
Abstract
Abstract
Background:
Anxiety is a very common psychiatric symptom and can also occur in many physical conditions. Due to the limitations of conventional pharmacotherapy, the discovery of nonpharmacologic treatments that alleviate anxiety effectively is clinically important. Yintang (EX-HN 3), an acupoint located between the eyebrows, is known to have a mentally stabilizing effect in Traditional Chinese Medicine.
Objectives:
This preliminary review was conducted to investigate the current state of studies using acupressure or acupuncture on EX-HN 3 alone for anxiety, and to explore ways to apply this in clinical settings and future research, including systematic reviews and clinical trials.
Materials and Methods:
The authors searched 2 electronic medical databases, including PubMed and China National Knowledge Infrastructure, up to December 7, 2017, to collect clinical studies that used acupuncture or acupressure on EX-HN 3 only to relieve anxiety. Methodological qualities of included randomized controlled trials (RCTs) were assessed by the Cochrane risk-of-bias tool and a Jadad scale.
Results:
Five RCTs were included. Most of the RCTs were aimed at preoperative participants. In this population, the reduction of self-reported anxiety was consistently significant.
Conclusions:
Acupuncture or acupressure on EX-HN 3 was used mainly to reduce the anxiety of preoperative participants. The simplicity and economics of this intervention suggest the need for future rigorous clinical trials or systematic reviews on this topic. In addition, more experimental studies should be conducted to identify the underlying mechanisms of this anxiolytic effect.
Introduction
A
In order for acupuncture to be used extensively, in both the East and West, acupuncture's implementation needs to be simple. In this regard, it is especially promising to perform acupressure, a technique of pressing acupoints with a finger or noninvasive tool, or using an acupuncture sticker, which is a therapeutic tool for attaching a small needle or seed to acupoints. There is also scalability in cases when the number of acupoints used is small and their locations are easy to find to perform acupuncture or acupressure.
Yintang (EX-HN 3), an acupoint located between the eyebrows, is known to have a mentally stabilizing effect in TCM (Fig. 1). 6 Ajna, known as the third-eye chakra in the Hindu tradition, is also located in the same area as EX-HN 3. 7 EX-HN 3 is clinically useful because it is very easy to find and use even for beginners. In a recent systematic review of the effects of acupressure on anxiety, acupressure showed promising results for anxiety relief, and EX-HN 3 was one of the most commonly used acupoints. 8 However, there has been no systematic review of the anxiolytic effect of EX-HN 3, especially using this acupoint alone. Therefore, this preliminary review was conducted to investigate the current state of studies using acupressure or acupuncture on EX-HN 3 alone for anxiety, and to explore ways to apply this in clinical settings and future research.

The location of Yintang (EX-HN 3).
Materials and Methods
Study Search
Two electronic medical databases, including PubMed and CNKI [China National Knowledge Infrastructure] were searched to collect clinical studies that used acupuncture or acupressure on EX-HN3 only to relieve anxiety and reported the changes in anxiety symptoms as outcomes. The keywords used in each database were (
Study Selection
The inclusion criteria in this review were as follows:
(1) Study design: Clinical studies such as case report, case series, case-control study, nonrandomized controlled trial, and randomized controlled trial (RCT) (2) Population: No limitation (3) Intervention: Acupressure or acupuncture on EX-HN 3 alone (4) Comparison: No limitation (5) Outcome: Both qualitative and quantitative outcomes, such as the Hamilton Anxiety Rating Scale and the State–Trait Anxiety Inventory (STAI) assessing the severity of anxiety were allowed.
Two researchers reviewed the searched articles and selected relevant studies, independently. Any disagreement was resolved through discussion among the researchers.
Data Extraction
Using preplanned standardized forms, the 2 researchers extracted study designs, sample sizes, characteristics of participants, interventions, treatment periods, outcome measures, results, and adverse events of included clinical studies, independently. In particular, the acupressure or acupuncture methods were extracted according to the STRICTA [STandards for Reporting Interventions in Clinical Trials of Acupuncture] reporting guideline. 9 Any disagreement was resolved through discussion among the researchers.
Quality Assessment
Two researchers independently evaluated the methodological quality of the included RCTs using the Cochrane Collaboration's tool for assessing risk of bias 10 and a Jadad scale. 11 According to the Cochrane risk of bias tool, 10 the following characteristics were assessed as “Low risk,” “Unclear,” or “High risk”: (1) random sequence generation; (2) allocation concealment; (3) blinding of the participants and personnel; (4) blinding of the outcome assessment; (5) incomplete outcome data; (6) selective reporting; and (7) other biases.
The Jadad scale was used to evaluate the following
11
:
(1) Was the study described as randomized? (2) Was the method of randomization described in the article, and was that method appropriate? (3) Was the study described as double blinded? (4) Was the method of blinding described, and was it appropriate? (5) Was there a description of withdrawals and dropouts?
For questions 1, 3, and 5, a single point for yes or zero points for no were given. For questions 2 and 4, a single point for appropriate method use, zero points for no description of the method, or a minus single point for inappropriate method use were given. Therefore, the total score was 5 points, and a score of 3 points or more for a study meant that it was evaluated as having superior methodological quality. 11
Any disagreement between the researchers was resolved through discussion among the researchers.
Results
A total of 40 articles were searched. After excluding 1 duplicate study, the titles and abstracts of the remaining 39 were reviewed. After the exception of 31 irrelevant articles through the first screening, the full texts of remaining 8 were reviewed. One review article and 2 studies that used 2 or more acupoints to perform acupuncture or acupressure were excluded. Finally, 5 RCTs12–16 were included in the current review (Table 1 and Fig. 2).
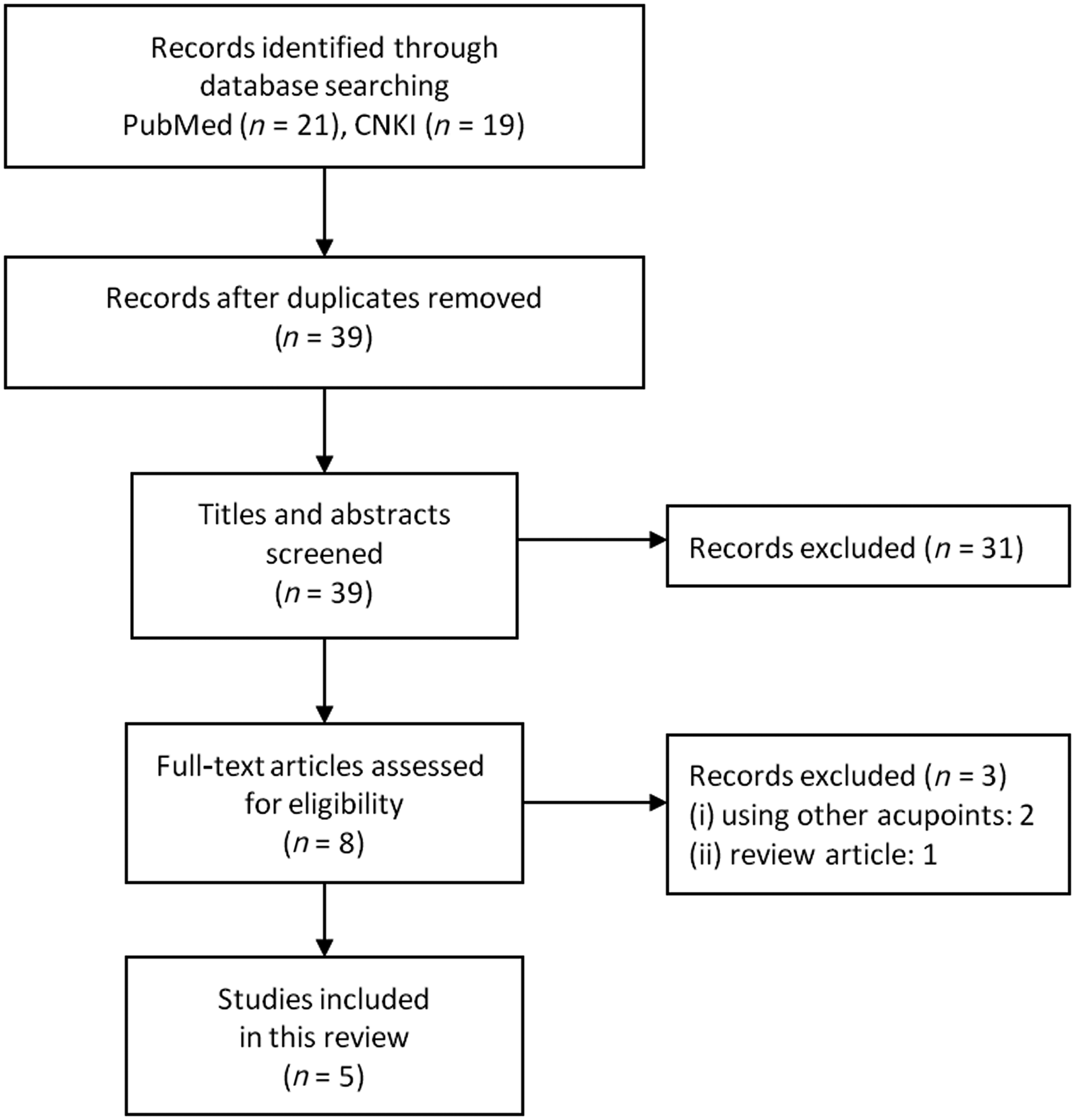
PRISMA [Preferred Reporting Items for Systematic Reviews and Meta-Analyses] flow diagram. CNKI, China National Knowledge Infrastructure.
≒, not significant (P > 0.05).
M, male; F, female; RCT, randomized controlled trial; NR, not recorded; min, minutes; STAI, State–Trait Anxiety Inventory; APAIS, the Amsterdam Preoperative Anxiety and Information Scale; PONV, postoperative nausea and vomiting; BIS, bispectral index; SBP, systolic blood pressure DBP, diastolic blood pressure; HR, heart rate; BP, blood pressure; VSS, verbal score scale.
Clinical Trials
Wiles et al. (2017), 12 in a RCT of preoperative participants, performed acupuncture using an acupuncture sticker on EX-HN 3 in an experimental group (EG; n = 62) and did not perform any intervention in a control group (CG; n = 62). As a result, anxiety scores measured by the 6-item short-form of the STAI (STAI-S6) and the Amsterdam Pre-operative Anxiety and Information Scale (APAIS) at 30 minutes postintervention were significantly decreased in the EG (P < 0.001 for STAI-S6; P < 0.001 for APAIS), but not in the CG (P = 0.829 for STAI-S6; P = 0.872 for APAIS). Postoperative pain intensity, opioid administration rate, and incidence of postoperative nausea and vomiting were similar in both groups.
Acar et al. (2013), 13 in a RCT of preoperative participants, performed acupuncture using an acupuncture sticker on EX-HN3 in an EG (n = 26) and sham acupuncture on a nonacupoint in a CG (n = 26). The anxiety score measured by the STAI-S, but not the STAI-T, at 20 minutes postintervention was significantly decreased in the EG (P = 0.018 for STAI-S; P = 0.156 for STAI-T). However, there were no significant reductions of the anxiety scores in the CG (P = 0.387 for STAI-S; P = 0.116 for STAI-T). All of the bispectral index (BIS) values measured every 2 minutes during 20 minutes after intervention initiation were significantly lower in the EG compared with those values in the CG (P < 0.0042).
Huang and Tang (2009), 14 in a RCT of preoperative participants, performed acupressure using a practitioner's finger on EX-HN3 in an EG (n = 40) and did not perform any intervention in a CG (n = 40). Anxiety scores measured by STAI at 20 minutes postintervention were significantly lower in the EG, compared with the anxiety scores in the CG (P < 0.01). Moreover, heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (SBP) at 20 minutes postintervention in the EG were all significantly lower, compared to the HR, SBP, and DBP in the CG (P < 0.05 for all).
Wang et al. (2005), 15 in a RCT of parents waiting for operations on their children, performed acupuncture using an acupuncture sticker on EX-HN 3 in an EG (n = 28) and sham acupuncture on a nonacupoint in a CG (n = 33). Anxiety scores measured by STAI-S at 20 minutes postintervention were significantly lower in the EG, compared to the CG (P = 0.03). However, there were no significant differences in the BIS measured every 5 minutes during 20 minutes after intervention initiation, and on HR and BP at 20 minutes postintervention between the groups (P-values were not presented).
Paraskeva et al (2004), 16 in a RCT of preoperative participants, performed acupuncture on EX-HN 3 in an EG (n = 25) and sham acupuncture on a nonacupoint in a CG (n = 24). Anxiety scores measured by a verbal score scale (VSS) at 15 minutes postintervention were significantly decreased in the EG (P = 0.027) and CG (P = 0.0001), with no significant difference between the groups (P = 0.368). BIS measured during the intervention was significantly decreased in the EG (P < 0.0001) but not in the CG (P-value was not presented) with no significant difference between the groups (P-value was not presented). The acupuncture or acupressure methods used in the included clinical trials are summarized in Table 2.
NR, not recorded; NA, not applicable; min, minutes.
Quality Assessment
Among the 5 RCTs12–16 included in this current review, according to the Cochrane risk-of-bias tool, 10 3 studies12,13,15 using a computer-generated randomization table were evaluated as “Low risk” in a random sequence generation domain. All clinical trials did not mention the information associated with allocation concealment and were rated as “Unclear.” All did not adequately perform the blinding of participants and personnel and were evaluated as “High risk.” However, 3 trials12,13,15 performed a blinding of outcome assessment. One trial, 12 using a per protocol approach, was evaluated as “High risk” in the incomplete outcome data domain, while 2 trials13,16 did not mention the information associated with incomplete outcome data and were rated as “Unclear” (Fig. 3). Jadad scores of only 2 studies12,15 were more than 3 points indicating superior methodological quality (Table 3).

Risk of bias summary.
Discussion
In this preliminary review, we collected clinical studies of using acupuncture or acupressure of EX-HN3 when treating anxiety, in order to describe the future direction of research about this topic and its possibility of application in clinical settings. All of the included clinical trials performed acupuncture on EX-HN3, except for 1 study 14 in which acupressure was performed. In 4 RCTs12,13,15,16 performing acupuncture, the authors of articles on 3 trials12,13,15 reported that they used acupuncture stickers, while the remaining trial 16 did not have a description of the materials used in the acupuncture procedure.
Most of included RCTs12–14,16 were aimed at preoperative participants. Acupuncture or acupressure on EX-HN 3 was performed for the purpose of reducing anxiety in preoperative waiting time. In most cases, the 20-minute intervention significantly reduced the participants' anxiety levels measured by STAI, compared to what occurred in participants in the wait-list or sham acupuncture groups. In 1 study, 16 a VSS was used as an anxiety scale and there was no significant difference between acupuncture and sham acupuncture. However, both groups showed significantly less anxiety than baseline. Studies using the BIS,13,15,16 which measures the level of arousal by measuring brain activity, reported mixed results. Two RCTs15,16 reported no significant differences between the EG and CG, and the other study 13 reported significant differences. In studies reporting BP and HR as outcomes,14,15 there were no significant differences in 1 study, 15 and the other study 14 reported significant differences. One study 12 reported that there were no adverse events associated with acupuncture of EN-HN 3.
The Cochrane risk-of-bias tool and a Jadad scale were used to assess the methodological quality of the included RCTs. Specifically, only 2 studies12,15 received more than 3 points and were evaluated as high quality when assessed by the Jadad scale. In all studies, blinding of participants and personnel was not performed perfectly, which is inevitable due to the nature of acupuncture or acupressure. Therefore, this might have led to the underestimated methodological quality.
One of the hypotheses is that acupuncture might modulate the activity of the sympathetic and parasympathetic nervous systems and control neurotransmitters in the brain through central autonomic regulation. 17 In one animal study, 18 acupuncture stimulation on EX-HN 3 was administered in a rodent depression model, and no significant changes were observed in both depression and anxiety. However, this might not reflect the effect of acupuncture on anxiety, considering that the authors of that trial stated that stress induced by immobilizing the rats to perform acupuncture could have led to anxiety in the animals. 18 Therefore, in order to elucidate the underlying mechanism of anxiolytic effect of this treatment, further experimental research with improved methodologies should be carried out.
EX-HN 3 can be used easily even by a doctor or a nurse who is not familiar with TCM, because this acupoint's location can be found easily, and the point can be stimulated easily using an acupuncture sticker or a practitioner's finger as well as a stainless acupuncture needle. In the studies included in this review, acupuncture or acupressure on EX-HN 3 was generally applied to preoperative participants. Considering the busy nature of clinical settings, it seems to be easier to attach an acupuncture sticker rather than to perform acupressure, which requires the practitioner to hold a finger on the acupoint for about 15–20 minutes. Attaching an acupuncture sticker on EX-HN 3 is economical because it does not require expert knowledge for the procedure and costs little to perform.
This preliminary review has the strength of describing, for the first time, the future direction of research using acupuncture or acupressure on EX-HN 3 for anxiety and its possibility of application in clinical settings. However, this review has the following limitations. First, given that this review was conducted for the purpose of considering the direction of future research and clinical applications, the diversity of databases searched was limited. This implies that there could be more relevant studies not included in this review. Further studies, such as a systematic review, may include the studies that have not been included in the current review but potentially relevant. Second, the results reported in each clinical trial were not synthesized; therefore, the results of this review cannot be used to estimate the anxiolytic effects of acupuncture or acupressure on EX-HN 3.
Conclusions
Acupuncture or acupressure on EX-HN3 was used mainly to reduce the anxiety of preoperative participants. Although the number of clinical trials on preoperative patients was small, the self-reported measure of anxiety reduction was almost consistently positive. The simplicity and economics of this intervention suggest the need for future rigorous clinical trials or systematic reviews on this topic. In addition, more experimental studies should be conducted to identify the underlying mechanisms of the anxiolytic effect of EX-HN 3.
Footnotes
Author Disclosure Statement
No competing financial interests exist.