
Abstract
Objective:
Evidence of effectiveness and demand for acupuncture to treat acute pain conditions is growing, as is the need for acupuncturists trained to deliver patient care in a hospital setting. This articles describes collaboration between Bastyr University and Harborview Medical Center to incorporate Doctor of Acupuncture and Oriental Medicine (DAOM) students into a trauma hospital setting.
Materials and Methods:
A model was developed to integrate DAOM students into an Anesthesiology Acute Pain Service to provide acupuncture to postoperative inpatients. That in-person model pivoted to remote student education and patient self-care education during the COVID 19 outbreak. A review was conducted of 323 consecutive patients who received acupuncture while they were hospitalized.
Results:
The review of 323 consecutive patients who received acupuncture for pain during their hospital admission indicated that as few as one acupuncture treatment resulted in clinically significant benefits. No serious complications or safety concerns were reported.
Conclusions:
Collaboration between academic and clinical programs can provide the structure to integrate acupuncture into hospital settings safely and with benefit to patients and students.
INTRODUCTION
Acute pain—from trauma, surgery, and other medical events—produces a variety of short- and long-term detrimental effects that can hamper a patient's recovery and lead to chronic pain. 1 Thus, acute pain associated with trauma and surgery demands a prompt multimodal approach, combining methods with different mechanisms of action, including pharmacologic and nonpharmacologic strategies. 2 There is growing evidence of the effectiveness and efficacy of acupuncture for addressing a wide array of acute pain conditions common in a hospital setting. Acupuncture has demonstrated benefits in cases of acute rib fractures, 3 acute low-back pain (LBP), 4 acute postoperative pain following back surgery, 5 acute migraine, 6 post-tonsillectomy pain in children, 7 and many acute pain conditions in emergency department (ED) settings. 8 A multicenter, randomized trial assessing pain relief for ED presentations of acute LBP, migraine, or ankle sprains, found acupuncture analgesia to be comparable to that of pharmacotherapy. 9 A meta-analysis showed that acupuncture reduced pain on the first day after surgery and lowered subsequent opioid use, resulting in the recommendation of acupuncture as an adjuvant therapy for treating postoperative pain. 10 Moreover, auricular acupuncture has been shown to provide additional benefits in patients with opioid-use disorder. 11
A common understanding and evidence-based rationale for acupuncture increases openness of Western medical systems toward this form of complementary and alternative medicine (CAM). Acupuncture therapy encompasses a family of procedures involving stimulation of anatomical points on the body, using a variety of techniques that may include needle insertion, manual needle stimulation, digital pressure, massage (tu'ina), magnet application, electrical stimulation, laser stimulation, cupping, and moxibustion (a warming technique). In this report, the term acupuncture refers to the method of penetrating the skin with thin, solid, flexible metallic needles that are manipulated by hand or by electrical stimulation.
Trauma and surgery can affect a person's spiritual, emotional, mental, and physical health, and may contribute to an internal imbalance of Yin and Yang and Obstruction of Qi and/or other substances, such as Blood, along pathways known as channels. A classic adage in Chinese Medicine states: “Where there is Stagnation, there is pain.” Accordingly, Qi and Blood may be unblocked by using acupuncture at certain points along the channel lines. 12 Acupuncture has been shown to produce a variety of biologic responses locally and systemically, including effects on noradrenaline, epinephrine, and the endogenous opioid system. 13 The analgesic and anti-inflammatory effects of acupuncture have also been linked to nonopioid neuropeptides including Substance P, vasoactive intestinal peptide, and calcitonin gene-related peptide. 14 Acupuncture induces activations in multiple brain networks, affecting sensory, affective, cognitive, and autonomic functions. 15
Acupuncture is accepted by a majority of hospitalized patients receiving acute care. 16 Integration of CAM in academic medical centers is on the rise through collaborations utilizing existing frameworks, 17 although protocols and service-delivery models vary according to institutions. Cross-agency collaborative education projects are often designed to teach nurses and physicians how to provide auricular acupuncture. 18 Although medical center–affiliated training sites for acupuncturists may be common in clinic or ambulatory settings for patients with chronic pain, the current authors were unable to find any literature about U.S. program collaborations that utilize hospitalized patients with acute postoperative and trauma pain for acupuncturist education. Integration models that link 2 organization's cultures and medical approaches help achieve visibility and acceptance of acupuncture within hospital settings and provides opportunities for learning. 19
MATERIALS AND METHODS
Bastyr Doctor of Acupuncture and Oriental Medicine Program
The Doctor of Acupuncture and Oriental Medicine (DAOM) is a 2-year postgraduate clinical doctorate that prepares acupuncturists to deliver specialized pain management in integrative care settings. Bastyr University—based in, Seattle, WA, USA—is a nonprofit, private university that is at the forefront of developing leaders in natural health arts and sciences, with U.S. campuses in San Diego, CA, and Kenmore, WA. Bastyr's DAOM program is accredited under applicable standards by the Accreditation Commission for Acupuncture and Oriental Medicine (ACAOM). Drawing on Traditional Chinese Medicine (TCM)and biomedical concepts, the program combines theory and practice in hands-on internships, clinical theater, case reports and discussions, preceptorships, and a capstone research project to help students gain skills to treat patients in pain and to collaborate across health care disciplines. Eligibility criteria for enrollment in the DAOM program includes a Master's degree (or its equivalent) from an ACAOM-candidate or ACAOM-accredited school of acupuncture. A license to practice acupuncture is required before beginning this doctoral internship.
Harborview Medical Center
Harborview Medical Center (HMC) is a 413 bed tertiary-care hospital located in downtown Seattle, WA, USA, and is the only designated Level 1 adult and pediatric trauma and burn center in the state of Washington, serving as the regional trauma and burn referral center for Alaska, Montana, and Idaho. As a patient safety-net hospital, Harborview's mission is to provide a significant level of care to low-income, uninsured, and vulnerable populations, including those with mental health and substance use disorders. Harborview is owned by King County and managed by the University of Washington. The HMC Acute Pain Service (APS) is consulted for management of severe postsurgical pain, and peripheral nerve and epidural catheters; and for multimodal treatment plans for patients with challenging conditions (e.g., substance-use disorders, complex chronic pain, and opioid tolerance).
In 2015, the HMC Integrated Pain Care Program chief reached out to Bastyr leaders to form a collaborative agreement that would enhance student-learning experiences and the anesthesiology-based APS comprehensive-care service delivery. A hospital administrative policy was written to outline program administration and oversight by the APS director, acupuncture treatment indications and contraindications, and permissions and provisions for infection control. This policy only addresses use of acupuncture within the context of pain management for patients being cared for by the APS at HMC under the approval of the attending APS physician. The provision of acupuncture in the hospital as part of a comprehensive pain-treatment plan under the management of a responsible physician is a key feature of the model for replication. Per hospital policy, acupuncturists cannot independently practice medicine, diagnose a patient's condition, or prescribe for a patient.
Pre-COVID 19 Workflow
On designated clinical days at HMC, acupuncture students and their Bastyr faculty supervisor attend the daily morning hour-long sit-down rounds to review the list of APS patients. This “table rounds” is attended by the entire APS staff, including a nurse–practitioner, physician assistant, chemical-dependency counselor, rehabilitation psychologist, chaplain, pharmacist, and department of anesthesiology and pain medicine residents and attending physicians to facilitate care planning and communications among the entire team.
All patients are considered to be acupuncture candidates, unless any of them have contraindications to this treatment. Contraindications include therapeutic anticoagulation, absolute neutrophil count under 500, implanted defibrillator or vagal-nerve stimulators, untreated bacteremia, pregnancy, and acute decompensating conditions (medical or surgical emergencies with instability of vital signs). No acupuncture is performed on patients younger than age 3 without prior approval of the APS chief of service. Following this meeting, students consult with their Bastyr supervisors and review individual medical records to achieve a more-thorough understanding of each patient's history and current medical problems. Students then approach individual patients in their hospital rooms to offer acupuncture that day and obtain formal written consents for treatment after explaining risks (soreness, minor bleeding or bruising, rare infection) and benefits of the treatment. Students also coordinate with nurses and other care providers to ensure the best timing for patients and a smooth overall workflow for hospital staff.
A procedural “time-out” is performed immediately prior to the treatment session. A time-out is a universally practiced pause prior to any invasive procedure or surgery and is required by the Joint Commission and hospital policy prior for patient safety. This process includes having at least 2 staff members confirm correct patient, procedure, site, and other pertinent information (e.g., anticoagulation status, safe patient position, accurate consent, etc.).
A standardized documentation template for use in the Cerner Hospital and Health Systems 20 electronic medical record (Box 1) was developed to document the procedural time-out, a brief history, a tongue and pulse examination, TCM differential, pretreatment pain assessment, details of treatment provided including points used and needle count, post-treatment assessment of pain, complications, and future plans. Examination of the tongue (body, shape, color, coat, and texture) and assessment of a variety of pulse qualities are used by trained acupuncturists to indicate different Disharmonies and overall health, and strength of energy and vibrancy against illness. This information is used to help the acupuncturist determine the TCM differential diagnoses. including potential pathogenesis of present diseases or syndromes to design an appropriate point treatment plan. The pain-assessment field in the documentation template includes 2 well-validated self-reported pain scales; 0–10 on which 0 = “no pain” and 10 = “worst pain possible” and pain relief with categorical responses of “none,” “slight,” “moderate,” “lots,” and “complete.” 21
Electronic Health Record Documentation Template Variables for Acupuncture Procedure Note
OTHER means free text may be entered.
A faculty supervisor employed by Bastyr is on site to assist with student learning, patient care, and communication with staff and providers. The designated Bastyr faculty rounds bedside after the doctoral students, checking in with patients regarding their treatments, and frequently with the nursing staff. This provides feedback for students and another point of contact for patients as well as their caregivers. Additionally, faculty supervisors facilitate the doctoral students by providing ongoing education about the science and practice of acupuncture to the APS residents and other rotating staff. Throughout the day, supervisors and students discuss individual cases, often with other members of the APS care team. After students complete the electronic medical record treatment documentation, supervisors check and guide revisions or approve the records.
Program Outcomes
The University of Washington Institutional Review Board provided exemption status for a retrospective medical-record review of the acupuncture treatments. An electronic report was generated to analyze patients' characteristics and documented categorical items from the standardized treatment notes.
The average daily census for the APS at HMC is 20 patients. Of those a few are ineligible for acupuncture treatment due to contraindications or inability to be give their consent (e.g., being intubated and sedated, or having significant cognitive impairment) or are unavailable due to other scheduled inpatient care. The total numbers of eligible patients were not counted nor were those who declined treatment offers, but ∼80% of the patients in the daily APS census are offered acupuncture treatment, provided there are enough students in the clinical rotation to cover the demand.
RESULTS
Patient Self-Reported Outcomes
The sample for this report comprised 323 consecutive patients with acupuncture treatment notes recorded between July 24, 2017, and October 1, 2018. Of these patients, the average age was 43.6 (standard deviation [SD]: 15.2) and 61% were female. The most-common surgery type was orthopedic (36%). Patient-reported pain intensity ranged from 0 to 10, with an average pretreatment intensity of 6.40 (SD: 2.23) and post-treatment intensity of 3.72 (SD: 2.45). The average difference between pre and post pain intensity ratings was 2.68 (SD: 2.25; P < 0.001). Using a self-reported Pain Relief Scale, patients were documented as having none (7.4%), slight (22.6%), moderate (29.4%), lots of (14.9%), or complete (6.5%) relief from pain as a result of a single acupuncture treatment (Fig. 1). Nineteen percent of the pain relief data were missing because, early on, some students were misinformed about the need to query the patients for both change in pain intensity ratings and responses on the categorical Pain Relief Scale. Treatments averaged 36 minutes (SD: 17.99) and ranged from 20 to 79 minutes in length, with the exception of 1 treatment documented as lasting 215 minutes. The medical record for this outlier was manually reviewed by 2 of the current authors (S.B. and D.B.G.), who attributed the unusually long length of the treatment to allowing the patient to sleep during the treatment, and possibly including time for obtaining consent and for the time-out procedural processes.
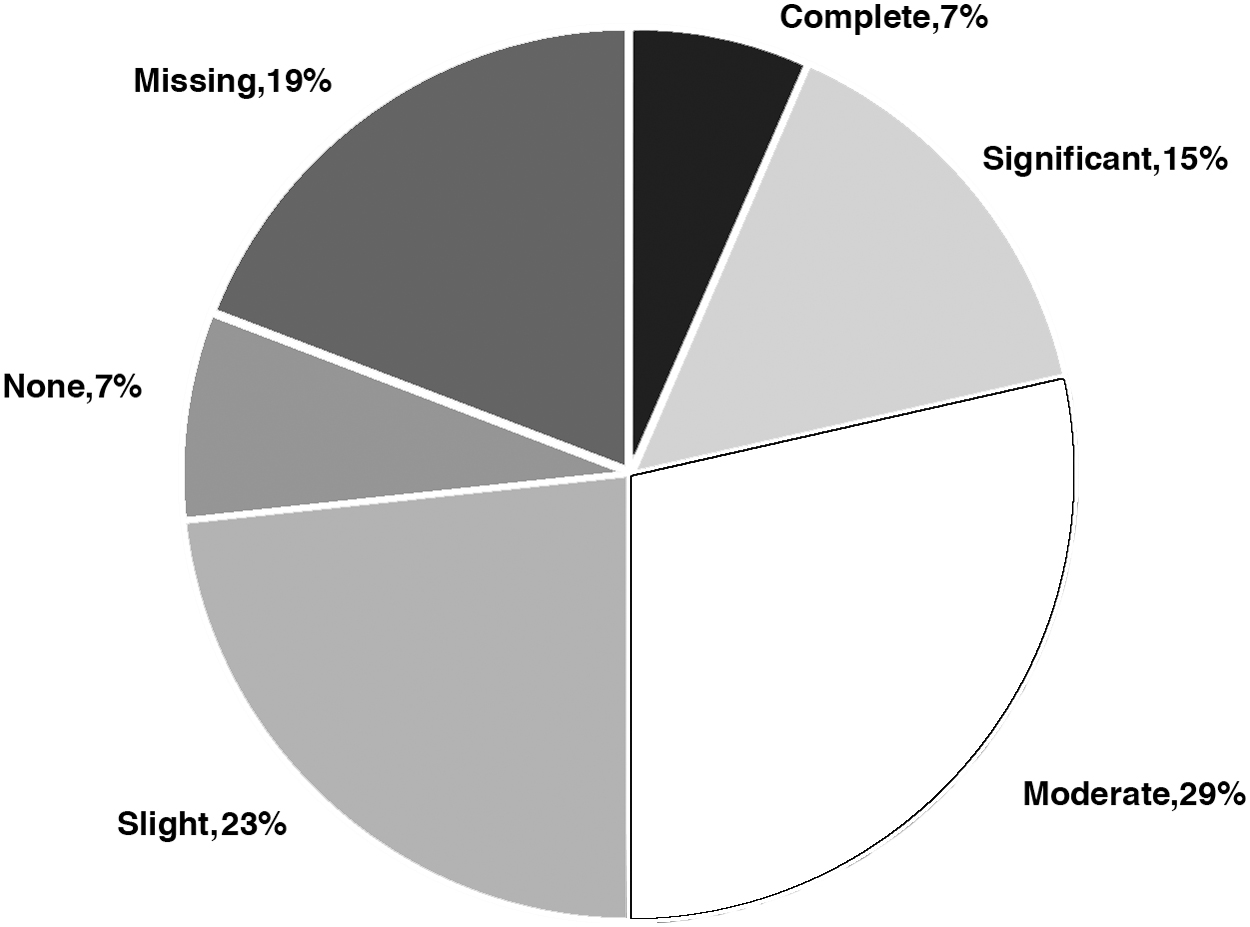
Self-reported Pain Relief Scale from a single acupuncture treatment.
The acupuncture treatments themselves were heterogeneous, varying, depending on each student's style of practice. All were licensed acupuncturists, and treatment types ranged from Toyohari to scalp electroacupuncture (EA). Data regarding style of practice and depth of needling were not recorded. Acupuncture needles included Mac Ultra Smooth Pipe (15 mm, 36 gauge; 30 mm, 34 and 36 gauge; and 40 mm, 32 gauge) as well as Serin J Type (30 mm 40 and 36 gauge). The EA device used was a Pantheon Research Electrostimulator 6c. Pro.
One patient asked for the needles to be removed early, reporting that she was experiencing a panic attack. Five patients had the needles removed early for safety when they were unable to lie still for the duration of the treatment and another 5 patients requested early removal of needles due to the need to urinate. Three treatments were disrupted by other staff members interrupting the procedures, and seven notes reported minor bleeding as a complication.
Students' and Staff Evaluations
The effectiveness of the educational model for DAOM students is also shown in student evaluations, as well as adoption of the program's acupressure and Qigong education materials by APS team members, and inclusion in the hospital system's online-on-demand patient education catalogue. In their evaluations of clinical rotations at HMC, students described their experiences as meeting or exceeding their expectations and used words that encapsulated the purpose and effectiveness of this model:
“I thought the experience at Harborview was one of the best parts of the program. Observing how patients were treated on the service and the relationship dynamics of the various doctors was very informative. It opened up new ideas for where acupuncture doctors can fit into an integrative or hospital-care model and also for when we don't. Other benefits include learning more about the drugs the patients are prescribed, learning where in the recovery process acupuncture is the most useful, and how acupuncture techniques can improve patient outcomes.” “My HMC internship literally changed my level of compassion, my understanding of medicine, and the power of complementary medicine. The experience altered the way I approach my patients and changed my understanding of substance use and how to approach patients on drug-regimens. It changed how I see and approach [patients] who self-medicate and why they don't seek medical assistance readily.” “My experience at Harborview Medical Center was an extremely important part of my DAOM program at Bastyr University. On many occasions, I treated patients that were in severe pain and taking strong medication. These patients were not able to relax or find any relief from their pain. Then, shortly after the acupuncture needles were applied, [these patients] fell into a deep sleep. This experience was extremely rewarding and clearly displayed that acupuncture is effective in hospitals for reducing pain. Practicing at Harborview Medical Center was also extremely challenging in many ways. As a practicing acupuncturist I see patients in my clinic during my scheduled hours. My patients are acupuncture-aware and expect a high-quality treatment. When practicing at Harborview Medical Center, I got to interact with patients from all over the world with varying medical conditions. Most of these patients have never had acupuncture before, and I had to clearly explain the procedure and the expectations of the treatment. This is quite difficult to accomplish through an interpreter, but also quite rewarding when the patient decides to give it a try. Acupuncture is becoming accepted as a powerful modality to reduce pain with difficult to treat patients.”
Constructive criticism was nearly absent in student evaluations. A comment that came close was in response to the question “What 3 things could the instructor improve upon that would have increased your ability to learn the material? Please be as specific as possible.” One student wrote: “Continue to encourage talking[,] discussing[,] and having different opinions.” Clinical supervisors have been asked in future to set aside time for evaluations on shift in order to glean more student recommendations for improvement.
Pain-service staff and other members of the patients' health care teams have also been positive about the program.
Post COVID-19
Restrictions of in-person student clinical experiences by the University of Washington and Bastyr during the COVID-19 pandemic of 2020 created a need to pivot to virtual learning experiences and novel treatment strategies. This resulted in the development of evidence-based, patient-self-care educational materials by the students. Materials included a series of brief instructional videos demonstrating how to use acupressure and Qigong to address pain, anxiety, stress, and sleep difficulties that are available on a public Bastyr YouTube channel. * Patient handouts on acupressure and Qigong developed by Bastyr faculty members were then edited further by UW staff members and adopted into the UW/HMC patient-education system; these handouts will continue to be used as a resource.
With the introduction of the online clinical-learning environment, clinical-student needs shifted. Anonymous evaluations yielded the following narrative feedback:
“I just appreciated the patience with the starting of this new virtual world. I was in a state of shock and nothing seemed to be working right. I don't see things well via the computer; how to do things, using it as a tool in this program has been essential, and even though we've had to automate quicker for the entire program, learning how to use today's technology is part of the doctorate program for me.” “The online clinic/rotations have been the best. … I love the group discussions…very valuable as a practitioner.” “Amazing that you have been able to get virtual learning up and running in such a short time, and even more, that it actually makes the program better in ways!” “I appreciate that we have Zoom meetings on a fairly regular basis with our virtual clinics because it helps me feel like we are all still connected in some way. I think the hardest part is sitting still at my computer for so many hours but, in all honesty, it is not so dissimilar to our in person DAOM weekends.” “Everything is going well, fewer surprises, good organization. Never used Zoom before-—getting easier. Help is going well. Emotional fatigue, and ability to keep up [are] taxed (like the capstone, which is a major project that takes planning and time) but, overall, things are good.” “One of my biggest issues is my internet kicking me out of the meeting at least a few times during the shift/class. The instructors don't always notice that someone is in the waiting room until that person texts another classmate and asks to be let in. I don't know if there is a more-reliable way of making sure instructors notice when someone is missing.” (This last piece of feedback was addressed by establishing a texting network between students and the instructor, which succeeded in ensuring everyone could be promptly readmitted to online meetings.)
Overall, the students' comments underscored the students' own adaptability and dedication, as well as that of the integrative clinical team.
DISCUSSION
National pain-management clinical practice guidelines 2 and the Joint Commission accreditation standards for hospitals support use of a multimodal approach to management of acute pain, including nonpharmacologic strategies such as acupuncture. As well, the U.S Food and Drug Administration and the National Academies of Sciences, Engineering, and Medicine recommend acupuncture as a first-line nonpharmacologic therapy to help cope with the ongoing national opioid crisis. 15 Integrating acupuncture services into busy acute-care environments where patients are seriously ill and have relatively short lengths of stay is a challenge. Students have to navigate finding uninterrupted bedside time with patients who may practically only be available to receive 1 treatment. Despite these challenges, the availability of acupuncture services allowed APS providers to offer a safe, low-risk intervention to contribute further to a multimodal analgesic regimen. In addition, the patients reported notable impacts from single acupuncture treatments.
A change of 1–2 points on a 0–10 pain intensity rating scale or a response of “moderate” relief on the Pain Relief Scale was reported by patients to be clinically meaningful improvement from a single opioid dose in a multicenter randomized, blinded, placebo-controlled trial. 22 The patients in this sample, reported achieving similar levels of pain relief following a single acupuncture treatment. As well, clinical trials of acupuncture delivered postoperatively in the hospital have produced significant reductions in pain, nausea, and anxiety, and improvements in patients' ability to cope with surgery. 23
This report was not designed with an a priori hypothesis and rather describes a model for program collaboration, preliminary findings, and adaptations to remote care and learning. Limitations of this evaluation included a single-site experience; lack of availability of other clinically relevant factors that affect perception and reporting of pain, including affect, mood, and patient expectations; timing of pain medications; and reliance on medical-record documentation. A strength was the use of valid and reliable patient-reported outcome measures. An additional strength was the introduction of novel adaptations to remote training and patient care.
While there is a paucity of evidence in the literature regarding acupuncture-student integration into hospital teams, many TCM training programs rely on relationships with facilities in China, where visiting Masters and doctoral students from the United States may observe inpatient hospital treatments. Additionally, a large number of schools maintain collaborative outpatient clinics in U.S. hospitals and other integrative settings. Both international externships and outpatient clinical training are conducted according to standards set by the ACAOM. 24 To the current authors' knowledge, the collaboration of the Bastyr DAOM program and HMC's inpatient APS is the first—and currently only—acupuncture-doctoral-student training of its kind, although it still falls under ACAOM's accreditation guidelines. Future studies could be designed to compare learner outcomes of various collaborative program models.
CONCLUSIONS
This model of collaboration between academic and clinical programs provides one example of a structure to integrate acupuncture into other hospital inpatient settings. DAOM acupuncture students and faculty were able to integrate successfully into an interdisciplinary inpatient APS, caring for a diverse and medically complex trauma-patient population. A majority of patients self-reported meaningful benefit from a single acupuncture treatment. Treatments were safe and well-tolerated by consenting patients. Incorporating acupuncture students' clinical rotations into an inpatient APS seems to be a beneficial collaboration for both patients and organizations, even when done remotely. Further research is warranted to evaluate the effect of a series of treatments, or to develop a more-rigorous study design to assess the impact on opioid sparing as part of a multimodal analgesic approach and more long-term, objective outcomes.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
This work was done by staff and students from Bastyr University and UW/HMC, and was not grant-funded.