
Abstract
Objective:
Acupuncture continues to gain popularity as a first treatment option for a variety of conditions; however, an in-depth understanding of the relationships between the acupoints and the underlying anatomy of the human body is often unclear. This article updates the anatomical relationship between facial acupoints and the trigeminal nerve (CN V) and contrasts the results against the standard textbook Chinese Acupuncture and Moxibustion.
Methods:
A literature review, cadaver dissection, and a neuroanatomical stimulation of the CN V was conducted, focusing on the anatomical locations of the acupoints along the CN V on the face and nerve block targets. The results were contrasted against the standard acupoint location and nerve targets described in Chinese Acupuncture and Moxibustion.
Results:
The present article classifies CN V acupuncture targets according to 4 different types: (1) trunk; (2) bifurcation; (3) branch; and (4) anastomoses. The results of this exploration highlight the specificity with which acupoints are located in relation to the CN V. Areas of high nerve density correspond to several acupoints. Consequently, acupoints overlay closely with CN V branches as they emerge and bifurcate on the face.
Conclusions:
There is a clear and neuroanatomically relevant relationship between facial acupoints and the CN V.
Introduction
Acupuncture is an ancient medical practice that is gaining popularity as a minimally invasive treatment. 1 The body of evidence-based research continues to grow, with 117 conditions currently recognized for treatment. 2 As acupuncture continues to expand as a first-line treatment modality, a deeper and more-accurate understanding of the acupoints' anatomical target(s) is necessary to achieve reproducible clinical results.
At present, the practice of acupuncture focuses on specific and generally accepted therapeutic effects of the acupoints; however, modern anatomy is generally not described or emphasized during acupuncture education. This lack of anatomical education in acupuncture practice creates difficulty in developing consistent and reliable results in practice and in clinical research trials.
When acupuncture texts, such as Chinese Acupuncture and Moxibustion, describe acupoint anatomical targets, these ting in misleading treatment targets and nonreproducible clinical results. 1 The Extra points, not associated with a meridian, are not discussed when anatomical targets are explored, leaving a significant gap in understanding and decreasing the potential for positive treatment results. This inaccuracy takes away from acupuncture's utility, creating skepticism within the broader medical community.
The trigeminal nerve (CN V) is the largest of the 12 cranial nerves. The CN V transmits sensory input from the face and head and provides motor innervation to the muscles of mastication through its 3 subdivisions: ophthalmic (V1); maxillary (V2); and mandibular (V3) (see Diagram later in this article).
There are more than 100 acupoints located on the head, and a thorough understanding of the relationship between these acupoints and the CN V will be useful in the development of minimally invasive treatments for CN V disorders. Although research does exist regarding the correspondence of facial acupoints to the CN V, standards and detailed descriptions of the relationships have not been developed fully.3,4
Trigeminal neuralgia, also known as tic douloureux, is a painful neurologic disorder characterized by recurring brief attacks of paroxysmal, severe shocklike pain that can be distributed between 1 or more branches of the CN V. Trigeminal neuralgia more-commonly occurs in the elderly population (ages 60–70).5–7 In China, acupuncture is a common treatment for trigeminal neuralgia, with promising results; however, treatment protocols and acupoint–nerve targets have not been standardized. 8
As the population continues to age, minimally invasive treatments for neurologic conditions will become essential for maintaining that population's health. Acupuncture has the potential to become a standard treatment after a thorough understanding of the relationship between the CN V and the acupoints of the face is achieved.
To this end, the present article updates the anatomical relationship between the acupoints of the face and the CN V and contrasts the results against the standard acupuncture text (i.e., Chinese Acupuncture and Moxibustion 1 ). Understanding the unique anatomical specificity of the acupoints helps standardize the needle targets during treatment of CN V disorders to allow for reproducible results for clinical and research purposes.
Methods
Defining the Areas of the Face
For this literature review, the face was defined as the area included within the boundaries of the anterior and lateral hairlines, from the preauricle region to the mandibular angle, and down to the tip of the chin. One exception is the deep temporal nerve. It innervates the temporalis muscle that moves the mandible, which is within our definition of the face.
Many acupoints on the face have also been excluded from the present review, as they correspond more-accurately to the facial nerve (CN VII) and will be described in a future article.
Literature Review
Anatomical descriptions and dissections of the CN V were summarized from medical, surgical, and plastic-surgery journals, with a special focus on anesthesia targets. Standard acupoint locations were sourced from Chinese Acupuncture and Moxibustion. 1 For the purpose of acupoint location comparison to modern anatomy, the cun measurement must be considered. A cun is a proportional measurement (it can be scaled to any body size) but generally can be converted to modern measurements, generally described as the width of the person's thumb ∼1 inch.
When possible, nerve targets were crossreferenced with Gray's Anatomy.9,10 In some cases, the anatomical targets have been purely described based on Gray's Anatomy.
Dissection Notes
A single cadaver dissection was performed to highlight the anatomical specificity of the acupoints in relation to the CN V. The specimen was an 88-year-old female acquired for anatomical dissection via the Human Body Donation Program at Queen's University, in Canada. The dissection was completed at the Anatomy Learning Center in Queen's University as part of the Complementary & Alternative Medicine—Human Dissection Experience Program.
The specimen was fixed with vascular perfusion, using a mixture of liquid phenol, 95% ethanol, glycerin, and water.
Neuroanatomical Stimulation
Acupoint location was superimposed on CN V anatomy and the relationship was examined to determine the unique anatomical target of each acupoint. When a detailed nerve terminus was not dissected, a Pointer Plus device (a 10-Hz monopolar electrostimulation device manufactured by Mayfair Medical Supplies Ltd., Hong Kong) was applied for the electrical stimulation of CN V innervation targets in order to describe the nerve course.
Unique anatomical nerve targets were described whenever a discrepancy or neuroanatomical redundancy was identified in Chinese Acupuncture and Moxibustion. 1 For these acupoints, a new neuroanatomical target was provided based on correspondence between acupoint location and CN V trajectory.
Results
Results from the literature review and dissection studies are presented in Table 1. The modern acupoint locations, according to Chinese Acupuncture and Moxibustion, 1 were used as the benchmarks for acupoint locations. The standard nerve targets as described by Chinese Acupuncture and Moxibustion 1 were contrasted with the reinterpreted nerve targets in relation to the anatomical nerves/nerves-block locations.
Comparison of Chinese Acupuncture and Moxibustion a Versus Reinterpreted Neuroanatomical Targets of the Trigeminal Nerve Branches Based on Modern Acupoint Locations
Cheng 1
Not listed.
Table 1 is as a quick reference guide for clinical practice and research to improve treatment standardization and outcomes.
Diagram
The following diagram shows how Figures 1, 2, and 3 illustrate the 3 divisions11–13 of the CN V:


Fig. 1A: frontal V1 points + nerves
Fig. 1B: lateral V2 points + nerves + schematics
Fig. 1C: dissection photo (composite)
Discussion
The CN V has an extensive branching pattern over the head and face. 11 The above Diagram highlights the branching pattern of the CN V and provides an overlay of associated acupoints of the face.
Ophthalmic Division (V1)
The ophthalmic division (V1) of the CN V innervates the forehead, portions of the nose and eye, the sphenoid sinus, and areas within the cranium, including the dura mater. 11 Despite being the smallest division of the CN V, this division's nerve branches have strong anatomical relationships to the acupoints of the face.
Ex-HN8 (Bi Tong)
Ex-HN8 (Bi Tong) is one of the Extra acupoints of the face (see Diagram), located at the superior end of the nasolabial groove. The external nasal branch of the anterior ethmoidal nerve (V1) emerges onto the face at the lower border of the nasal bone. Nerve block is achieved through injection over the periosteum at the junction of the bone nasal and cartilaginous parts of the nose on either side of the midline.14,15
Ex-HN8 (Bi Tong) is located just lateral to the emergence of the external nasal branch of the anterior ethmoidal nerve (V1; Fig. 1B). The external nasal branch of the infraorbital nerve (V2) emerges onto the face in proximity to the location of Ex-HN 8 (Bi Tong); however, it relates more closely to the location of LI 20 (Ying Xiang), as discussed below (Fig. 2B).
Unique anatomical targets are essential for standardizing needle targets, and Ex-HN 8 (Bi Tong) was mapped to the external nasal branch of the anterior ethmoidal nerve to remove redundancy imposed on the external nasal branch of the infraorbital nerve (V2). The current authors posit that Ex-HN 8 (Bi Tong) is located more accurately at the emergence of the external nasal branch of the anterior ethmoidal nerve (V1) onto the nose, rather than at the end of the nasolabial fold. The angle of needle insertion associated with Ex-HN 8 (Bi Tong) is typically in a superior direction along the bridge of the nose, in the direction of the emergence site of the external nasal branch of the anterior ethmoidal nerve.
Ex-HN 4 (Yu Yao)
Ex-HN4 (Yu Yao) is an Extra point located in the middle of the eyebrow. When the eye looks straight ahead, the point is in line with the pupil. The supraorbital nerve (V1), a branch of the frontal nerve (V1), exits the orbit and emerges onto the face via the supraorbital foramen/notch.16,17 This notch is palpable approximately at the middle of the eyebrow.
Generally, the vertical line delineated by the pupil approximates the center of the eyebrow. Based on this location, it can be inferred that the anatomical target of Ex-HN 4 (Yu Yao) is the supraorbital nerve trunk (V1) within the supraorbital notch (Fig. 1C). 3 Before needling Ex-HN 4 (Yu Yao), the supraorbital notch must be palpated to ensure that the nerve is targeted properly during treatment. Palpation, rather than the vertical line from the pupil, is the preferred method for locating Ex-HN 4 (Yu Yao). This vertical line does not account for anatomical variation of the supraorbital notch location and would therefore be a less-accurate way to locate the neuroanatomical target associated with this point.
BL 2 (Qu Chai)
BL2 (Qu Chai) is located at the medial end of the eyebrow, in the supraorbital notch. It is of particular interest that the location of BL 2 (Qu Chai) is described in Chinese Acupuncture and Moxibustion 1 as the supraorbital notch at the medial end of the eyebrow, given that this notch is located at the midpoint of the eyebrow.17,18 A frontal notch, located between the trochlea and the supraorbital foramen, was described as the exit point of the supratrochlear nerve.9,10 This frontal notch could be confused easily with the supraorbital notch associated with Ex-HN 4 (Yu Yao).
The frontal notch is not always anatomically present; however, the supratrochlear nerve (V1) exits the orbit at the medial corner of the eye and travels upward along the forehead, parallel and medial (∼ 1 cm) to the supraorbital nerve, indicating that the supratrochlear nerve (V1) is the unique anatomical target of BL 2 (Qu Chai).3,16,17
Chinese Acupuncture and Moxibustion 1 describes BL 2 (Qu Chai) as targeting the medial branch of the frontal nerve (i.e., the medial branch of the supraorbital nerve), which branches from the main nerve trunk shortly after leaving the supraorbital foramen. Anatomically, the supraorbital nerve (V1) was associated with Ex-HN 4 (Yu Yao) and cannot be associated with BL 2 (Qu Chai), as these acupoints occupy distinct locations along the eyebrow (Fig. 1C). The emergence of the supratrochlear nerve from the orbit (see Diagram) best corresponds to the location of BL 2 (Qu Chai). 18
Maxillary Division (V2)
The maxillary division (V2) is intermediate in size relative to the ophthalmic (V1) and mandibular (V3) divisions and functions as a purely sensory division of the CN V. The maxillary division receives sensory innervation for the area around the maxillary bone, the midfacial region, lower eyelid, portions of the nose, upper lip, and the maxillary mouth and jaw. 12
ST 2 (Si Bai)
ST 2 (Si Bai) is located in the depression of the infraorbital foramen. The infraorbital nerve emerges onto the face through the infraorbital foramen.15,18
The location of ST 2 (Si Bai) corresponds exactly to the emergence of the infraorbital nerve trunk onto the face (Fig. 2C). 3 The shallow depth of needling (perpendicular 0.2–0.3 cun) for ST 2 (Si Bai) also confirms the infraorbital nerve trunk as the target. In this instance, Chinese Acupuncture and Moxibustion 1 also describes the infraorbital nerve as the target for ST 2 (Si Bai); there were no discrepancies noted.
LI 20 (Ying Xiang)
LI 20 (Ying Xiang) is in the nasolabial groove, at the level of the midpoint of the lateral border of the ala nasi. As the infraorbital nerve descends from the infraorbital foramen, the external nasal branch (V2) separates from the main trunk and anastomoses with the external nasal branch of the anterior ethmoidal nerve (V1) to innervate the area from the ala to the root of the nose.19,20
As described above, Ex-HN 8 (Bi Tong) is associated with the external nasal branch of the anterior ethmoidal nerve (V1). LI 20 (Ying Xiang) is located between Ex-HN 8 (Bi Tong) (Fig. 1B) and LI 19 (He Liao; Fig. 2B) and overlays closely with the external nasal branch of the infraorbital nerve (V2) as it reaches the nose.19,20
Chinese Acupuncture and Moxibustion 1 associates LI 20 (Ying Xiang) with the anastomotic branch of the facial (CN VII) and infraorbital nerves (V2). This part of the text describes the infraorbital plexus, which is located just below the infraorbital foramen, whereas LI 20 is located at the level of the ala nasi, much lower than Chinese Acupuncture and Moxibustion's 1 attributed neuroanatomical association. 21 The mention of the infraorbital nerve (V2), although accurate, does not reflect a unique anatomical target, and the external nasal branch of the infraorbital nerve (V2) is a more-accurate neuroanatomical location for this acupoint. 22
LI 19 (He Liao)
LI 19 (He Liao) is located directly below the lateral margin of the nostril level with DU 26 (Shui Gou), which is located at the junction of the upper third and middle third of the philtrum. The internal nasal branch of the infraorbital nerve (V2) branches as the nerve descends from the infraorbital foramen and runs superior to the depressor septi muscle, along the ala of the nose to supply the skin of the philtrum, nasal septum, and nasal vestibule.19,20
LI 19 (He Liao) and LI 20 (Ying Xiang) are located close together (Fig. 2C). Assuming unique anatomical targets for the acupoints, having 2 acupoints located close together indicates that there is a dense branching pattern of the nerves in the vicinity. This was made apparent by dissections of the infraorbital nerve. 20 LI 19 (He Liao) is located close to the nostril and the innervation pattern of the internal nasal branch to the lower portion of the nose corresponds to the location of LI 19 (He Liao).
Chinese Acupuncture and Moxibustion 1 describes LI 19 (He Liao) as targeting the anastomotic branch of the facial nerve (CN VII) and infraorbital nerve (V2), which is the same description as for LI 20 (Ying Xiang). These descriptions are redundant and imprecise.
Summary: LI 19 (He Liao), LI 20 (Ying Xiang), and Ex-HN 8 (Bi Tong)
When LI 19 (He Liao), LI 20 (Ying Xiang), and Ex-HN 8 (Bi Tong) are examined together (see Diagram), the reinterpreted nerve targets show the specificity of the acupoints and the sophistication of anatomical knowledge at the time the acupoints were described. It is not a coincidence that the acupoints were located with this specificity. These 3 unique anatomical targets allow for improved study and treatment outcomes associated with these acupoints. This triad of points highlights the importance of a detailed understanding of the unique anatomical targets associated with acupuncture points.
GB 1 (Tong Zi Liao)
GB 1 (Tong Zi Liao) is located lateral to the outer canthus in the depression on the lateral side of the orbit. The zygomatic nerve bifurcates within the orbit forming 2 branches: the zygomaticotemporal and the zygomaticofacial nerves. The zygomaticofacial nerve (V2) emerges onto the face via a foramen in the zygomatic bone lateral to the orbit, whereas the zygomaticotemporal nerve (V2) emerges through a foramen above the zygomatic arch and posterior to the orbit.9,10,12,21
It is common for acupoint names to describe an anatomical feature of the body, providing a reference to the acupoint location. 1 GB 1 (Tong Zi Liao) translates as “pupil bone hole.” Bone holes are generally considered to be foramina. This is of relevance, considering that the zygomaticofacial nerve (V2) passes through a foramen to emerge onto the face. The zygomaticofacial foramen is the main foramen located lateral and inferior to the orbit (Fig 2D). The zygomaticotemporal foramen is located superior to the zygomaticofacial foramen.9,10
Chinese Acupuncture and Moxibustion 1 associates GB 1 (Tong Zi Liao) with the zygomaticofacial nerve, zygomaticotemporal nerve, and temporal branch of the facial nerve. Considering that these nerves emerge onto the face at unique locations, it is unreasonable to assume they could all be the anatomical target of GB 1 (Tong Zi Liao).
Considering the relationship between GB 1 (Tong Zi Liao) and the other acupoints around the eye (see Diagram) and their corresponding nerve exit points, it is unlikely that GB 1 (Tong Zi Liao) would be mapped to a neuroanatomically insignificant location (i.e., just lateral to the outer canthus of the eye). 1 It would appear the location of GB 1 (Tong Zi Liao) drifted from its intended bone-hole position and therefore should be reanchored to the zygomaticofacial foramen to target the zygomaticofacial nerve (V2).
Mandibular Division (V3)
The mandibular division (V3) of the CN V is the largest nerve branch, providing both sensory and motor innervation to the lower one-third of the face. Sensory innervation is received from the lower teeth and gingiva of the mandible, the skin of the temporal region, and the anterior two-thirds of the tongue. Motor innervation is provided to the muscles of mastication. 13
ST 7 (Xia Guan)
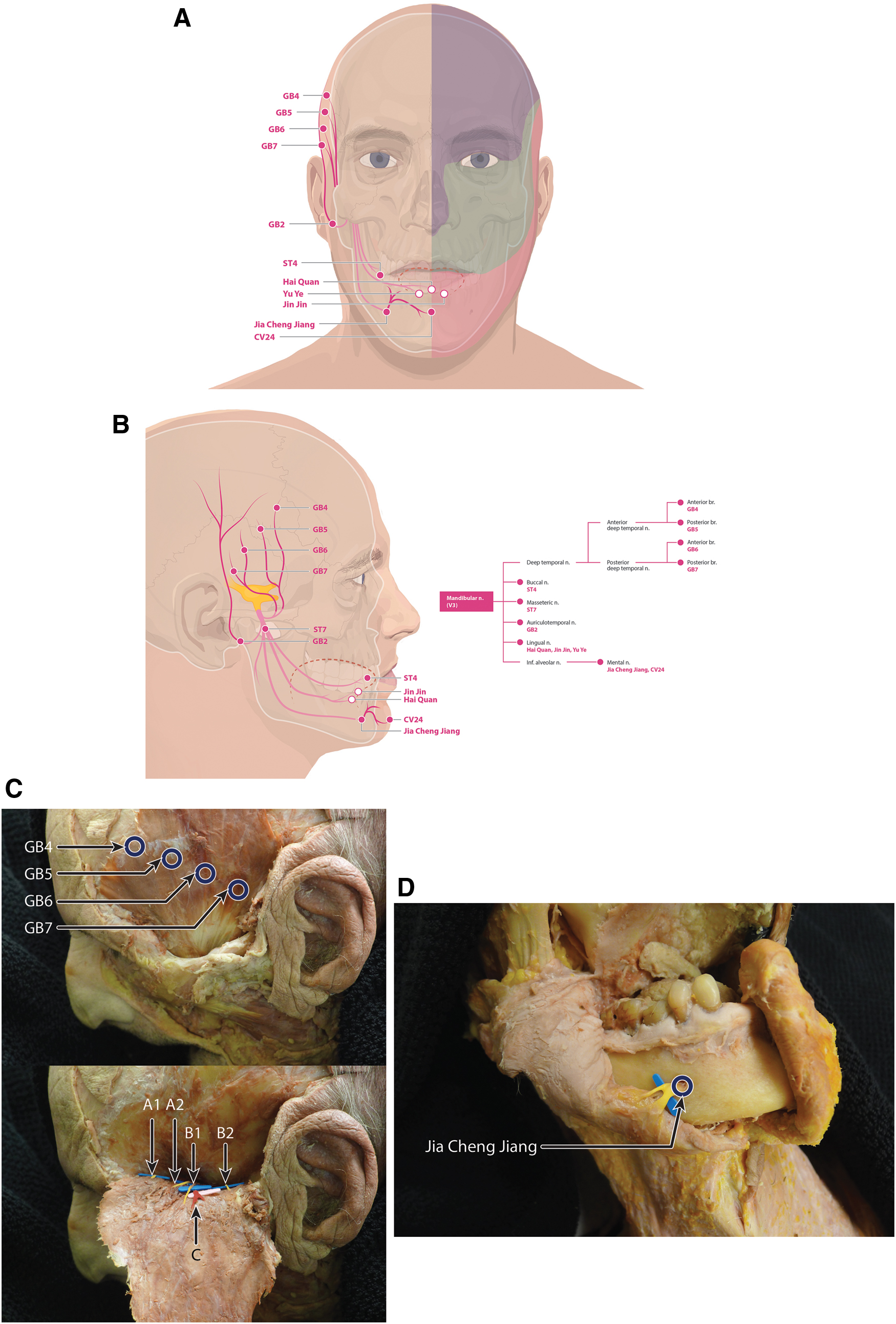
ST 7 (Xia Guan) is located in the depression at the lower border of the zygomatic arch, anterior to the condyloid process of the mandible. The masseteric nerve branches from the mandibular nerve (V3) within the mandibular notch (Fig 3B). 23
The depression at the lower border of the zygomatic arch is the mandibular notch, which corresponds to the emergence of the mandibular nerve. The location of ST 7 (Xia Guan) corresponds exactly to the access point of the masseteric nerve. Superficial needling will target the masseteric branch. At a deeper depth, within the mandibular notch, the mandibular nerve trunk (V3) can also be targeted during treatment.
Chinese Acupuncture and Moxibustion 1 describes ST 7 (Xia Guan) as relating to the zygomatic branch of the facial nerve and branches of the auriculotemporal nerve. The zygomatic branch of the facial nerve (CN VII) passes superior to the mandibular notch and cannot be accessed reliably via the location of ST 7 (Xia Guan).9,10 The auriculotemporal nerve (V3) is best accessed at the anterior margin of the upper helix of the ear, 17 which also confirms that this nerve is an inaccurate target for ST 7 (Xia Guan).
Overview: GB 4 (Han Yan), GB 5 (Xuan Lu), GB 6 (Xuan Li), and GB 7 (Qu Bin)
The deep temporal nerve divides into anterior and posterior branches and follows a diagonal line from the root of the helix toward the angle form by anterior and lateral hairlines. This nerve-branching pathway along the anterior border of the temporalis muscle parallels the described course of the acupoints GB 4 (Han Yan), GB 5 (Xuan Lu), GB 6 (Xuan Li), and GB 7 (Qu Bin). 1
Chinese Acupuncture and Moxibustion 1 describes GB 4 (Han Yan), GB 5 (Xuan Lu), GB 6 (Xuan Li), and GB 7 (Qu Bin) as associated with the temporal branch of the auriculotemporal nerve (Table 1). The course of the auriculotemporal nerve is closely related to that of the superficial temporal artery, which traverses a straight path along the temporalis muscle toward the top of the head. 16 This course does not overlay with the diagonal distribution drawn between ST 8 (Tou Wei) and GB 7 (Qu Bin); the deep temporal nerve approximates this line better. The branching pattern of the deep temporal nerve (DTN) shows a high density of nerve branches (Fig. 3C), corresponding to the proximity of the Gall Bladder points along the line between ST 8 (Tou Wei) and GB 7 (Qu Bin). 24 In contrast, the temporal branch of the auriculotemporal nerve does not show this branching pattern.
There is a neuroanatomical redundancy of associating these 4 acupoints with the temporal branch of the auriculotemporal nerve. This redundancy does not consider the specificity with which the acupoints of the head were described and thus is not the appropriate nerve target associated with these points.
GB 4 (Han Yan)
GB 4 (Han Yan) is located within the hairline of the temporal region, one-quarter of the distance between ST 8 (Tou Wei) and GB 7 (Qu Bin). The anterior deep temporal nerve (ADT), a branch of the DTN (Fig. 3B), enters the anterior (deep) aspect of the temporalis where it branches into 2 divisions: anterior and posterior. 24 The anterior branch supplies the anterior two-thirds of the temporalis muscle. Dissection work, tracing along the course of the deep temporal nerve, shows a close overlay to the modern location of GB 4 (Han Yan).
GB 5 (Xuan Lu)
GB 5 (Xuan Lu) is located within the hairline of the temporal region, midway along the line connecting ST 8 (Tou Wei) and GB 7 (Qu Bin). The posterior branch of the ADT (see GB 4, Han Yan) supplies the posterior one-third of the temporalis muscle and divides from the nerve trunk inferior to the anterior branch of the ADT. 24
The dissection work, tracing along the course of the deep temporal nerve, shows a close overlay to the relationship between the anterior and posterior branches that relates closely to the modern locations of GB 4 (Han Yan) and GB 5 (Xuan Lu). 24
GB 6 (Xuan Li)
GB6 (Xuan Li) is located within the hairline of the temporal region, midway between GB 5 (Xuan Lu) and GB 7 (Qu Bin). The posterior deep temporal nerve (PDT), a branch of the DTN, passes along the lateral pterygoid to enter the posterior deep surface of the temporalis muscle, where the PDT divides into 2 branches: anterior and posterior. The anterior branch of the PDT supplies the anterior portion of the posterior temporalis muscle. The path of the branch matches the location of GB 6 (Xuan Li) closely. 24
GB7 (Qubin)
GB 7 (Qu Bin) is located within the hairline of the temporal region, anterior and superior to the auricle, and level with, and roughly a finger's breadth, anterior to TE 20 (Jiao Sun). TE 20 (Jiao Sun) is located directly above the ear apex within the hairline. The PDT posterior branch innervates the posterior portion of the posterior temporalis muscle. The posterior branch of the PDT divides inferior to the anterior branch and is located just anterior to the auricle, aligning with the modern location of GB 7 (Qu Bin). 24
Trigeminal Neuralgia
In trigeminal neuralgia, the maxillary (V2) and mandibular (V3) divisions of the nerve are most commonly affected.5,25 Considering the specificity with which the CN V can be targeted with acupuncture, the potential to develop standardized treatment protocols is significant.
There are various theories regarding the causes of trigeminal neuralgia. The most common theory focuses on demyelination of the CN V and vascular compression of the nerve route. 26 Acupuncture research is now exploring how acupuncture can improve circulation during treatment. 26 Although the deep nerve roots cannot be reached easily, with the exception of the mandibular trunk (V3) at ST 7 (Xia Guan), that acupuncture might improve the circulation within the peripheral and symptomatic branches of the CN V warrants further exploration.
The potential for acupuncture to improve treatment outcomes for neurologic conditions is promising, as a greater understanding of how the acupoints map to neuroanatomical locations will lead to the standardization of needle targets and improvements in patient outcomes.
Conclusions
The results of the current explorations suggest that the examined acupoints map to unique neuroanatomical locations and enable access to treatment of conditions affecting the CN V branches on the face. Following the guidelines presented here for neuroanatomical correspondence of the acupoints will help standardize acupuncture treatments.
Currently, there is insufficient detailed dissection research regarding the trajectory of the CN V on the scalp. The current authors hypothesize that, as further dissection work is completed regarding the course of the CN V within the scalp, unique anatomical nerve targets will emerge for the corresponding acupoints.
The field of electrostimulation serves as an exciting platform to explore how nerves are affected when targeted accurately by acupuncture treatment and to confirm the nerve–acupoint relationships described here.
Footnotes
Author Disclosure Statement
No financial conflicts exist.
Funding Information
No funding was received for this article.