
Abstract
Background:
Scar pain is a residual symptom of a wound that can cause physiologic and psychologic disorders in patients. In addition to mechanical stimulation in nociceptive fibers, pain can be caused by a neuroma—an adhesion between the layers of skin and fascia that disrupts blood flow around the scar—as well as an increase in peptidergic nerve-fiber density due to dysregulation between synthesis and degradation of collagen tissue that cause abnormal scar formation. Research has shown that ear acupuncture is effective for management of acute pain, including scar pain. Acupuncture in the local area of the scar is also effective for reducing pain significantly. The combination of these 2 therapies is expected to be effective for management of scar pain in cases that have not improved for 4 years.
Case:
A 69-year-old woman, with a history of a laparotomy 4 years ago, came to the RSCM acupuncture outpatient unit with severe pain in her stomach. The pain was located in a 30-cm long laparotomy wound that ran between the xiphoideus process and the umbilicus, and felt like a rope binding and pressing upward in the area. Manual acupuncture was given at a Battlefield Acupuncture (BFA) point, combined with acupuncture to local point on the scar.
Results:
She had with a positive vascular autonomic sign response for 30 minutes at each session. At the end of her 12th therapy session, she reported that she was pain-free and did not experience any severe side-effects.
Conclusion:
A combination of BFA with local-point acupuncture was effective in reducing the severe pain of caused by a post-laparotomy scar.
Introduction
Scar pain is a residual symptom of a wound that can cause physiologic and psychologic dysfunction in a patient. This pain can be the result of any form of surgery. 1 The prevalence of scar pain with minimal nerve damage is 10%, while in more-invasive surgeries, such as amputation and thoracotomy, the prevalence of scar pain is 30%–50%, and 6.6% of affected patients reported disturbances in their daily activities. 2
The emergence of scar pain is influenced by several things, such as surgical procedures and techniques, age, gender, and preoperative traumatic memory. 2 There are various theories about the pathophysiology of scar pain, one of which is a neuroma that occurs due to trapped neurons that are regenerating after trauma in fibrotic tissue. In addition, studies have shown that there is an impaired balance of peptidergic and nonpeptidergic fibers, where there is an increase in the density of peptidergic nerve fibers responsible for pain transmission. This is supported by research by Henderson et al., in 2005, which revealed an increase in substance P (sub-P) in 3 months post-trauma. 3 In addition, damage due to mechanical compression of nerve fibers A-δ and C was also thought to cause scar pain. 4
Researchers continue to look for effective management for scars, both prophylactic and therapeutic. Prevention of the formation of an excessive scar is a more-effective action than the treatment itself. A delay in epithelialization that exceeds 10–14 days increases the incidence of excessive scar formation. 5
Various conservative therapies currently used—including pressure garments, silicone, topical ointments or gels, and massage—reduce redness and thickness, and increase elasticity in scars. In addition, corticosteroid injections, cryotherapy, and scar tissue incision are also therapeutic options. However, the ability of these various therapies to reduce pain and itching is considered less-effective.6,7
Much research has been conducted on acupuncture for pain management, including cases of scar pain. Ear acupuncture is one of the effective acupuncture techniques for management of acute pain. 8 In addition, in cases of scar pain that do not improve with conventional therapy, intradermal needling along the scar has produced significant reductions in patients' pain. 1 A combination of both therapies is expected to work simultaneously to reduce acute and chronic pain in cases of scar-pain that have lasted for 4 years.
Case
A 69-year-old female patient with a history of undergoing a laparotomy 4 years prior, came with severe abdominal pain to the Dr. Cipto Mangunkusumo National Central Public Hospital's acupuncture outpatient unit. Since that operation had been performed, the patient began to feel pain in her laparotomy scars that felt like a rope tying and pressing upward in that area of her body. Laparotomy was performed on the indication of a fibrotic mass in the pancreas. Over time, this patient's pain became worse and interfered with her activities of daily living.
Three years later, because there was no reduction in this pain, the patient returned for a check-up. An examination showed the presence of gallbladder stones; thus, she underwent a laparoscopic cholecystectomy. However, after this second operation, she still did not experience any reduction in her pain; instead, this pain intensified.
This patient also had a history of hypertension and dyslipidemia and, to date, routinely took amlodipine (1 × 10 mg) and atorvastatin (1 × 10 mg).
On her first visit, the patient's blood pressure was 151/79 mm Hg, her pulse was 83 beats per minute, her temperature was 36°C, her respiratory rate was 16 breaths per minute, and her numeric rating scale—11 (NRS-11) was 8; she looked seriously ill. An abdominal physical examination revealed a midlevel transverse scar between the xiphoideus process and the umbilicus with a length of 30 cm and a width of 0.3cm. This scar was dark brown and prominent. When palpated, there was no muscular defending in any of her abdominal quadrants, but hard tissue was palpated along the scar area and this area was tender. There were no masses nor was her liver palpable.
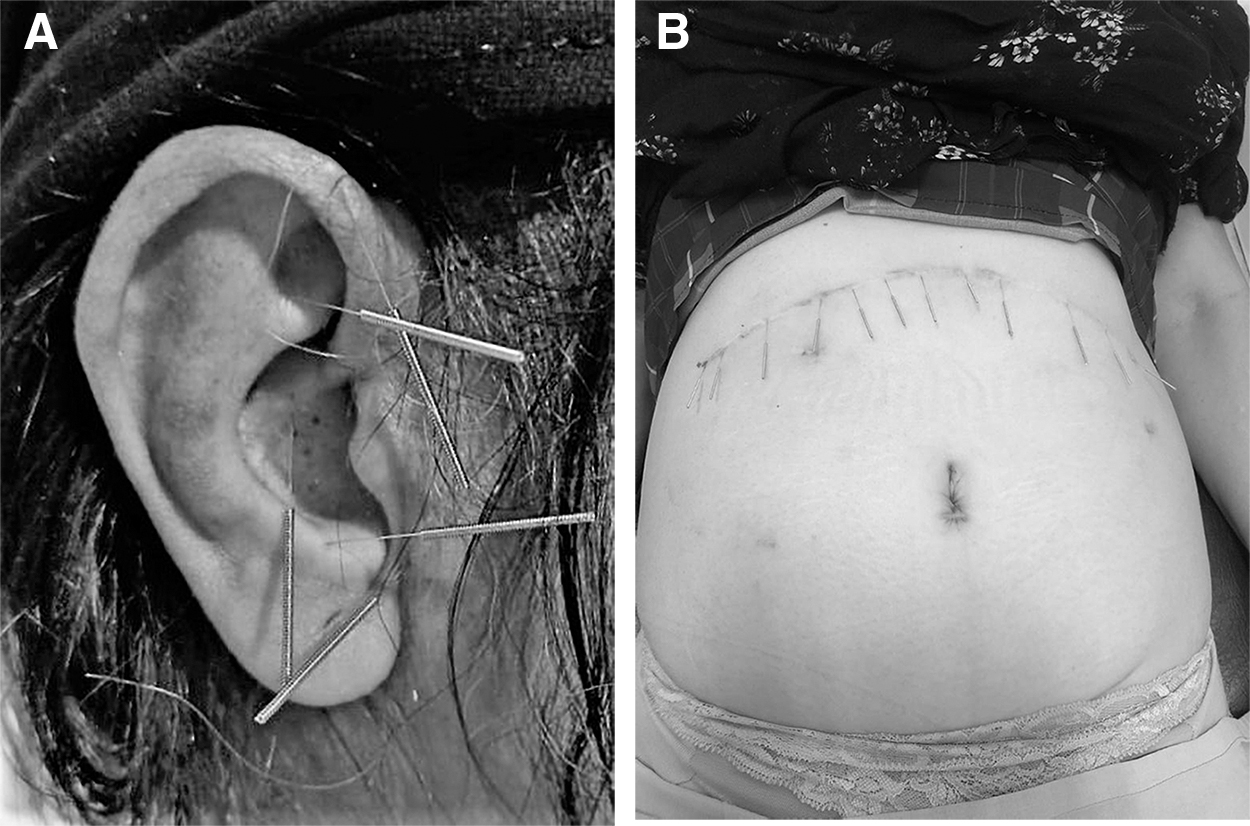
To reduce this patient's pain, acupuncture therapy using Battlefield Acupuncture (BFA) points on the ear—Cingulate Gyrus, Thalamus, Point Zero, Shen Men, and Omega 2—was performed. Additional needles were placed alongside the scar where there were positive responses to the vascular autonomic signal (VAS). This therapy was performed using a 0.15 mm × 15 mm acupuncture needle (Huanqiu®) at a 1–2 mm depth of insertion, without further manual or electrical stimulation. The goal of this therapy was reduction in NRS until the patient was pain-free.
Results
This patient underwent a total 12 acupuncture treatments over a period of 8 weeks. During the therapy sessions, the patient only felt discomfort due to the needling itself; she did not report any severe side-effects (Fig. 1 and Table 1). After the last treatment, she reported being pain-free and that she did not experience any severe side-effects.
Progress of Patient's Numeric Rating Scale (NRS)
Discussion
Wound healing, including that of surgical scars, is a complex problem involving various aspects—namely histochemistry, immunology, and molecular biology—which all play roles in cell repair and cellular factors. 9 Under normal circumstances, the density of nerve fibers will increase in the first week of wound healing and slowly decrease with time. However, in some cases, the healing response can occur more slowly and cause abnormal scars—such as keloids and hypertrophic scars—to form. 5 This occurs due to dysregulation between collagen synthesis and degradation and causes excessive proliferation of muscle-fiber cells and causes a violent local eruption, pain, itching, and functional limitations. 9
In this current case, the scar had an abnormal wound-healing process, wherein excessive collagen deposition occurred. When this occurs, the scar forms adhesions between the skin layer and fascia so that blood flow around the scar becomes disrupted and is associated with pain, itching, and hyperesthesia, which affects the patient's quality of life. Another theory is that scar pain is caused by an increase in calcitonin gene-related peptide (cGRP), as well as damage to nerve fibers A-δ and C due to mechanical compression of scar tissue. 6 In scar pain, there is an increase in peptidergic nerve fiber density (sub-P or cGRP) that responds to nerve growth factor (NGF). This results in nerve interactions that should not occur and gives rise to central plasticity, which helps cause neuropathic pain due to changes in the peripheral nervous system.2,10
After this patient's examination, the diagnosis given was scar pain. To reduce her pain, acupuncture therapy was performed at 5 BFA points and at points at local areas along the scar that had a positive VAS response. In such cases, evaluation is done by monitoring the intensity of pain in each patient. The NRS-11 is used to accomplish this. This is a pain-assessment method consisting of 11 points, for which 0 represents a pain-free condition, and 10 represents the worst-imaginable pain condition. A reduction in pain of 2 points is considered clinically significant. 11
Ear acupuncture has proven to be effective for treating acute pain. 12 BFA is an ear-acupuncture technique that has been widely used to treat pain quickly. The needling is applied sequentially at: (1) Cingulate Gyrus, (2) Thalamus; (3) Omega 2; (4) Point Zero; and (5) Shen Men. 8 Reduction of pain at the BFA points can occur significantly in minutes and can last for several hours to months. In the current case, decreases in NRS scores were reached at the end of each therapy session, and gradual decreases in NRS scores occurred at each visit, from the initial NRS score at the beginning of the first therapy until the patient had a pain-free condition at the end of the 12th session.
A randomized controlled trial using a semipermanent auricular needle (Aiguille Semi-Permanente® [ASP]) at the BFA point in patients with chronic pain showed a decrease in continuous pain on days 4 and 8. 13 ASP needles were not used in this case as they are not available at the current authors' clinic.
The mechanism of pain reduction in ear acupuncture is achieved through the release of β-endorphins, regulation of proinflammatory and anti-inflammatory cytokines, reduction of cGRP proinflammatory neuropeptides, and regulation of neurotropin NGF. 14 Opioid peptides and their receptors such as μ, δ, and κ are abundant in the raphe magnus nucleus and the caudate submedius nucleus, which are regions of the brain that form the descending inhibition system. The presence of lesions in this area causes inhibition of the effects of acupuncture analgesia. 15 A functional magnetic resonance imaging study conducted by Cho (cited by Niemtzow in 2007) showed involvement of the hypothalamus, thalamus, cingulate gyrus, and cerebral cortex in the use of the BFA technique. 16 This area is activated by opioids and cooperates in nociception modulation and that causes pain.
The analgesic effectiveness of BFA points is consistent with studies conducted by Fox et al., in 2018, which compared BFA + standard therapy with standard therapy alone in patients with low-back pain. 17 There was a significant reduction in pain in the treatment group, compared to the control group (P < 0.04), and no side-effects were reported. 17 The decrease in pain that occurred was also in line with a case report by Papadopoulos et al., in 2017, in a patient with thorax trauma who had severe chest pain that caused ventilation and oxygenation disorders. 18 The patient had significantly decreased pain scores and improvement in oxygenation and ventilation after BFA acupuncture; this effect which lasted for 5 days until the patient was transferred to the usual-care unit. 18
In the current patient, needling was also performed in the local area along the scar tissue. In such cases, the points are chosen according to the area that manifests a positive VAS response. The VAS is a vasculocutaneous reflex, wherein, if a stimulus is given to a part of the body that has an abnormality, this reflex will produce changes in the tone of arteries throughout the body. 19 In a study by Naoki et al., in a similar case, the acupuncture was performed using an intradermal needle at a point with a low pain threshold. There was a significant reduction in pain and in analgesic consumption. 1
Superficial needling is applied because the pain that occurs in the scar tissue after surgery has similar characteristics to a myofascial trigger point (MTP), so that needling at the local point is thought to inactivate the pain locally and activate antinociceptive centrally, as occurs in MTP. When this occurs, mechanisms that are thought to be related to local needling include inhibition of neural depolarization and activation of descending antinociceptive mechanisms.1,20
Reduction of tenderness in the area of the scar in the current case was accompanied by a reduction in her continuous and sharp pain that was initially felt. This was in line with research by Kotani et al., in 2001. 1 This is thought to be related to the mechanism of the gate-control theory, wherein stimulation caused by acupuncture needling will stimulate the central antinociceptive system, which will then cause the analgesic effect.
During the 12 therapy sessions, no serious side-effects were reported by this patient. Minimal side-effects—such as pain, bruising, bleeding, or swelling—were reported in a systematic review of acupuncture for management of post-traumatic scar cases by Tuckey et al. in 2019. 6
Conclusions
BFA points and local points alongside the scar produced a satisfactory reduction in the current patient's pain until she reached a pain-free condition; there were no serious side-effects. Use of press needles at the BFA points at the start of therapy can be considered to maintain the therapeutic effect. With minimal data regarding the use of acupuncture for post-traumatic scar cases, BFA points and local points alongside the scar can be considered a therapeutic option.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.
Editor Disclosure Statement
The Editor-in-Chief of Medical Acupuncture, Dr. Richard Niemtzow, is the inventor of Battlefield Acupuncture (BFA). In his capacity as an expert in BFA, he was involved with the overall review of this paper after it was peer reviewed and accepted by independent, anonymized reviewers.
Funding Information
No funding was received for this article.