
Abstract
Objective:
Obesity is an epidemic with an increasing prevalence in developing countries. The condition affects almost all physiologic functions of the body and is a significant threat to public health. Treatment of obesity is often difficult and expensive. Pharmacologic therapy has many side-effects. Acupuncture, a nonpharmacologic therapy, has shown promising results for treating obesity. Electroacupuncture (EA) and thread-embedded acupuncture (TEA) can be used. The aim of this study was to analyze the therapeutic effects of EA and TEA, using polydioxanone (PDO), on weight loss, waist circumference, and plasma-leptin concentrations in obese patients undergoing a dietary intervention.
Materials and Methods:
This single-blinded, randomized clinical trial randomized 34 subjects into 2 groups: EA and TEA. In the EA group, EA was administered 3 times per week for 4 weeks (a total of 12 sessions). In the TEA group, EA was administered only once. Body weight and waist circumference were measured at baseline, and on days 3, 7, 14, 21, and 28 (end) of the trial. Plasma-leptin concentrations were measured at the beginning and end of the trial.
Results:
There was a significant decrease in body weight and waist circumference in the groups before and after treatment (P < 0.001), and a significant decrease in plasma-leptin concentrations in the EA (P = 0.012) and TEA groups (P = 0.001). There were no significant differences between the groups in weight loss (P = 0.621), waist circumference (P = 0.545), and plasma-leptin concentration (P = 0.784).
Conclusions:
EA and PDO TEA are equally effective for reducing body weight, waist circumference, and plasma-leptin concentrations in obese patients undergoing dietary interventions. However, TEA is more time-efficient than EA.
INTRODUCTION
Obesity is defined as a chronic excess of body fat, and is typically diagnosed based on body mass index (BMI). Obesity is associated with an increased risk of various diseases, 1 the prevalence of obesity is rising in developing countries, and it is predicted to affect nearly half of the global population by 2030. 2 Obesity affects almost all physiologic functions of the body, poses a significant threat to public health, and is responsible for ∼5% of all deaths worldwide.2,3
BMI is the most-common measurement used to diagnose obesity. BMI is calculated as mass in kg divided by height in square meters, yielding the unit of kg/m2. 2 According to the Asia Pacific criteria, a BMI of <18.5 indicates underweight, 18.5–22.9 indicates normal weight, 23.0–24.9 indicates overweight, 25.0–29.9 indicates grade 1 obesity, and ≥30 indicates grade 2 obesity. 4 However, BMI has the disadvantage of not distinguishing between fat mass and lean body mass. Therefore, an additional measurement, such as waist circumference, must be included.5,6 White adipose tissue releases the hormone leptin, which plays a role in body weight regulation by maintaining the balance between food intake and energy consumption. The level of circulating leptin is proportional to body fat. 7 Obese people have leptin resistance, characterized by high leptin concentrations that lead to additional caloric intake and prevent weight loss. 8
Management of obesity involves lifestyle modification, pharmacotherapy, and surgery. However, these approaches are often difficult to comply with, unsuccessful, and expensive. 6 Therefore, there is an increasing social need to seek effective, affordable, and safe therapies for obesity. In this context, acupuncture may be an alternative.
Acupuncture has beneficial effects on obesity-related peptides, such as those involved with leptin, glucose and lipid metabolism and appetite reduction. Acupuncture modalities may vary, including electroacupuncture (EA) and thread-embedded acupuncture (TEA). 9 For EA, electrical stimulation is applied through insertion of acupuncture needles (attached to source electrostimulators) at specific acupuncture points. 10 For TEA, continuous, long-lasting, and intense stimulation is applied at specific acupuncture points.11,12
Because polydioxanone (PDO) is effective and has few-side-effects, it is used in TEA. PDO is a synthetic monofilament of polyester or a polymer of polydioxanone. 13 PDO thread embedding can be performed using a perpendicular or penetrating technique. In penetrating thread embedding, PDO is inserted at one point and then advanced internally until it reaches the second point. For this technique, less thread is used, but the effect is stronger because of stimulation from the extracellular matrix. 14 In addition, the high tensile strength of PDO enhances the mechanical tensile strength of tissues and supports the structure of the dermis and extracellular matrix, strengthening the components of collagen and elastin further. 15 To date, however, no study has compared the effectiveness of EA and TEA using PDO. Therefore, the purpose of the present study was to analyze the therapeutic effects of EA and TEA using PDO on weight loss, waist circumference, and plasma-leptin concentration in obese patients undergoing a dietary intervention.
MATERIALS AND METHODS
Study Design and Participants
The present study was a single-blinded, randomized clinical trial conducted from July 21, 2021, till October 26, 2021, at the Medical Acupuncture and Nutrition Clinic in RSUPN Dr. Cipto Mangunkusumo Hospital, Central Jakarta, DKI Jakarta, Indonesia. The study included patients who met the following criteria: (1) all sexes between the age of 18 and 60 years; (2) BMI between 25 and 35 kg/m2; (3) waist circumference >90 cm in males and >80 cm in females; and (4) willing to participate in the trial until its completion. Patients who met the following criteria were excluded: (1) pregnant; (2) postpartum <6 months; (3) diabetes mellitus (blood glucose ≥200 mg/dL); (4) hypertension (blood pressure ≥140/90 mm Hg); (5) fever >38°C; (6) contraindication to EA or TEA; (7) consumption of weight-loss medication (orlistat, phentermine, diethylpropion, etc.) or supplement (slimming tea, herbal medicine, etc.) in the past 25 hours; (8) kidney or/and liver disorders; and (9) history of acupuncture for weight reduction in the past 6 months.
The study protocol was approved by the Ethics Committee of the Faculty of Medicine of Universitas Indonesia (KET-576/UN2.F1/ETIK/PPM.00.02/2021) and was registered at ClinicalTrials.gov (NCT05023148). All participants read and signed informed consent forms prior to the start of the trial.
Sample Size
Considering a statistical power of 80%, a significance level of 5%, and a standard deviation and a mean difference based on a previous study, 16 and a dropout rate of 10%, the present trial included 34 participants for randomization and treatment. The participants were allocated randomly to one of 2 groups based on computer-generated numbers: (1) an EA group (n = 17) and (2) a TEA group (n = 17). Both groups received the same dietary intervention.
Treatment Protocol
The points selected for the trial included CV-12, CV-9, CV-6, CV-4, ST-25 bilateral; SP-15 bilateral, and ST-40 bilateral. During all treatments, the participants were placed in a supine position, and pretreatment antisepsis and asepsis were applied at each acupoint.
In the EA group, 0.25 × 40–mm needles at bilateral CV-12 and CV-9, CV-6 and CV-4; right ST-25 and SP-15; left ST-25 and SP-15 were each connected to 1 source electrostimulator (Hwato SDZ V), and 0.25 × 25-mm needles at bilateral ST-40 were connected to another source electrostimulator. Then, the electrostimulators were activated to deliver a continuous-wave 2 at Hz for 30 minutes, with a low intensity that could be tolerated by the participants. The treatment was administered 3 times per week for 4 weeks (a total of 12 sessions). Both images of Figure 1 show a patient receiving EA. (Fig. 1).
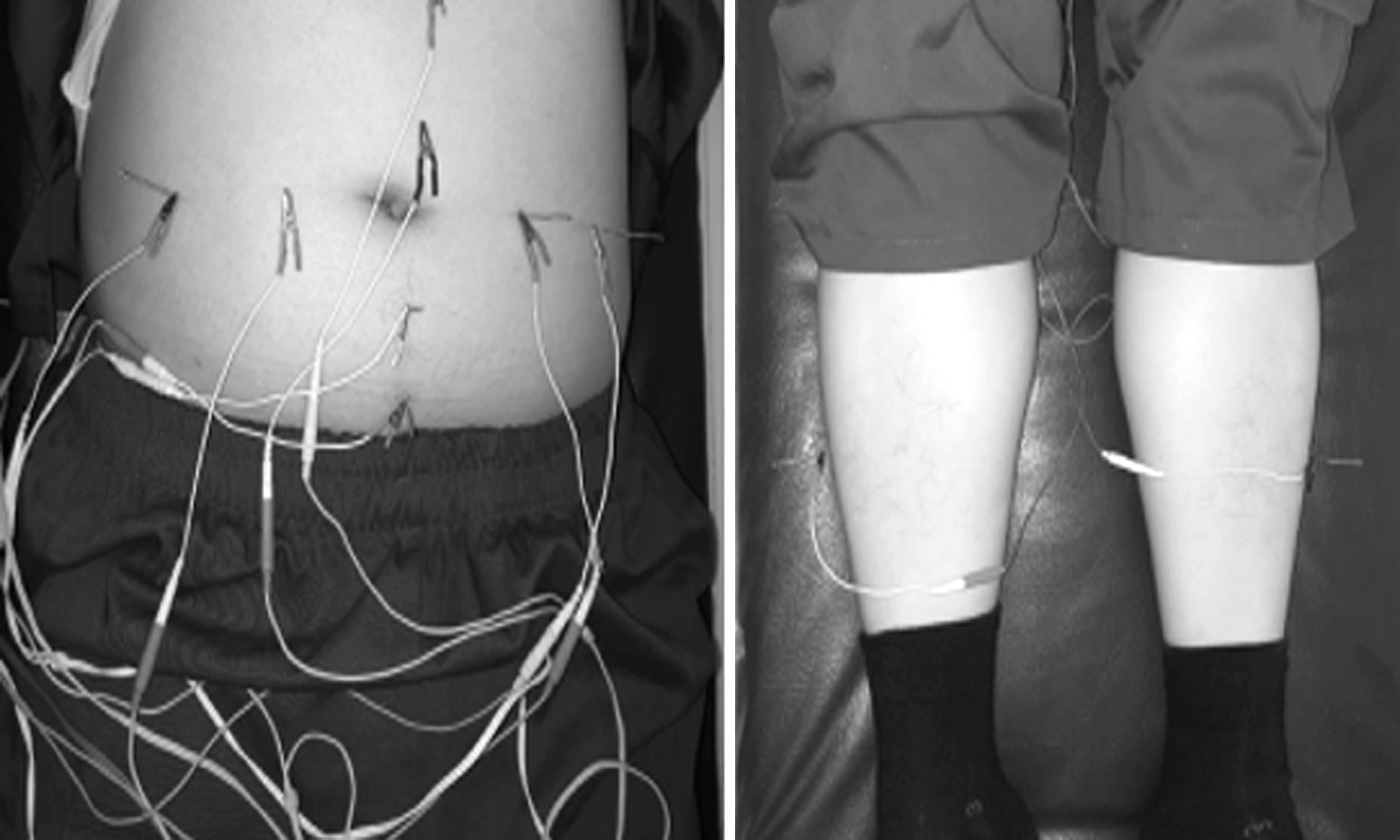
Electroacupuncture.
In the TEA group, a single-use needle (Fig. 2). PDO thread was inserted at a 30° angle. A PDO 5-0 27G × 60–mm syringe was used at CV-12 leading to CV-9, as well as a PDO 5-0 27G × 40-mm syringe at ST-25 leading to SP-15, and at CV-4 leading to CV6. A 31G × 25–mm syringe was inserted perpendicularly at ST-40 bilaterally. Following thread implantation (Fig. 3), the needle was removed and discarded in a safety box. The puncture site was closed with a bandage. This treatment was administered only once.

Polydioxanone thread-embedding acupuncture needles.

Polydioxanone thread-embedding acupuncture.
For the dietary intervention, the resting and total energy expenditures of all participants were calculated and gradually reduced by 500 kcal/day from the total daily energy requirement by taking into account participants' eating habits when consuming low-calorie diets (low-fat and low-carbohydrate). This diet was monitored and reevaluated after 14 days.
Figure 4 shows a flow chart for the study.

Study flow chart. EA, electroacupuncture; TEA, thread-embedding acupuncture; PDO, polydioxanone.
Outcomes
Body weight and waist circumference were the primary outcome measurements. Plasma-leptin concentration level was the secondary outcome. Body weight and waist circumference were measured at baseline and on days 3, 7, 14, 21, and 28 (end) of the trial. Plasma-leptin concentration was measured at the beginning and end of the trial using a DRG® Leptin Sandwich enzyme-linked immunosorbent assay kit. 17
Statistical Analysis
Data were analyzed using SPSS, version 20. For the primary outcome, a repeated-measures analysis of variance was used for within-group and between group analyses if the data were normally distributed or a Friedman analysis was used if the data were non-normally distributed. For the secondary outcome, if the data were normally distributed, an independent t-test was used for between-group analysis and a paired t-test was used for within-group analysis. However, if the data were non-normally distributed, a Mann–Whitney-U test was used for between-group analysis and a Wilcoxon signed-rank test was used for within-group analysis. A P < 0.05 indicated significance.
RESULTS
Participants
The 45 participants who applied for the study were screened; 34 met the inclusion criteria and were enrolled for the trial after they provided signed informed consents. These participants were randomly allocated into the 2 groups: EA (EA + dietary intervention) and TEA (TEA + dietary intervention). Each group included 17 participants; there were no dropouts (Fig 4).
Baseline Measurements
There were no significant differences between the 2 groups in terms of age, sex, body shape, BMI, waist-to-hip ratio, blood pressure, heart rate, and blood-glucose concentrations. The majority of the participants were females with an apple-shaped body type (Table 1).
Baseline Characteristics
= Mann–Whitney-U test; f = Fisher's exact test; t = independent t-test.
EA, electroacupuncture; TEA, thread-embedded acupuncture; yrs, years; BMI, body mass index; WHR, waist–hip ratio; BP, blood pressure; HR, heart rate; bpm, beats per minute.
Body Weight
Significant weight loss was noted in the EA group on the fourteenth day of evaluation. In the TEA group, significant weight loss was noted on the twenty-first day of evaluation. Before treatment, the mean baseline body weight was 76.03 ± 10.52 kg in the EA group and 74.24 ± 6.00 kg in the TEA group. Mean body weight decreased by 1.88 ± 1.43 kg (P = 0.001) in the EA group (74.15 ± 9.74 kg) and by 1.47 ± 1.02 kg (P < 0.001) in the TEA group (72.76 ± 5.96 kg; Fig. 5 and Table 2). In a time–pairwise comparison analysis, there was a significant mean difference in body weight from the fourteenth day of evaluation (P = 0.030; Table 3). However, there were no significant mean differences in body weight according to group analysis (P = 0.566; Table 3) and time–group interaction analysis (P = 0.621; Table 3).

Mean weight loss in the electroacupuncture and thread-embedding acupuncture groups.
Comparison of Mean Weight Loss on Every Evaluation Day in the Electroacupuncture and Thread-Embedded Acupuncture Groups
= analysis of variance (repeated measures).
P < 0.05.
EA, electroacupuncture; TEA, thread-embedded acupuncture.
Comparison of Mean Difference Body Weight on Every Evaluation Day between the Electroacupuncture and Thread-Embedded Acupuncture Groups
= analysis of variance (repeated measures).
P < 0.05.
EA, electroacupuncture; TEA, thread-embedded acupuncture.
Waist Circumference
A significant decrease in waist circumference was noted in the EA group on the third evaluation day. In the TEA group, a significant decrease in waist circumference was noted on the seventh evaluation day. The mean baseline waist circumference was 93.79 ± 7.18 cm in the EA group and 92.17 ± 6.46 cm in the TEA group. Waist circumference decreased by 6.15 ± 2.69 cm (P < 0.001) in the EA group (87.65 ± 7.93 cm) and by 5.94 ± 2.89 (P < 0.001) in the TEA group (86.34 ± 5.25). See Figure 6 and Table 4. In a time pairwise-comparison analysis, there was a significant mean difference in waist circumference on the third evaluation day (P < 0.001; Table 5). However, there were no significant mean differences in waist circumference in a group analysis (P = 0.477; Table 5) and in a time–group interaction analysis (P = 0.545;Table 5).
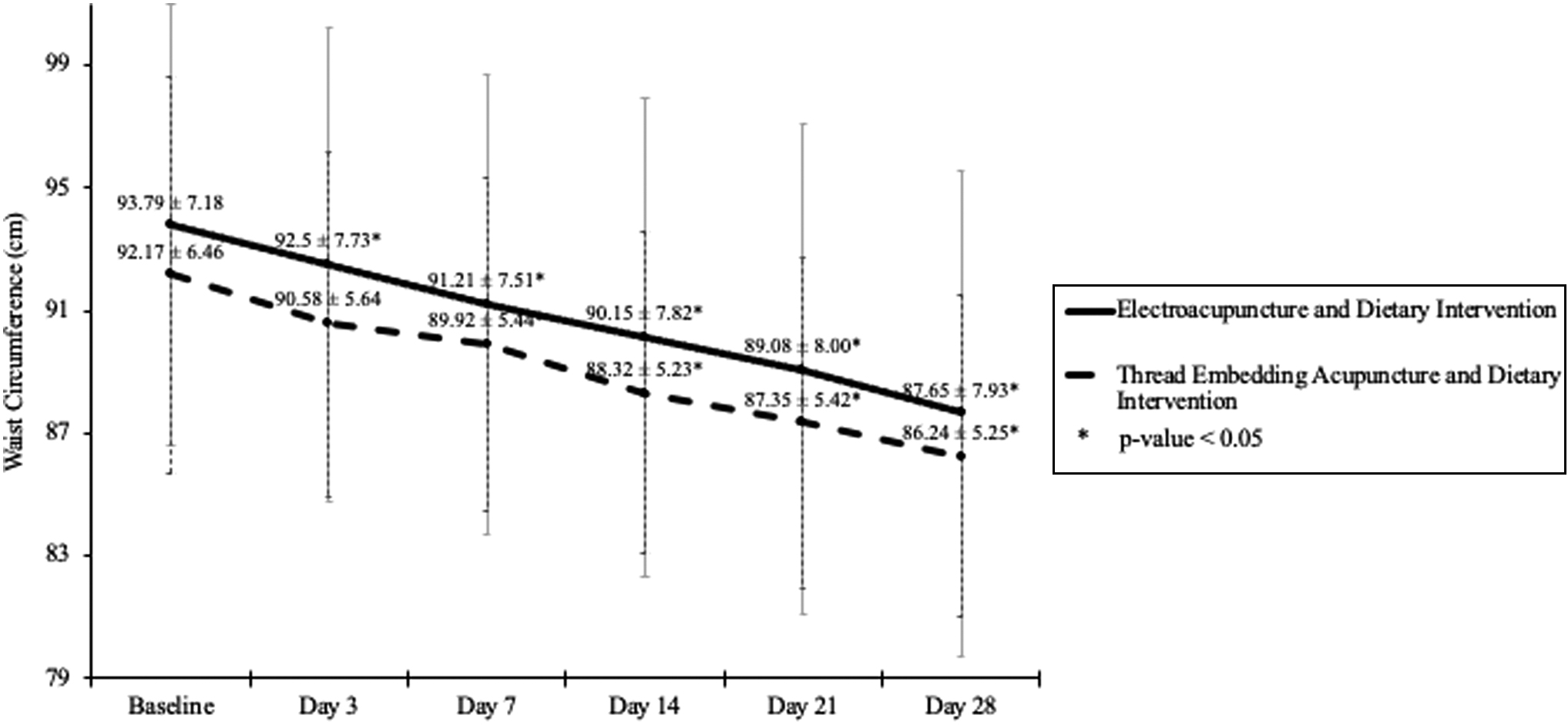
Decrease in mean waist circumference in the electroacupuncture and thread-embedding acupuncture groups.
Comparison of Decrease in Mean Waist Circumference on Every Evaluation Day in the Electroacupuncture and Thread-Embedded Acupuncture Groups
= analysis of variance (repeated measures).
P < 0.05.
EA, electroacupuncture; TEA, thread-embedded acupuncture.
Comparison of Mean Differences in Waist Circumference on every evaluation Day between the Electroacupuncture and Thread-Embedded Acupuncture Groups
= analysis of variance (repeated measures).
P < 0.05.
EA, electroacupuncture; TEA, thread-embedded acupuncture.
Plasma-Leptin Concentration
Plasma leptin concentration was significantly decreased in both groups. Mean baseline plasma leptin concentration was 17.05 ± 6.21 ng/mL in the EA group and 12.31 ± 5.96 ng/mL in the TEA group. Plasma leptin concentration decreased by 3.32 ± 4.86 ng/mL (P = 0.012) in the EA group (13.73 ± 6.08 ng/mL) and by 2.93 ± 3.15 ng/mL (P = 0.001) in the TEA group (9.38 ± 4.85 ng/mL). Thus, there was no significant difference in mean leptin concentration before and after treatment between the 2 groups (P = 0.784; Tables 6 and 7).
Comparison of Mean Plasma-Leptin Concentration Before and After Treatment in the Electroacupuncture and Thread-Embedded Acupuncture Groups
= paired t-test.
P < 0.05.
EA, electroacupuncture; TEA, thread-embedded acupuncture.
Comparison of Reduction in Plasma-Leptin Concentration between the Electroacupuncture and Thread-Embedded Acupuncture Groups
= independent t-test.
EA, electroacupuncture; TEA, thread-embedding acupuncture.
Side-Effects and Other Findings
In the EA group, local bruising was noted in 6 of the 204 procedures (2.9%). The bruises resolved without any intervention within 1 week. In the TEA group, 5 participants (29.41%) experienced slight discomfort at the site of thread embedment, although this discomfort did not last long (< 24 hours). No other side-effects, such as infections or allergy, were noted.
Other effects experienced by participants in both groups included normal bowel movement, satiation, and reduced appetite. One participant with a history of dysmenorrhea reported that her dysmenorrhea disappeared after TEA. Three other participants reported that their knee, heel, and ankle pain disappeared after treatment.
DISCUSSION
The present trial included more female than male participants. This trend is consistent with the global data survey and Riskesdas Indonesia 2018 information, according to which there were more obese females (29.3%) than males (14.5%) in the >18 year age group of.18,19
EA is most frequently used to control body weight because of its constant and measurable stimulation. In several studies, EA was reported to alleviate leptin resistance, decrease plasma-leptin concentration, and upregulate leptin-receptor expression in the hypothalamus.20–23
Furthermore, EA has been proven to be more effective than manual acupuncture for treating obesity. 24 The arcuate nucleus of the hypothalamus is more sensitive to low-frequency EA than to high-frequency EA. Peripheral leptin can penetrate the third ventricle and bind leptin receptors in the arcuate nucleus of the hypothalamus, thereby stimulating proopiomelanocortin/cocaine- and amphetamine–regulated transcript (POMC/CART) and suppressing neuropeptide Y/aguti-related protein (NPY/AgRP), ultimately producing anorectic effects. 25
Moreover, low-frequency EA promotes endorphin and serotonin release, of which endorphins produce a lipolytic effect. 26 EA at a 2-Hz frequency 3 times per week for 4 weeks suppressed NPY but augmented alpha-melanocyte-stimulating hormone (α-MSH), POMC, and CART, leading to reduced food intake, weight loss, and increased insulin sensitivity through the SIRT1 and peroxisome proliferator-activated receptor γ-coactivator (PGC-1α) pathways. 20 According to Mayor, 10 the optimal effect of EA is achieved within 30–45 minutes. Therefore, EA at a 2-Hz frequency 3 times per week for 4 weeks with retention for 30 minutes was expected to reduce body weight, waist circumference, and plasma-leptin concentration.
In TEA, continuous, long-lasting, and intense stimulation is applied at acupuncture points; thus, the number of visits to the service provider can be reduced. In a cost–benefit analysis, TEA was shown to be more cost-effective and economically advantageous while being as effective as EA for treating obesity.11,12 The PDO TEA protocol followed in the present trial used the penetrating method, which required less thread but still produced a stronger effect due to stimulation of the extracellular matrix. 14 In addition, the high tensile strength of PDO sutures increased the mechanical tensile strength of the tissue and supported the structure of the dermis and extracellular matrix, increasing collagen and elastin components further. 15
Additionally, penetration of subcutaneous tissue provided mechanical and chemical stimulation, which can promote connective tissue regeneration and enhance cellular activation, thereby activating intercellular interactions, neovascularization, and mechano-transduction. Such mechanical effects can induce signal transduction and gene expression of fibroblasts, adipocytes, and immune cells, which mediate acupuncture mechanisms.27,28
Acupuncture points used in the present study were CV-12, CV-9, CV-6, CV-4, ST-25, SP-15, and ST-40. CV-12 inhibits gastric motility through transient-receptor potential cation channel subfamily V (TRPV) stimulation and endorphin release and, together with ST-25, modulates serotonin secretion. 29 CV-9, CV-6, SP-15, and ST-40 can collectively reduce body weight, waist circumference, and leptin concentration. 20 CV-12, together with CV-4, ST-25, and ST-40, can reduce leptin concentration and promote nesfatin-1, ghrelin, and cholecystokinin (CCK) expression. 30 CV-4, together with ST-25, can reduce body weight, increase serotonin secretion, improve intestinal-transit rate, resolve intestinal microbiota dysbiosis, and promote intestinal motility. 31 CV-12 and CV-4 increase adiponectin and, together with ST-40, suppress tumor necrosis factor–alpha (TNF-α), nuclear factor kappa B (NFκB), and NPY and elevate interleukin-10.25,32,33 CV-9 has a diuretic effect. 34
Obesity treatment requires a state of negative energy balance, such that any dietary intervention can reduce calorie intake. 35 A low-calorie diet can reduce body weight by ∼0.5–1 kg per week by inhibiting proinflammatory pathways and reactive oxygen species generation by lowering serum advanced glycation end-products through the glycation/lipoxidation reduction process.36–38
In the present study, both EA and TEA, accompanied by the dietary intervention, effectively reduced body weight, waist circumference, and plasma-leptin concentration in obese patients. The mean weight loss of, respectively, 1.88 kg and 1.47 kg in the EA and TEA groups was consistent with the results of a previous study by Chen et al., 16 who noted a mean weight loss of 1.65 kg with catgut chromic TEA at CV-6, CV-9, ST-28, KI-14, and ST-36 once per week for 6 weeks in 90 obese females (versus a single session of TEA at different acupoints in both males and females).
The present study's results are also in line with the findings of a previous study by Chen et al., 39 who used polyglycolic acid (PGA) TEA on 51 subjects every 10 days for 10 weeks and noted a body weight loss of 4.15 kg. However, the frequency and duration of acupuncture in that study were greater than those in the present study. Furthermore, PGA sutures lead to a weaker inflammatory-tissue reaction and have a lower tensile strength (89% less after 1 week, 63% less after 2 weeks, and 17% less after 3 weeks) than PDO sutures (74% less after 2 weeks, 50% less after 4 weeks, and 25% less after 6 weeks). In addition, PGA is completely hydrolyzed by 90–120 days, whereas PDO requires ∼180 days. 13
García-Vivas et al., 40 compared the effectiveness of acupuncture with moxibustion, long-needle acupuncture with moxibustion, EA with a dense–disperse (D–D) wave of 4 Hz, EA with moxibustion, and catgut chromic TEA with moxibustion (CGM) and recorded body weight losses of, respectively, 4.1 and 2.6 kg in the EA and CGM groups. However, the acupoints and technique used in that study differed from those used in the present study. As an additional treatment, participants in the present trial were administered a dietary intervention; however, the compliance was not satisfactory (average recommended diet: 1297 calories; average measured intake: 1365 calories), which likely affected weight-loss results. According to Raynor et al., 41 3%–5% weight loss can improve clinical health and a greater weight loss can reduce risk factors for cardiovascular disease; therefore, 5%–10% weight loss in 6 months is recommended. In the present study, the average monthly weight loss was 2%–2.5%.
The decreases in waist circumference of, respectively, 6.15 cm and 5.94 cm in the EA and TEA groups was in line with the results of a study in 2018 by Kristiani, who noted a 4-cm decrease in waist circumference using EA with D–D waves of 5/25 Hz for 30 minutes 3 times per week at CV-12, CV-4, ST-25, ST-36, and ST-40, without connecting ST-44 and SP-6 to the electrostimulator. In the present trial, a relatively greater reduction was noted in waist circumference using EA with a continuous 2-Hz wave at fewer acupoints overall but using more acupoints on the abdominal area. Low-frequency EA mediated by the μ- and δ-receptors stimulates the release of endogenous opioids endorphins and enkephalins, with endorphins producing a 2.5-fold stronger lipolytic effect than enkephalins.10,42 The lipolytic effect of endorphins is associated with increased free fatty acid and glycerol lysis.43,44 In this light, more acupoints in the abdominal area in the current study protocol likely produced stronger lipolysis, reducing waist circumference to a greater degree.
Similarly, in a study by Garcia-Vivas, 40 waist circumference in EA and CGM groups was reduced by 4 and 3.6 cm, respectively. In a study by Tanudjaja et al., 45 catgut chromic TEA at CV-12, CV-6, ST-25, and SP-6 performed alternately 2 times at 2-week intervals reduced abdominal circumference by 7.5 ± 3.4 cm. The use of PDO sutures likely affected the results of waist circumference in the present study, as PDO produces lower tissue reactivity than catgut chromic sutures. 13 Lower tissue reactivity can lead to a weaker inflammatory reaction at acupoints, affecting the efficacy of acupuncture. Nonetheless, the use of PDO sutures is more advantageous because fewer needles are required; multiple acupoints can be stimulated through a single insertion with the penetrating method, the procedure is simpler, and the risk of infection is smaller.
One of the most well-known adipokines involved in weight loss is leptin, which acts on the arcuate nucleus of the hypothalamus to suppress food intake and stimulate energy expenditure through increased thermogenesis. Plasma concentration of leptin is linked to the severity of obesity; obese patients have elevated plasma-leptin concentrations—leptin resistance. 20 Normal plasma-leptin concentration in humans is ∼5 ng/mL. 46 In the present study, plasma-leptin concentration decreased by, respectively, 3.32 and 2.93 ng/mL in the EA and TEA groups. This decrease was in line with the results of a previous study in 2016 by Juanieta, who noted a decrease of 8.08 ng/mL in leptin concentration using EA with D–D waves of 2 Hz for 20 minutes at ST-25, ST-28, CV-12, CV-9, CV-4, and SP-6 applied 3 times per week for 4 weeks (versus EA with a continuous 2-Hz wave at SP-15, CV-6, and ST-40 in the present study).
Similarly, in a study by Cabioělu and Ergene, 26 EA with a continuous 2-Hz wave for 30 minutes was applied on alternate days at ear acupoints (Hunger and Shen Men) and every day at body acupoints LI-4, LI-11, ST-25, ST-36, and ST-44 for 20 days, accompanied by a 1400-calorie diet per day. The researchers noted an 8.8-ng/mL decrease in leptin concentration and an increase in endorphin levels, which played a role in weight loss. In contrast, in the present study, EA was applied at only body points and delivered 3 times per week for 4 weeks (a total of 12 sessions), along with a dietary intervention with a reduction of 500 calories from the daily intake. However, in both studies, leptin concentrations were reduced significantly.
The current study results were also consistent with the findings of Chen et al., 16 who noted a 5.2-ng/mL decrease in leptin concentration when using catgut chromic TEA once per week for 6 weeks in 90 obese females. Meanwhile, the present study included both males and females, and TEA was applied once using PDO.
In another experimental study, Yang et al., 47 proved that TEA could reduce leptin concentration and enhance leptin-receptor expression in the hypothalamus, thereby reducing leptin resistance, which is a characteristic of obesity. Leptin binds leptin receptors in the hypothalamus, which stimulates POMC and CART to increase the anorexigenic peptide α-MSH and suppress the orexigenic peptides NPY and AgRP, thereby decreasing appetite, augmenting uncoupling protein expression in adipose tissue, and increasing energy expenditure.20,47
Furthermore, in the present trial, most participants had normal bowel movements, satiation, and reduced appetite, consistent with the mechanism of action of acupuncture for treating obesity; specifically, release of neurotransmitters serotonin and endorphins affects leptin sensitivity, which stimulates anorexigenic POMC and CART to reduce appetite.26,48 Acupuncture can also affect the enteric nervous system, which reduces gastric motility and then improves intestinal-transit rate to enable satiation and normal defecation. 31 Some participants in the present study reported alleviation of pain in supporting parts of the body such as knees, heels, and ankles after treatment. This may be attributed to weight loss reducing the mechanical burden of obesity. One participant reported resolution of dysmenorrhea following PDO TEA. CV-4 and CV-6, used in the present study, are often used to deal with dysmenorrhea. In a systematic review and meta-analysis, acupuncture was reported to be effective for reducing pain in females with primary dysmenorrhea. 49
In clinical settings, based on the frequency and cost of treatment, PDO TEA is more economical and time-efficient than EA. With comparable effectiveness, PDO TEA requires only a single session, as opposed to 12 EA sessions to achieve the same effect. In a systematic review and meta-analysis, Cho et al., 12 concluded that TEA had a lower cost and was economically more beneficial, with comparable effectiveness to EA, for treating obesity.
The present study had limitations, such as no control group with only a dietary intervention. However, according to prior studies, both TEA and EA alone, or in combination with a dietary intervention, had a better effect on obesity parameters than dietary intervention alone.39,45,50–52 Other limitations in this study were a lack of inclusion of physical-activity interventions and relatively short time and follow-up durations. Thus, further studies are warranted with a longer follow-up duration and inclusion of physical activity, in addition to a dietary intervention.
CONCLUSIONS
EA and PDO TEA are equally effective for reducing body weight, waist circumference, and plasma-leptin concentration in obese patients undergoing a dietary intervention. However, TEA is more time-efficient than EA.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
The authors received no financial support for this research.