
Abstract
Objective:
The goal of this research was to study the feasibility of comparing heat therapy with sea salt versus sea salt combined with Chinese herbs for chronic low-back pain (cLBP) due to lumbar-disc herniation (LDH).
Materials and Methods:
This was a randomized, single-blinded, controlled feasibility study. Eight participants with cLBP were randomly allocated into 2 groups. Group S received a warm sea-salt bag alone and group S + H received warm sea-salt combined with Chinese herbs. Both groups (S and S+H) received treatment on the tender spot of the low-back area for 30 minutes, 3 times per week for 8 treatments. Participants were evaluated with the Roland–Morris Questionnaire (RMQ) for disability and a numeric rating scale (NRS) for pain before and after treatment.
Results:
The RMQ and the NRS revealed significant improvement in group S + H for reducing disability symptoms and LDH-related pain after treatment. Group S also had significant reductions per the RMQ scores after treatment but this result was not seen on the NRS. No signs of any side-effects were observed for either group.
Conclusions:
Heat therapy using a warm sea-salt bag + Chinese herbs helped reduce disability symptoms and cLBP due to LDH. It is feasible to conduct larger clinical studies to verify the results.
INTRODUCTION
Low-back pain is the leading cause of missed workdays in the United States. 1 It costs Americans more than $100 billion per year and U.S. companies ∼$25 billion annually.2,3 Lumbar-disc herniation (LDH) can cause acute low-back pain (LBP) and chronic low-back pain (cLBP). Approximately 5%–15% of patients with LBP suffer from LDH. 4 LDH has become a major cause of disability affecting 1%–3% of the general population in the world.5,6
Current conservative therapies for cLBP due to LDH include nonsteroidal anti-inflammatory drugs, acetaminophen, muscle relaxants, or even a short course of opioid pain medication in conjunction with physical therapy. If conservative methods do not provide symptomatic relief, invasive treatments, such as epidural steroid injections or even surgery, are considered. 7 The question is if there are alternative options for patients for whom conservative therapies and/or invasive procedures fail, before considering surgical options such as discectomy, disc arthroplasty, or spinal fusion.
Superficial heat therapy has been used for centuries to relieve pain and promote health. 8 The latest clinical guidelines from the American College of Physicians recommends superficial heat therapy as a nonpharmacologic treatment for reducing LBP. 9 Superficial heat elevates temperature of the area it is applied to and improves circulation of the surrounding tissues. Heat therapy includes such modalities as hot-water bottles, heated stones, soft heated packs filled with grain, hot towels, hot baths, saunas, steam, heat wraps, heat pads, electric heat pads, and infrared heat lamps. 10 The physiologic effects of these modalities include pain relief and increases in blood flow, metabolism, and elasticity of connective tissues. 11 Sea salt is also a good material for preserving heat and is often used in heat therapy.
According to acupuncture theory, chronic LDH is known as Bi Syndrome, usually caused by Blood Stasis, pathogenic Cold and Dampness, or Kidney Deficiency. External and internal use of Chinese herbs—such as Duo Huo (Angelica pubescentis radix), Dang Gui (Angelica sinensis radix), San Qi (Notoginseng radix), Du Zhong (Eucommia cortex), and Sheng Jiang (Zingiber recens rhizoma)—showed high efficacy for treatment of LBP. 12 Zheng Gu Shui liniment is another popular patented herbal extract used among martial-arts practitioners and athletes to address their pain and tissue damage. 13 Hong Cong Tou (Eleutherine bulb or shallot) has also been used as an anti-inflammatory. 14 Modern pharmacologic studies have shown that these Chinese herbs may reduce LBP via their known analgesic, anti-inflammatory, and antispasmodic effects.15,16
The purpose of this study is to examine the feasibility of comparing heat therapy with warm sea salt alone versus sea salt combined with Chinese herbs for treating cLBP due to LDH. Indeed it would be interesting to learn if the heat therapy and topical Chinese herb combination synergistically reduced LBP and reduced LDH-associated disability symptoms.
MATERIALS AND METHODS
The study design and treatment protocol were reviewed and approved by the Atlantic Institute of Oriental Medicine (Fort Lauderdale, FL) institutional review board. The study was conducted by 1 licensed acupuncturist Cheung in a single private acupuncture clinic and Hong participated in the study design. Participants were recruited through digital and print advertisements. All prospective participants were interviewed in the clinic. Details about the study were discussed and all risk factors were disclosed. All participants were asked to sign the Protection of Human Subjects Consent Form. This study was a randomized, single-blinded, controlled feasibility study. Eight participants were enrolled, using the criteria shown in Table 1, which also shows the criteria that would have been used for dropouts.
Inclusion, Exclusion, and Dropout Criteria
yrs, years, LDH, lumbar-disc herniation; mos, months.
Randomization
The participants were divided randomly into two groups, a sea-salt alone group (Group S) and an herbal sea-salt group (Group S+H). To achieve randomization, each participants was asked to draw 1 paper from a box containing papers folded 4 ways and marked with a letter X (denoting Group S) or Y (denoting Group S+H) inside the paper. Each participant was then asked to hand the chosen folded paper back to the researcher, who unfolded the it to record the name of the group that the patient was allocated to.
Blinding
The participants were not informed which groups they were in. To keep this single blinding, a fresh herbal sea-salt bag was always brought into the treatment room during all treatment sessions to create a fragrant environment for the patients both groups. At the end of the study, all participants were surveyed to learn if they had known which groups they were in.
Preparation of Both Sea-Salt Bags
The plan sea-salt bag contained 1 kg of sea salt only in a cotton bag.
The herbal sea-salt bag ingredients were: 1 kg of sea salt; 100 g of Hong Cong Tou (fresh shallot bulb); 50 g of Sheng Jiang (fresh ginger); 5 g of granulated Duo Huo; 5g of granulated Dang Gui; 5 g of granulated San Qi; and 5 g of granulated Du Zhong. Preparation of the herbal sea-salt bag was as follows:
Hong Cong Tou was cut into 8 pieces and Sheng Jiang was cut into pieces 0.5-cm thick. The pieces were stir-fried dry with the sea salt and granulated herbs in a pan on a stove at a medium temperature. The stirring was performed for 15–20 minutes until the mixture became fragrant; the sea salt had turned slightly brown; and the Hong Cong Tou and Sheng Jiang had cooked and become brownish. Then, the stove was turned off and more granulated herbal ingredients were added and mixed. After cooling, the herbal sea salt was put into a cotton bag and sealed. The cooking took ∼25–30 minutes and the cooling took another 30 minutes. Based on experience, a freshly made herbal sea-salt bag can be reused up to ∼50 times before the herbal fragrance dissipates.
The different materials and treatments used in Group S and in Group S + H are summarized in Table 2.
Materials and Treatments for Group S and Group S + H
Treatment Procedure
The treatment procedure was as follows:
The plain or herbal sea-salt bag was heated in a microwave for 2 minutes. The bag temperature, ∼60°C–62 C°, was checked by a digital thermometer. The warm bag then was placed in a wool bag and then covered by a cotton towel. Each participant laid on a treatment table in a prone position. The researcher palpated the participant's low-back area and identified the tender spot, in order to place the warm bag in the correct area. Zheng Gu Shui liniment was applied to the tender area for Group S + H participants and then a clean towel covered the area, while alcohol rubbing was applied to Group S participants to imitate the Zheng Gu Shui liniment. The warm bag was then placed on the participant's treatment area for 30 minutes. The surface temperature of the treatment area was kept ∼45°C–48 C°. The surface temperature was monitored frequently to prevent skin burn. After 15 minutes, a second fresh warm bag was used to replace the first one to maintain the optimal temperature of 60°C–62 C°. After 30 minutes of treatment, the warm bag was removed, and the treatment area was cleaned to remove any trace of the herbal fragrance. The treatment was conducted 3 times per week for a total of 8 sessions within 3 weeks.
Outcome Measurements
First published in 1983, the Roland–Morris Questionnaire (RMQ) for disability is designed to assess self-rated physical disability caused by LBP. 17 The 24-question version of the RMQ was used in the study. Any “yes” to the question was counted as 1point and the total score can range from 0 to 24. A higher score indicates a worse disability condition. The intensity of LBP was measured with a numeric rating scale (NRS) for pain. 18 Participants were asked to circle a number from 0 to 5, with 0 meaning “no pain,” and 5 meaning “the worst possible pain.” All participants were surveyed with the RMQ and NRS before the first treatment and after the 8th session. Data were recorded and analyzed using Microsoft Excel. P- value was calculated with a t-test that had a “paired two-sample for means” function.
RESULTS
This study was conducted between April and November of 2021. Due to the COVID-19 pandemic, only 8 participants were recruited. All 8 participants completed the entire course of 8 treatment sessions within 3 weeks. There were 1 male and 3 females, ages 30–55, in Group S, and 1 male and 3 females, ages 51–65 in Group S+H. Demographic and clinical characteristics of the participants are summarized in Table 3.
Demographic and Clinical Characteristics of Participants
yrs, years.
After treatment, the mean RMQ score for Group S was reduced from 8.50 (before treatment) to 4.25 (after treatment). This statistically significant lower RMQ score, P = 0.0030, was noted after treatment than before treatment. The after-treatment RMQ score had a 50% reduction from before treatment for Group S. The mean RMQ score for Group S + H was also reduced from 8.00 (before treatment) to 3.25 (after treatment). This after-treatment score was significantly lower than the before-treatment score at P = 0.0021. After treatment, the RMQ score was 58% reduced from before treatment in Group S+H. Analysis of the RMQ scores is shown in Table 4 and Figure 1.
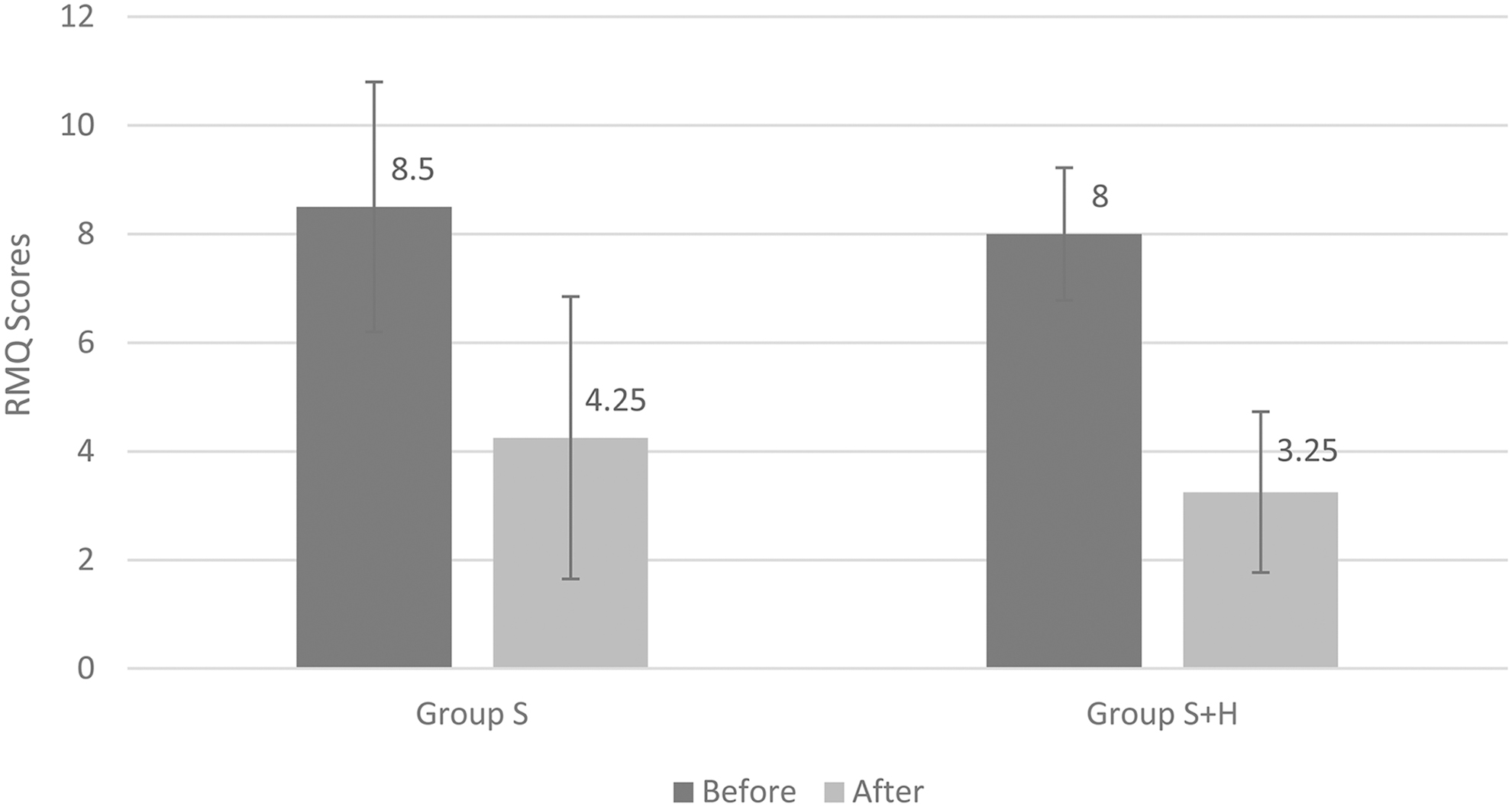
Roland–Morris Questionnaire
Roland–Morris Questionnaire for Disability Scores Before and After Treatment
Bolding indicates significant results.
SD, standard deviation.
The mean NRS score for Group S was reduced from 2.88 (before) to 1.38 (after), with a 52% reduction. However, this reduction was not statistically significant (P = 0.0691). Group S + H had a statistically significant reduction from a mean score of 4.13 to a mean score of 0.50 (P = 0.0006). This was an 88%percentage reduction was for Group S+H. An analysis of the results of the NRS scores is shown in Table 5 and Figure 2.

Numeric Rating Scale (NRS) for pain scores before and after treatment.
Numeric Rating Scale for Pain Before and After Treatment
Bolding indicates statistically significant result.
SD, standard deviation.
There were no side-effects in either group, based on clinical observation. No participants reported adverse effects during the study. On a poststudy survey, all participants reported that they were unaware of which groups they were in.
DISCUSSION
In Group S+H, both RMQ and NRS scores showed significant improvement in disability symptoms and LBP. In Group S, RMQ score showed significant improvement for disability symptoms but not in the NRS score for LBP. This was probably due to the small sample size of the study. However, Group S + H had a higher percentage reduction in both RMQ and NRS scores after the treatment. This suggests that heat therapy using sea salt combined with Chinese herbs may work better than warm sea salt alone. Larger clinical trials are both feasible and warranted. In addition, no obvious side-effects were observed after 8 treatment sessions. These results suggest that heat therapy with sea salt and Chinese herbs is an effective treatment for cLBP and disability caused by LDH. These results also also suggest that this therapy is a safe and promising alternative to pharmaceuticals and even surgery for patients with cLBP caused by LDH.
Limitations of this study included its small sample size, single-blind design, and lack of a placebo control. However, the randomization, single blinding, and controlled study design were successful. This suggests that it is feasible to conduct larger clinical trials with improved designs to support the current study's results. In addition, the variation of the disease course between the 2 groups might have affected the results. A larger sample size will resolve this issue in future studies. Meanwhile, a 2-month follow-up after treatment will be needed to evaluate the long-term efficacy of the therapy.
The herbal sea-salt bag and Zheng Gu Shui used in the study were used based on the diagnosis of Bi Syndrome in acupuncture theory with the patterns of Blood Stasis, Cold and Dampness, and Kidney Deficiency. Duo Huo, Dang Gui, San Qi, Du Zhong, Sheng Jiang, and Hong Cong Tou were used to promote blood circulation and remove Blood Stasis, dispel Cold and Dampness, as well as supporting Kidney energy. In this study, no further pattern differentiation diagnosis was attempted. Improvement was found for all participants, suggesting that the formula works for most patients with cLBP due to LDH. However, detailed pattern differentiation for each patient, and individualized acupuncture and moxibustion therapy, may still help improve clinical efficacy in everyday practice.
Granulated herb is a form of herbal extract that preserves active ingredients and some aromatic essences. People can smell volatilized herbal fragrance easily after an herbal salt bag is heated. When a warm herbal sea salt-bag is used on the human body, the aromatic essence and active ingredients may penetrate the skin together with the heat. External use of herbal granulates with warm sea salt has not been well-studied. Future research may focus on the efficacy of a warm herbal sea-salt bag alone, not together with Zheng Gu Shui as was done in this study.
Preparation of an herbal sea-salt bag is quick and easy. The materials used are also inexpensive. This bag may be a sustainable option for patients who are sensitive to the cost of treatment. The herbal sea-salt bag can even be used conveniently at a patient's home to manage pain and related symptoms. Zheng Gu Shui is also readily available. Meanwhile, moxibustion, heat therapy involving burning moxa on acupoints, is a common practice in acupuncture offices for LBP. However, smoke from burning moxa can be a hazard in a common office setting, and moxa skin burns have also been reported as adverse events from moxibustion. 19 Thus, the combination of a warm herbal sea-salt bag and Zheng Gu Shui can be an alternative to moxibustion in an acupuncture office. This bag can also be an adjunct to physical therapy.
CONCLUSIONS
Although conducted with a small sample size, a single blinded design, and lack of a placebo control, this study found that heat therapy using sea salt combined with Chinese herbs was an effective and safe alternative to drugs and surgery for cLBP due to LDH. The combination of heat therapy and Chinese herbs may work better than the heat alone to reduce LBP and reduce disability symptoms due to LDH. It is feasible to conduct larger clinical trials to support the results of this current study.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this study.