
Abstract
Objective:
Pregnancy is a complex physical and hormonal condition. Many women experience back and pelvic pain, reflux, and headaches during pregnancy. There has been a significant rise in the popularity of acupuncture for pain conditions in pregnancy, wherein nonpharmacologic options are important. Concerns have been raised by both traditional and medical acupuncturists about using “forbidden points” during pregnancy and the risk of preterm contractions (PTC), as this could limit women's and practitioners' willingness to continue treatment during pregnancy. There is also a risk of bias introduced into clinical trials when participants are highly selected or they drop out of studies due to adverse outcomes. This review examined randomized controlled trials (RCTs) of acupuncture using forbidden points prior to 37 weeks of pregnancy to treat pain conditions, with the primary outcome of PTC.
Methods:
A database search identified RCTs, including trials of penetrating acupuncture that used forbidden points in their protocols to treat pregnancy-related pain conditions. STRICTA [Standards for Reporting Interventions in Clinical Trials of Acupuncture] and GRADE [Grades of Recommendation, Assessment, Development, and Evaluation] criteria were used to assess the quality of evidence. This review includes 8 RCTs reporting on 713 women.
Results:
Only 2 studies reported on the primary outcome of PTC, and there were insufficient data to perform a primary analysis. In these 2 studies, 6 participants withdrew due to PTC. No study was at a low risk of bias for all GRADE domains, and 3 studies were at high or unclear risk of bias in all domains.
Conclusions:
PTC is an important clinical outcome and should be reported routinely. The strength of evidence to date is insufficient to recommend using forbidden points prior to 37 weeks of pregnancy. Highly selected patient populations, risk of bias in study design, and participant withdrawal rates, suggest that high-quality trials are required.
Introduction
Pregnancy is a complex physical and hormonal condition for women. Many women experience back, pelvic, and other pain conditions during pregnancy associated with the change in weight distribution that occurs, but also due to the change in hormones to soften ligaments and tissue to accommodate the baby and prepare for birth.1,2 The most commonly experienced condition relates to back and pelvic pain. The Royal Australian College of General Practitioners describes lumbar pain as “pain experienced in the region between the last thoracic spinous process and first sacral spinous process, laterally bound by the lateral borders of the lumbar erector spine” 3 The experience of back and pelvic pain is multifactorial and influenced by physiologic, psychologic, and social factors. It is one of the commonest conditions of pregnancy, with a prevalence estimated to be between 25% and 90%, with the majority of women reporting that this pain affects their daily routines and capacity to work.2,4,5
Over the past decade, there has been a significant rise in the popularity of acupuncture for pain-related conditions, especially in pregnancy wherein nonpharmacologic options are important. Research in this area is reassuring, in that there are no reported increased rates of miscarriage or premature labor when treating pregnancy-related conditions with acupuncture.6,7
However, concerns have been raised by both traditional and medical acupuncturists about the use of so-called “forbidden points” during pregnancy.8,9 This small group of points were historically used to treat difficult labor, and, while some of these have been indicated for use as labor-preparation points after 36 completed weeks of pregnancy, other points are only indicated when the onset of contractions is appropriate. 10 With acupuncture on Large Intestine 4 (LI 4), Spleen 6 (SP 6), Bladder 32 (BL 32), and Bladder 67 (BL 67) being incorporated into medical-acupuncture research as part of point prescriptions for care, concerns about the possibility of these treatments stimulating preterm contractions (PTC) have been raised.11,12 PTC, even if they are self-resolving and do not result in preterm labor, are obviously very concerning to women. This has the potential to limit women's willingness to continue with treatment and practitioners' willingness to treat women during pregnancy.
The information on using these points is not straightforward, with some researchers recommending routine use at any time in a pregnancy, including the first trimester6,13 while others suggest caution and use indicated only post-36 completed weeks' gestation as labor-preparation/induction.14,15 Additionally, there are researchers who suggest that these points are indicated or “warranted” for particular conditions within the framework of Traditional Chinese Medicine (TCM) theory, and when a woman's personal constitution is considered.16,17 These differing approaches have the potential to create uncertainly among practitioners, despite an evidence base to recommend acupuncture for conditions such as pregnancy-related back and pelvic pain. 18
Evidence suggests that the effectiveness of these points is significant and point-specific when used for strengthening contractions and for pain relief during labor and birth.19,20 While review evidence reports no increase in adverse events beyond the background population rate when used during pregnancy,7,21 reports of adverse events, such as premature contractions, which could result in women withdrawing from the research studies or discontinuing treatment,22,23 create potential for bias within research and are not reported.
Currently, practitioners in maternity care include a range of allied health practitioners, such as physiotherapists, acupuncturists, medical acupuncturists, and specialist educators. As dry needling or medical acupuncture becomes part of the toolbox of allied health practitioners, it is important to note the role that relevant Chinese Medicine theory and traditions play in informing frameworks for diagnosis and treatment. Medical acupuncture, also known as Western medical acupuncture, is a system wherein classical points that stimulate the nervous system (segmental and extrasegmental points) are chosen, but without reference to TCM theory. 24 The loss of the traditional frameworks is reflected in some of the current evidence in which segmental acupuncture points are common with no reference to the guiding treatment principles. Use of these forbidden points is standardized regardless of individual presenting patterns 12 and the quality of evidence has not been assessed using specific critical-assessment tools designed for acupuncture interventions.
Therefore, to understand the potential effect of forbidden points during pregnancy the current authors examined published randomized controlled trials (RCTs) of acupuncture for lower-back, pelvic, and other pain conditions in pregnancy, with protocols that routinely include forbidden points. The primary outcome was incidence of PTC, and secondary outcomes included other adverse events, including preterm birth. To examine risk of bias and the quality of the current evidence for acupuncture for lower-back and pelvic pain, including study design, participant selection, generalizability of participant populations, and methods of analysis, the evidence was examined according to the STRICTA [Standards for Reporting Interventions in Clinical trials of Acupuncture] guidelines 25 and the GRADE [Grades of Recommendation, Assessment, Development, and Evaluation] criteria. 26
What Are the Forbidden Points?
A small group of acupuncture points were historically indicated for difficult labor. These were: SP 6, LI 4, GB 21, BL 60, BL 67, BL 32, and BL 33. 27 Of these points SP 6, BL 60, and BL 67 (with moxa) have been reported as being used prior to labor for labor preparation15,28 and during labor for pain relief and augmentation of labor. 19 Observational midwifery feedback has reported that SP 6 promotes cervical ripening and that BL 60 and BL 67 aid optimal fetal positioning. 15 This anecdotal reporting also included use of LI 4 and BL 32 for stimulating uterine contractions when appropriate and GB 21 to promote fetal descent during labor. The onset of contractions after acupuncture to BL 67 has also been reported.
Why This Is Important
Previous reviews on the safety of acupuncture in pregnancy—for conditions such as back, pelvic, and other pain conditions—suggest that acupuncture during pregnancy does not increase the risk of adverse events, compared to noninvasive control groups. However, the potential bias introduced by participant selection, participant withdrawal, and lack of intention-to-treat analysis—due to adverse events such as PTC—is significant for evidence translation. Many of these studies do not follow the STRICTA guidelines for reporting on acupuncture studies, nor have they been evaluated using the GRADE tool; therefore, the quality and generalizability of the research has not been examined to make recommendations on use of these forbidden points in practice.
Aim, Objectives, and Outcome Measures:
The aim of this review was to examine RCTs of acupuncture for back, pelvic, and other pain conditions, when studies used forbidden points prior to 37 weeks of pregnancy, with the primary outcome of PTC and secondary outcomes of other adverse events, and to assess the quality of this evidence. [Standards for Reporting Interventions in Clinical trials of Acupuncture]
With this aim in mind, there were 4 objectives for this review:
To determine the incidence of PTC in RTCs of acupuncture using forbidden points prior to 37 weeks of pregnancy to treat lower-back, pelvic, and other pain conditions To determine the incidence of other adverse outcomes in RTCs of acupuncture using forbidden points prior to 37 weeks of pregnancy for lower-back, pelvic, and other pain conditions To assess generalizability of the study population and analysis of participants, using STRICTA criteria To assess the quality of the research, using the GRADE criteria.
The main outcome measure was PTC. Secondary outcomes included other adverse outcomes and the results of assessments of the quality of evidence using the STRICTA criteria and the GRADE tool.
Methods
A database search was conducted to identify peer-reviewed original research published from January 1 2000 to June 5 2019. The search included the following databases: Cumulative Index of Nursing and Allied Health Literature (CINAHL) PubMed, and Medline® via Ovid. The following search strategy was used within all search fields in CINAHL, Medline, and PubMed. MeSH [Medical Subject Headings] were used; terms included: acupuncture OR acup* OR acupuncture* OR needling OR dry needling OR needl* AND back pain OR pain OR hip pain OR pubic pain OR pubic symphysis* OR symphysi* AND pregnancy OR preg* or gravi* AND randomised controlled trials OR RCT OR random*.
Manual searching was also conducted to ensure that known relevant articles were included in the review.
Selection Criteria
Articles were included if they reported peer-reviewed original research findings, used penetrating acupuncture to treat a pregnancy-related pain condition, and used forbidden points prior to 37 weeks of pregnancy as part of their treatment protocols. Articles were excluded if they were commentaries, editorials, systematic reviews, literature reviews, or non-randomized studies; did not use penetrating acupuncture; and did not use forbidden points in their protocols. Articles that were in languages other than English were translated when possible. The database search was supplemented by an internet search using the same search terms as above to identify any additional items, and bibliographic searching of included materials was also used to identify additional material. One author conducted the search and downloaded the results. Two authors independently examined the title and abstract of each result to identify relevant studies for inclusion. This review used a narrative approach.
RCTs of acupuncture were sought that compared verum acupuncture to placebo, sham, usual care, or other treatment methods to treat lower-back, pelvic, and other pain conditions during pregnancy, and routinely used any of the listed forbidden points in pregnancy.
The search yielded 52 studies with titles relevant to the selection criteria, which were assessed by two investigators independently (K.M.L. and D.B.). After duplicates were removed, 31 studies were screened; 15 of these were excluded, as they did not meet the inclusion criteria. The remaining 16, were reviewed for their full text, which resulted in 8 additional articles being excluded because the studies were not randomized (6 studies) or did not use forbidden points (2 studies). The remaining 8 articles were included in the analysis. Data were extracted by 2 study investigators independently (K.M.L. and K.L.S.). The CONSORT [Consolidated Standards of Reporting Trials] statement outlines these methods (Fig. 1).

CONSORT [Consolidated Standards of Reporting Trials] flow chart of acupuncture safety review. RCTs, randomized controlled trials.
Critical Appraisal Analysis Tools and Assessment of Bias
Critical appraisal tools assist assessment of bias that might be present in studies, due to their designs or other features, and lead to incorrect findings even if the bias was unintended. Bias refers to features of a study that can systematically affect or alter observations within the study and conclusions about the study, which might not reflect the underlying truth(s) of the study. 29 Study findings could then over- or underestimate the true effect(s) of the study. When assessing risks of bias, then, one considers the chance that the features of the study design, or conduct of the study, will yield misleading results. Sources of bias can result from study design, participant selections, and analysis and reporting methods (see Table 1). Ultimately, when findings are translated into guidelines and practice, the introduction of bias could lead to a waste of resources, loss of effective interventions, and even harm(s) for consumers. 30
The Cochrane Handbook for Systematic Reviews of Interventions 31 reported several sources of bias; these are included in Table 1.
Two main sources of bias are attrition bias and selection bias; these are discussed in the sections below.
Assessing Attrition Bias
Assessing outcomes—both anticipated and adverse—with as little bias as possible, is at the heart of RCT designs. When there is loss of participants following randomization, this is referred to as attrition and can introduce bias known as attrition bias. Attrition bias is an important aspect of any trial and, as a general rule, losses to follow-up of <5% of participants is considered to pose a low threat to study validity, while losses >20% pose a serious risk to study validity. 32 When there are differential or excessive rates of losses between groups, the characteristics of the groups change, and there is a loss of information about the acceptability and tolerability of the treatment, as well as its true effectiveness. 33
Assessing Selection Bias
When recruiting participants for research, there is an often reported difference in the participant population than the general population of interest. The randomization of participants, in theory, will balance these differences between the intervention and control groups. However, selection bias can arise because participants differ from the general population in ways other than what is being investigated in the study or intervention. 33 Research participants tend to be healthier and more compliant in general. It is therefore important to consider if the research population reflects the actual patients that one plans to apply the evidence to, if the treatment effect is exaggerated, or that the real patient population will be less tolerant of the treatment itself.
The inclusion of highly selected participant populations might limit generalizability of a study's results to the population of interest, and potentially contribute to selection bias due to confounding. 33 Additionally, real patients could experience more-significant adverse events due to their differing background health statuses. 34
Critical Appraisal Tools
This review used two critical appraisal tools. These were:
Revised STRICTA items for reporting acupuncture studies. 35 The aim of the STRICTA guidelines is to increase transparency in reporting trials, enable critical appraisal and interpretation of results, and provide sufficient detail for replication of studies. The STRICTA guidelines are designed to replace Item 5 in the CONSORT statement. 36
The GRADE tool is a transparent framework for developing and presenting summaries of evidence and provides a systematic approach for making clinical practice recommendations. 26 The Centre for Evidence Based Medicine, on its Catalogue of Bias website, describes the GRADE tool as a “systematic approach for assessing and communicating the certainty of evidence and going from evidence to recommendations or decisions.” 33
Results
This review included 8 randomized controlled trials, randomizing 856 women and reporting on 713 women. Trials were published between 2000 and 2012, and included between 40 and 386 participants each. All studies used a randomized controlled trial design and included the use of ‘forbidden points’ in their treatment protocols. Three studies included investigation into low back and pelvic pain, three studies investigated pelvic pain only, two studies investigated low-back pain only, one study each examined dyspepsia and tension-type headaches in pregnancy.
The studies were 2- and 3-armed trials. There were seven 2-armed trials, with two comparing two alternative acupuncture interventions, one using acupuncture at different gestational ages (20 and 26 weeks; Ekdahl and Petersson, 201022), and one using acupuncture at different depths (superficial versus deep needling; Lund et al., 200637). The 5 other controlled trials compared acupuncture to usual care (3 trials, Kvorning et al., 2004, 38 ; and Guerreiro da Silva et al., 2012, 39 200940), sham acupuncture (1 trial, Elden et al., 2008), 41 and an active control group of physiotherapy (1 trial, Wedenberg et al., 200042). One 3-armed trial compared acupuncture with usual care and an active control group of stability exercises (Elden et al, 200543).
Primary Outcome Measure—PTC
Most studies did not report on the primary outcome of this review, PTC (see Table 2), and there was insufficient data to perform a primary analysis of this outcome, so this outcome is reported narratively in this article.
Trial Details and Outcome Measures of RTCs
RTC, randomized controlled trial; acup, acupuncture; PTC, preterm contractions; TCM, traditional Chinese Medicine; HIV, human immunodeficiency virus; AIDS, acquired immunodeficiency syndrome; POMS, Profile of Mood States; VAS, visual analogue scale; DRI, Disability Rated Index; HRQoL, health-related quality of life; SC, standard care; NRS, numeric rating scale.
PTC were reported in 2 studies.22,42 The study by Ekdahl et al. (2010) 22 compared early (n = 20) and late (n = 20) acupuncture at 20 weeks and 26 weeks of gestation for low-back and pelvic pain. Overall, there were 8 withdrawals from the study, with 3 women experiencing PTC, 1 from the early acupuncture group and 2 from the late acupuncture group. These participants' outcomes were not included in the final analysis, that is, there was no intention-to-treat (ITT) analysis. The study by Wedenberg et al. (2000), 42 compared acupuncture (n = 30) with physiotherapy (n = 30) for low-back and pelvic pain. This study reported 2 exclusions from the acupuncture arm, due to crossover of treatment, and 12 withdrawals from the physiotherapy arm, 3 were due to PTC and 1 woman gave birth during the study period. There was no ITT analysis for this study and postrandomization withdrawals constituted a 23% dropout rate.
The other 6 studies did not report on PTC as an outcome.
Other Adverse Events, Withdrawals and Attrition Bias
There were withdrawals due to adverse events or loss to follow-up from all studies except 1, 39 with only one study stating that they followed an ITT analysis. 41 The other six studies, in which no ITT analysis was reported and dropouts were noted, accounted for the randomization of 698 women and reported on 563 women, constituting a dropout rate of 19.4%.
Two studies reported on preterm birth as an adverse event.41,43 The Elden et al., 2005 study 43 compared acupuncture with stabilizing exercises and usual care. In this study, there were 19 preterm births, 5 in the acupuncture group, 7 in the stabilizing exercise group, and 7 in the usual-care group. These withdrawals were included in the final ITT analysis. In the Elden et al., 200841 study, 2 women were reported to have had preterm births, both in the acupuncture group. They were not included in the final analysis. One study 38 reported that 3 women gave birth during the minimal study period, but their gestational ages were not reported and they were not included in the final analysis.
In the Lund et al., study, 37 the researchers reported 23 dropouts (13 from the superficial-needle group (including 1 who gave birth during the study period) and 10 from the deep-needle group). These losses constituted a 33% dropout rate, and their data were not included in the final analysis.
In 2 studies,39,40 the researchers reported that “no important adverse events occurred”; however there were 5 withdrawals from the 2009 study 40 (1 from the acupuncture group, 4 from the usual-care group), and outcomes were not included in the final analysis.
Most minor adverse events reported included bleeding, bruising, needle pain, drowsiness, nausea, fainting, allergy to nickel, or aggravation of symptoms (Elden et al., 200841; Lund et al, 200637; Elden et al., 2005, 43 ; Kvorning et al., 200442). Other studies did not report on adverse events (Ekdahl and Petersson, 201022; Guerreiro da Silva et al., 201239 and 200940). See Table 2.
Inclusion and Exclusion: Participant Selection Criteria, Selection Bias, and Generalizability
Most studies reported small sample sizes and participant selection criteria included only women in the second and third trimesters of pregnancy (See Table 2). Six of the studies included only healthy women with low-risk pregnancies, no risk factors contraindicating acupuncture, no other prior medical conditions, and having signs of low-back or pelvic-girdle pain (Ekdahl and Petersson, 201022; Elden et al., 200841; Lund et al, 200637; Elden et al. 200543), tension headaches (Guerreiro da Silva et al., 201239), or dyspepsia (Guerreiro da Silva, et al., 200940). Only 2 studies reported including all women presenting with the condition in the inclusion criteria.38,42
Other demographic information about the participants who were included in the studies was not reported in all but 1 study, 39 making assessment of participant differences at baseline not possible.
STRICTA Reporting Guidelines
The studies were evaluated according to the STRICTA guidelines for reporting of acupuncture trials 35 (see Table 3), and addressed each of the six items.
STRICTA Reporting Guidelines for RCTs
STRICTA, Standards for Reporting Interventions in Clinical trials of Acupuncture RCT, randomized controlled trial; acup, acupuncture; Rx, prescription; uni, unilateral; bi, bilateral; MA, manual acupuncture; EA, electroacupuncture; Fx, effects; moxa, moxibustion; lit, literature; CONSORT, Consolidated Standards of Reporting Trials; min, minute(s); wk, week(s); PTC, preterm contractions; mo, month(s) stim, stimulation; TCM, Traditional Chinese Medicine; max, maximum; hr, hour(s).
Item 1
Acupuncture rationale included reporting on style of acupuncture, reasoning for treatment approach, and the extent to which treatment varied between participants. For style of acupuncture and treatment theory, 2 studies41,43 used segmental acupuncture, 1 study reported using superficial verses deep acupuncture 37 but no theoretical framework was described. Kvorning et al. reported acupuncture with stimulation verses no acupuncture 38 but no theoretical framework was provided. Two studies39,40 reported using TCM theory according to the classics and TCM theory and trigger-point locations.
Treatment variation was according to site of pain in 3 studies37,38,43 and, in 1 study the emotional response to needling. 38 Minimal or no variation was reported for 4 studies,22,39,41, or was not described. 42
Item 2
Number of needles, location, depth, response sought, stimulation type, retention time and needle type were generally well reported, with only 1 study providing insufficient details for replication. 22
Item 3
Treatment regimens were well described in all studies.
Item 4
Other components of treatment were not reported in any study except the Wedenburg trial, in which details of the physiotherapy intervention (control group) were described. 42
Item 5
This item describes practitioners' backgrounds, including qualifications, affiliations, and information provided to participants. In the 2 studies by Guerreiro da Silva et al.,39,40 the practitioner received 600 postgraduate hours of training in acupuncture; however, no qualifications were provided. Two studies22,38 reported that the practitioners were midwives trained in acupuncture, and 1 study had a physiotherapist trained in acupuncture. 37 However, no further details or information about qualifications were provided. Three studies did not report on this item at all.41,43,45
Item 6
This item concerns reports on control or comparator interventions, including the rationale for the comparator and a detailed description of what the intervention includes. The rationale and description of the control group were well-reported in three studies,22,41,43 and Lund et al., provided details of the comparison treatment but not the rationale. 37 These were minimally described or not described at all in the four remaining studies. 38–40,42 See Table 3
Risk of Bias
Using the GRADE risk of bias assessment tool, 29 the areas of potential bias were examined, including, selection bias, performance bias, detection bias, attrition bias, and reporting bias (see Table 1). No study was at a low risk of bias in all domains. However, the study by Elden et al. (2008) 41 was at the lowest risk of bias overall and 3 studies,22,39,42 were equally at the highest risk of bias overall.
Random-Sequence Generation
Three studies reported methods of randomization, using random-sequence generation and were at low risk of selection bias.38,41,43 However, the risk of bias was unclear in 3 studies due to inadequate description of randomization-sequence generation,22,37,42 and there was a high risk in 2 studies, as no descriptions were provided.39,40
Allocation Concealment
Four studies were at a low risk of selection bias for this outcome37,38,41,43 and, in 4 studies, the risk was unclear, as there were inadequate descriptions of allocation concealment.22,39,40,42
Blinding of Participants and Personnel
Two studies were at either a low 43 or unclear 37 risk of performance bias. The remaining 6 studies were at a high risk of bias due to lack of blinding for the participants as well as the personnel conducting the study.
Blinding of Outcome Assessment
Only 2 studies38,43 were at a low risk of detection bias due to blinding of the outcome assessor. One study was at an unclear risk due to inadequate description. 41 The remaining 5 studies were all at a high risk of bias due to the lack of blinding of outcome assessors.
Incomplete Outcome Data
Three studies were at a low risk of attrition bias,40,41,43 and 2 were at an uncertain risk due to inadequate reporting of outcomes.38,39 The remaining 3 studies22,37,42 were at a high risk of bias due to high, unaccounted for, withdrawals from the studies.
Selective Reporting Bias
As there were no clear protocols referenced in any of the studies, it remains unclear whether studies reported were reported selectively or not. All studies were rated as being at an unclear risk of bias.
Other Bias—Selection Bias
Studies reported selected patient groups, with most including only low-risk healthy women, with no predisposing factors or complications of pregnancy, therefore they were at an unclear risk of selection bias. Only 2 studies reported including all women presenting with the condition in the inclusion criteria.37,42 See Figure 2.
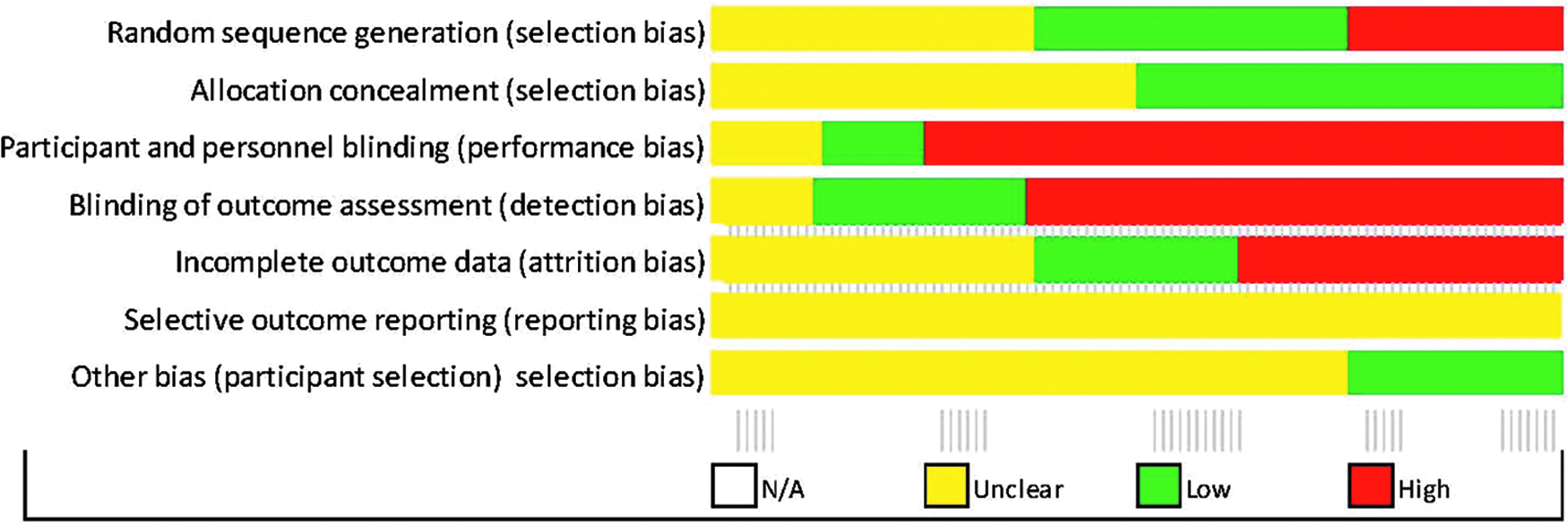
GRADE [Grades of Recommendation, Assessment, Development, and Evaluation]. Risk of bias in included studies. N/A, not applicable.
Discussion
This review examined RCT trials of penetrating acupuncture that used forbidden points prior to 37 weeks of pregnancy to treat pregnancy-related pain conditions as part of the studies' treatment protocols. The primary outcome of this review was incidence of PTC. Overall, few trials reported on the primary outcome of PTC, with 2 studies reporting 6 women who withdrew from trials due to PTC. Overall, there were 35 reported births during the study periods, wherein 32 were preterm, and, for 3, the gestation was not reported.
Ongoing concerns are raised by both traditional and medical acupuncturists about the use of forbidden points during pregnancy and the risk of PTC. The research literature suggests that they are not seen as severe adverse events in terms of miscarriages or premature births, however; these contractions are distressing to women and have the potential to limit practice.
The evidence suggests that segmental acupuncture points, including forbidden points, are common in research protocols, as was seen in this review. However there was little evidence of reference to the guiding treatment principles of TCM. This suggests that medical acupuncturists are using acupuncture from a different framework and might have dismissed forbidden points as not being relevant. Yet in the literature, there are reports of PTC. While the incidence of PTC remains uncertain according to this examination of the current evidence, highly selected patient populations, rates of dropouts, and lack ITT analyses, as well as underreporting of this outcome, might have introduced significant biases into the studies, limiting their validity and the generalizability of their findings. Other research demonstrated their use of forbidden points for augmenting labor, 19 and the points have been reported to stimulate uterine contractions and study withdrawal when used for cephalic versions of breech-presenting babies. 44
While forbidden points were selected in these medical acupuncture research protocols, within a TCM framework, these points are not considered to be essential for clinical practice and women have reported clinically meaningful reduction of their lower-back pain/pelvic pain without the use of these points. 11 Within a TCM framework, the use of these points is performed with knowledge and philosophical understanding to guide the treatment. 16
When considering risk factors in patient populations, it could also be relevant that these points are used with an appropriate rationale after 36 weeks. This may be particularly relevant for women presenting with histories of an incompetent cervixes, previous preterm deliveries, previous precipitate labor, twin pregnancies, or medical complications, such as polyhydramnios for which medical management is required at the onset of labor. Consideration of the presenting problem and TCM pattern of the person is essential when applying acupuncture protocols.
Generally, studies included in this review did not report adequately on outcomes, such as adverse events, reasons for dropping out of the studies, and losses to follow-up, as well as not describing these in sufficient detail to determine the level of evidence for the safety of acupuncture at points that are generally contraindicated during pregnancy. Additionally, the population included in the studies, wherein inclusion and exclusion criteria apply—and from which the study inferences were made—do not necessarily reflect the general population of women who experience back, pelvic, or other pain during pregnancy, with other factors that may increase risk of PTC.
In view of the reported incidences of PTC and the quality of evidence in studies to date when used, the routine use of forbidden points to treat pregnancy related pain conditions before 37 weeks of pregnancy is questionable.
Conclusions
PTC is an important clinical outcome and should be reported routinely as it has a significant impact on clinical practice. The strength of evidence to date is insufficient to recommend using forbidden points prior to 37 weeks of pregnancy. Highly selected patient populations, risk of bias in study designs, and participant withdrawal rates suggest that high-quality trials are required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors have received no funding to conduct this review.