
Abstract
Background:
The Varicella-zoster virus (VZV) remains dormant in the dorsal root ganglia and can become reactive later in a person's life. Factors such as stress, trauma, chronic disease, systemic illness, immune disorders, and age-related decline in host immunologic responses can potentially incite reactivation. Activation of VZV resulting in shingles following acupuncture has been reported in the literature previously, and some mechanisms have been proposed for this observation.
Case:
A patient with a history of total thyroidectomy for thyroid cancer presented with chronic neck pain. She was clinically and biochemically in a euthyroid state and on thyroid replacement therapy. She had a history of chickenpox, at age 13, and seasonal allergies. After her first acupuncture session, she received an allergy shot for her seasonal allergies. A day after the procedure, she developed a vesicular rash and was subsequently diagnosed with acute Herpes zoster. Subsequent acupuncture was withheld following this event. She received acyclovir and applied topical Aloe vera to the cutaneous lesions, and developed mild scarring, but did not experience postherpetic neuralgia.
Conclusions:
Acupuncture is a minor trauma that can predispose a patient to reactivation of VZV and shingles in the setting of immune activation with allergen immunotherapy.
INTRODUCTION
Herpes zoster (HZ), also known as zoster and shingles, is caused by reactivation of the Varicella-zoster virus (VZV), the same virus that causes varicella or chickenpox. Almost 1 of 3 persons in the United States develops shingles in his or her lifetime, with an estimated 1 million cases each year. In England and Wales, there are ∼50,000 cases of shingles in people ages 70 or older every year, and it is estimated that ∼50 of these cases result in death. About 1 in 4 adults will experience shingles in his or her lifetime 1 . The estimated global incidence using data from prospective surveillance, electronic medical records, and administrative data reviews in 7 countries in North America, Europe, and Asia–Pacific show an incidence ranging from 3–5/1000 person-years.2. Once varicella illness resolves, the virus remains dormant or latent in the dorsal root ganglia. VZV can reactivate late in a person's life, traveling to the dermatome corresponding to its ganglion, producing the typical painful, maculopapular rash. Factors, such as stress, trauma, chronic diseases, systemic illnesses, immune disorders, and age-related declines, in host immunologic responses can potentially induce reactivation.3,4
CASE
A middle-age acupuncture-naïve woman presented for acupuncture because of an insidious onset and progression of chronic neck pain following a total thyroidectomy and external beam radiation for treatment of thyroid cancer 20 years prior for papillary thyroid cancer, classical variant (stage I, pT3N1aMx). Her pain was bilateral, characterized as tight and achy without associated neurologic or constitutional symptoms. X-ray imaging showed that the area was normal with minimal multilevel degenerative spondylosis; magnetic resonance imaging of her shoulder showed mild acromioclavicular joint osteoarthritis. She had a history of seasonal allergic rhinitis triggered by tree pollen, mold, and seasonal allergens. She had been infected with VZV and developed chickenpox at age 13. Her current daily medications included 0.15 mg of levothyroxine, 0.25 μg of calcitriol, and 750 mg of calcium carbonate.
During her initial acupuncture assessment, she rated her pain intensity at a 5/10 using the 1–10 numeric rating scale. (NRS). On examination, slight thoracic dextroscoliosis (T-4–T-6) was observed with resulting tightness bilaterally in the iliocostalis, spinalis, and longissimus cervicis. Sternocleidomastoid, trapezius, levator scapula, splenius capitis, and rhomboid minor and major muscles were also noted to be tight. She had restrictions in active cervical lateral flexion and rotation.
After obtaining written informed consent for the procedure, the skin overlying the selected points was disinfected with an alcohol swab. Sterile disposable Peace brand (China) 1” 40 gauge/0.16-mm and 1.5” 36 gauge/0.20-mm were inserted in acupuncture points selected for their classical indications and orthopedic tendinomuscular associations. Needles were placed in the following locations: BL-60 (perpendicular insertion at 0.25”); BL-43, BL-44, BL-45, and BL-46 (oblique insertion at 0.5”–0.75”); GB-20 (oblique insertion at 0.5”); GB-21 (posterior perpendicular oblique insertion at 0.5”–75”); SI-15 (oblique medial insertion at 0.5”); SI 16 (perpendicular insertion at 0.25”); GV-14 (perpendicular superior oblique insertion at 0.25”); and on Hua Tuo Jia Ji M-BW-35 paravertebral points from C-4 to T-4 (oblique insertion at 0.25”–0.75”).
The depth of each insertion was chosen according to the patient's anatomical features and Traditional Chinese Medicine (TCM) descriptions of indications. No manual stimulation was provided. Needles were retained for 15 minutes. These were removed without incident and a sterile cotton ball was applied to the sites. The patient tolerated the procedure well, reported a postprocedure pain reduction to 2/10 on the NRS and an improved range of motion. Postprocedure counseling included instructions to continue on an anti-inflammatory diet, a daily walking program, strength training 2–3 days per week, practicing relaxation breathing, and taking 400–600 mg/day of magnesium glycinate based on notes from the referring physician. She was also informed that she might experience postprocedure fatigue and soreness. She received an 0.5-cc allergen immunotherapy (AIT) maintenance injection that was administered a few hours after her acupuncture session.
RESULTS
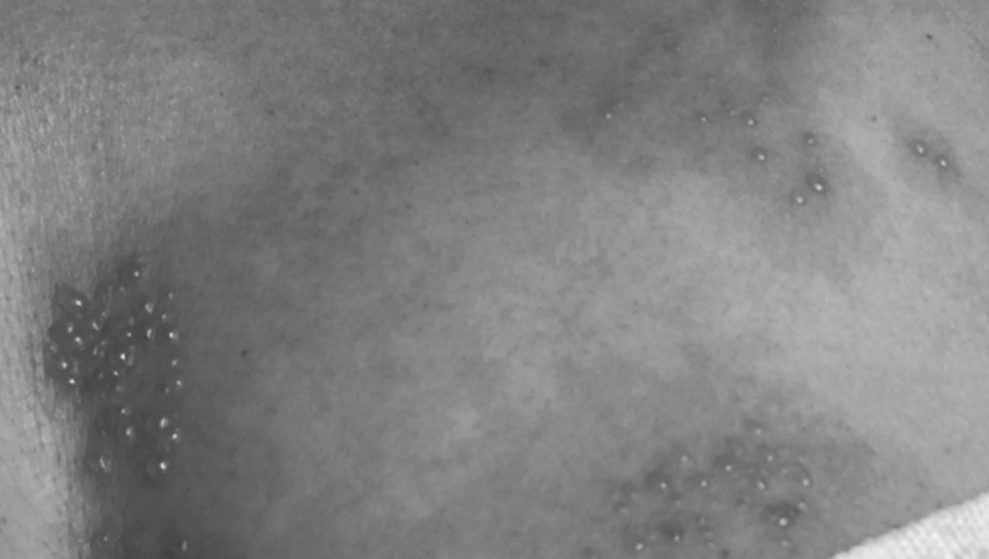
The following day, the patient began to notice a nonpainful rash on her left upper-back and chest wall, as shown in Figure 1. She was unsure if this was associated with pruritus. Two days after, she noted a painful erythematous vesicular rash on the anterior chest wall, along the left sternal border, that progressed over a period of 5 days. Figures 1–3 show the progression over the first 2 post-acupuncture days. She immediately received acyclovir and applied topical Aloe vera gel to the lesions. These healed completely by 2 weeks, and she developed minimal scarring. She completed the course of acyclovir and did not develop postherpetic neuralgia.

Skin, back, day 1 post-acupuncture.

Skin, Left anterior chest, day 2 post-acupuncture.
Skin, left anterior chest, day 3 post-acupuncture.
DISCUSSION
Although acupuncture can be used to treat shingles, it has also been reported to precipitate this condition.5,6 Chang described, in a letter, a case in which a patient was receiving weekly acupuncture for knee pain. 6 That patient had a history of recurrent cutaneous herpes involving the skin above her left buttock for 10 years, averaging 3 episodes per year. She had received a total of 20 treatments given at weekly intervals to address her knee pain. During that course of acupuncture, she had experienced 9 recurrences of herpetic skin lesions and 2 episodes of tingling over the skin supplied by the S-1 spinal segment. The recurrences occurred almost regularly, 12 hours after each treatment. Kewish reported an observation of herpes zoster in the trigeminal nerve distribution following auricular acupuncture, specifically a standard protocol named Battlefield Acupuncture, 13 days after receiving this procedure for the treatment of low-back pain. 7
In the current case, the absence of a prodromal time period of 2–3 days and prodromal symptoms prior to the skin eruption raised the possibility that VZV reactivation occurred prior to the acupuncture and AIT sessions. However, given the previous reports of VZV reactivation related to acupuncture, it is still important to note a potential causal relationship. Two factors potentially contributed to herpes zoster reactivation in this patient, acupuncture as a form of trauma and its potential interaction with AIT. Acupuncture is a form of trauma, possibly precipitating these acute eruptions. In an age-matched case-control study using Medicare data on persons who experienced musculoskeletal and intracranial, nerve, spinal cord, and crush injuries, herpes zoster was observed 3.4 times more, compared to controls, with the greatest proportion of cases occurring 1 week after the trauma. 8 A unique feature, in the current case, was the interval incident of an allergen immunotherapy injection between the acupuncture session and the VZV reactivation, suggesting a potential association. Waning of the humoral immune response is a risk factor for VZV reactivation, and T-cells play a role in preventing reactivation. 9 An AIT mechanism of action involves modulation of B- and T-cell responses, 10 and acupuncture has also has effects on immune modulation and the nervous system. 11
CONCLUSIONS
This case provides additional clinical evidence concerning acupuncture's relationship with shingles in comorbidity. Although acupuncture as a form of trauma has been reported to be related to VZV reactivation, the contribution of a recent AIT-maintenance injection might be another precipitating factor not previously reported in the literature. At present, shingles is not commonly reported as a complication of acupuncture, in the same manner as pneumothorax or infections. In the presence of previous reports and this current report, a history of varicella or shingles should be elicited when evaluating patients for this procedure; these patients should be informed of a potential reactivation. In this susceptible group of patients, stimulation of points to enhance immune function (wei chi) should be considered, and instructions to avoid any procedures that alter immune function should be added to post-procedure counseling and education.
Footnotes
ACKNOWLEDGMENTS
The authors thank Anthony Llanos for technical support for preparation of this article.
AUTHORS' CONTRIBUTIONS
All authors participated in writing, reviewing and revising this manuscript and assume responsibility and accountability for its contents.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funds were received to support this project