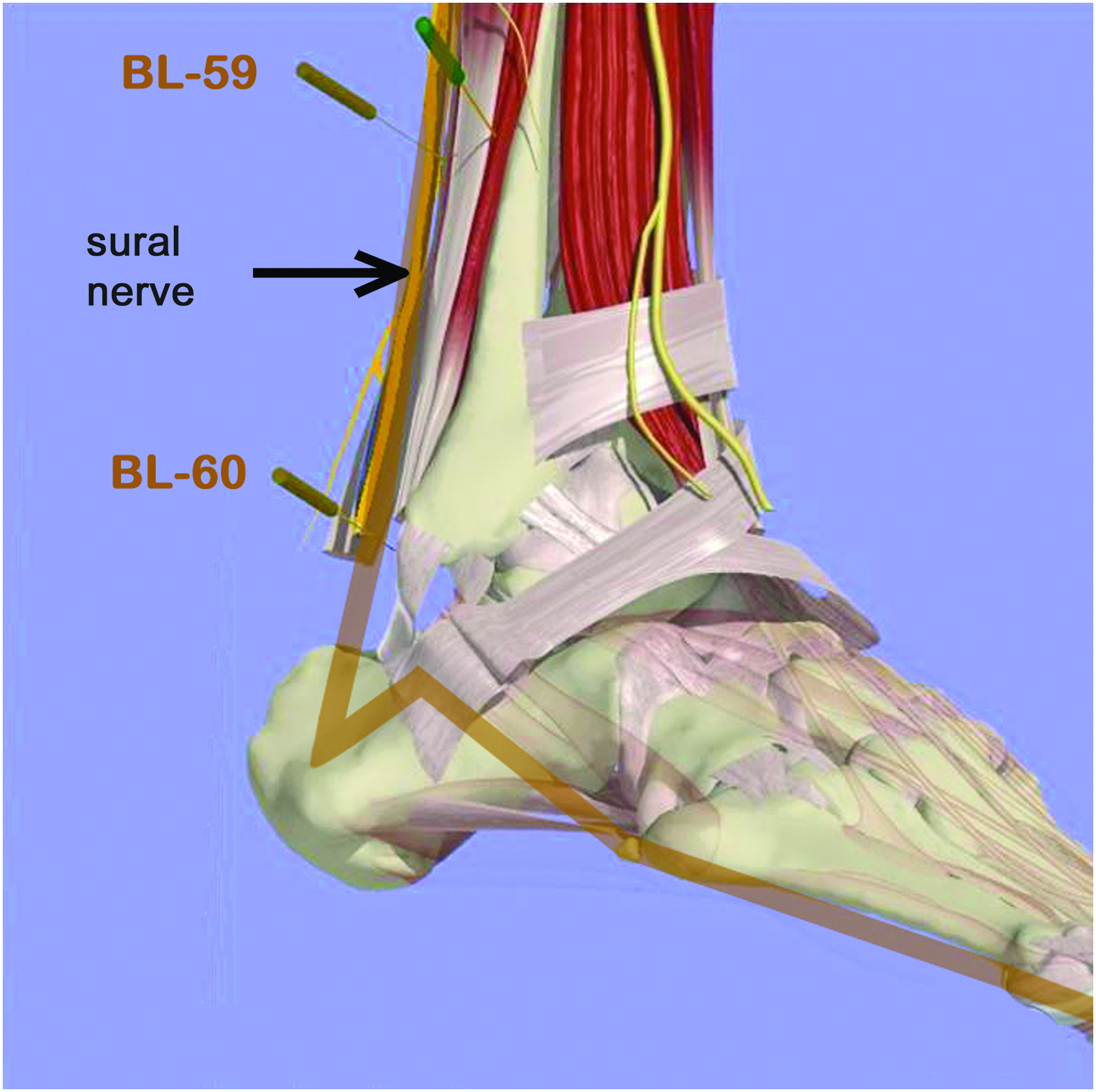
BL 60: anatomical relationship to sural nerve (lateral view of right ankle).
Note
It is important to emphasize that, for each of these examples in the head and extremities, the acupuncture points' Principal meridians mirror the distributions of the peripheral nerves they approximate.
Discussion
The fundamental correspondence of the Principal meridians with the peripheral nervous system in the extremities as previously outlined derives from indepth analyses of human embryologic development, human anatomy, and the cross-sectional anatomy of acupuncture needle passages at Classical acupoints described in widely available references.16–20 A limitation of the present study is that these relationships have not been demonstrated for every Classical acupuncture point in the extremities, and some of the graphics (Figs. 2 and 3) were created by the author and not validated at this point.
Embryologically, up to ∼6 weeks postconception, the human dermatomes, myotomes, and peripheral nervous system of the extremities develop in a largely linear fashion before the extremities develop joint articulations that allow limb bending and rotation into their approximate newborn positions. The distributions of the Principal acupuncture meridians mirror those of the peripheral nerves in the extremities when the fully developed human body is positioned akin to a 6-week embryo, and the cross-sectional anatomy of the Classical acupuncture points from Chen 20 and the Primal virtual human anatomical reference 19 provide independent confirmation of the fundamental overlap of the Classical acupuncture points and peripheral nerves. Sympathetic nervous system fiber distribution parallels the Principal meridians as well, via their innervation of the spinal nerves, their branches, and the walls of the arteries that accompany these peripheral nerves (neurovascular bundles).21–23
The results of this study have importance for acupuncture practice and research. These findings suggest that the target structures for needling in the extremities should not be muscles or fascia but rather peripheral nerves. The De Qi sensation would then be postulated to represent activation of nerve fiber endings when contacted by the needle, as confirmed by Hui et al. 24 The needle “grab” or muscle fasciculation would represent the result of stimulation of a motor axon due to acupuncture needle contact with the acupoint's nerve. Mechanical twisting of the needle in the fascia could be postulated to mechanically activate the small myelinated and unmyelinated fibers that penetrate fascia at acupuncture points. 25 The slow spread of the acupuncture Qi sensation along a meridian would reflect the slow transmission of unmyelinated autonomic fibers as well as central nervous system mechanisms. The autonomic nervous system innervation of acupoints would also serve to explain the edema, vasomotor, sudomotor, and pilomotor changes that may be seen at acupuncture points when needled.
A neurologic model of acupuncture effects would also provide a potential mechanism of how acupuncture styles that use subcutaneous needling (e.g., Japanese style) could produce their effects. Needling in the same cutaneous nerve and/or dermatome distribution that a Classical acupuncture point enters might then produce similar clinical effects.
In terms of research, then, placebo acupuncture point stimulation in the extremity, whether it penetrates the skin or not (e.g., Park or Streitberger needles), is not physiologically inert if applied in the same dermatome, myotome, and/or mixed motor/sensory nerve innervation as the Classical acupuncture point studied.
Melzack et al. in 1977 stated that “acupuncture points are associated with an ancient conceptual but anatomically non-existent system of meridians which carry Yin (Spirits) and Yang (Blood).” 3 The anatomical evidence outlined in the current study contradicts that statement. The authors of the Nei Jing 2000 years ago were seemingly aware of the nervous system through their dissections, but had no need to describe a discrete peripheral nervous system given that acupuncture Principal meridians are the expression of the peripheral nervous system and their accompanying vasculature in the extremities.
The Dutch physician Willem ten Rhijne, who observed acupuncture practice in Japan in the 1670s, was critiqued by Baldry 26 for reporting repeatedly that Chinese and Japanese acupuncturists used the terms artery, vein, and nerve interchangeably when describing the target of an acupuncture needle. The results of the present neuroembryologic and anatomical analysis of acupuncture meridians in the extremities (in conjunction with physiologic data) supports strongly that the acupuncture needle target appears to be the neurovascular bundles that course through the myofascial layers of the body and penetrate its fascia. Thus, ten Rhijne's descriptions actually would then be accurate descriptions of proper acupuncture technique. Indeed, in concordance of the results of the present analysis, in the mid-1700s the famous Dutch physician Gerhard van Swieten stated that “the acupuncture of the Japanese and the cautery of various parts of the body with moxa seems to stimulate the nerves and thereby to alleviate pain and cramps in quite different parts of the body in a most wonderful way.” 26 Thus, the TCM description that Qi (energy) and Blood circulate in the acupuncture meridians (i.e., neurovascular bundles) appears to reflect anatomical reality.
Conclusions
The acupuncture Principal meridians (and hence their Classical acupuncture points) in the extremities have strong anatomical correlations to the neurovascular bundles of the arms, which embryologic analysis demonstrates appears to derive from the linear development of the limbs and their dermatomes, myotomes, and nerves. This suggests that the Principal meridians and their Classical acupoints' functions derive from neural stimulation. This has implications for acupuncture techniques and research, especially when choosing points for placebo interventions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.