
Abstract
ABSTRACT
Background:
Trigger fingers is a condition that causes locking/stiffness due to inflammation and hypertrophy of the tendon sheaths. This inflammatory process occurs due to degenerative conditions, such as aging, chronic daily overuse, and other factors such as metabolic disorders.
Case:
A 51-year-old woman had grade IIIb trigger finger on her right hand for ∼2 months before going to an outpatient clinic. She also had stiffness and swelling for a longer time but it felt more severe by the time she presented at the clinic, thus, interfering with her work and quality of life (QoL). She was given acupuncture with low-level-laser therapy, using a low-energy laser, 3 times per week, on her right hand. The unilateral points used were LU-10 Yuji, LI-4 Hegu, PC-6 Neiguan, LI-11 Quchi, GB-21 Jianjing, and an Ashi point on the first finger of the metacarpophalangeal [MCP-I] joint). The bilateral body points used were ST 36 Zusanli and LR-3 Taichong.
Results:
After 12 sessions of therapy, there was a decrease her numerical rating scale (NRS) score of 6/10 to an NRS score of 0/10. She also had an improvement in her QoL, as measured by the Short Form-36 and Quick-Disabilities of the Arm, Shoulder and Hand instruments.
Conclusions:
Laser acupuncture may be considered for treating pain and improving QoL of patients with trigger finger. In addition, laser acupuncture causes minimal side-effects, compared with other medical treatments.
INTRODUCTION
Worldwide, the incidence of trigger finger occurs in ∼28 of 100,000 individuals every year, with a prevalence of 2%–3% in the general population. Trigger finger is 6 times more common in women than in men with ages 40–60.1–6 The cause of trigger finger is still unknown, but predisposing factors are female gender, rheumatoid arthritis, repetitive use of the fingers, and carpal tunnel syndrome. 7
Trigger finger—also known as stenosing tenosynovitis—is a condition in which one or more fingers have locking/stiffness due to inflammation and hypertrophy in the tendon sheaths. The diagnosis of trigger finger, itself, can be established through anamnesis and physical examination. Generally, the patient will feel pain and difficulty in moving the finger and/or experience the finger as being “locked” in flexion or extension positioning. On physical examination, in addition to the fingers being locked in flexion or extension, local edema or nodules may also occur.2,4,5,8
Treatment for trigger finger depends on the severity and duration of the patient's symptoms. Noninvasive therapy—including a combination of nonsteroidal anti-inflammatory drugs, massage, and splinting—can be given to patients with uncomplicated cases. If noninvasive treatment fails, then a corticosteroid injection may be made into the tendon sheath prior to surgery to release the locking on the A1 pulley. 9 Corticosteroid injections and surgery are still therapeutic options, 10 but frequent applications of this treatment has been reported to damage the tendons or tendon sheaths, so this treatment is still limited. 11 In addition, steroid injections only provide benefits in for a short term but not for a long term, so the recurrence rate is quite high. 12
Existing research suggests that acupuncture can improve local blood circulation and reduce inflammation by releasing anti-inflammatory cytokines. A study by Inoue et al. indicated that acupuncture may help improve conditions characterized by chronic local inflammation. 11 Low-level laser therapy (LLLT) is a noninvasive therapy with a conservative therapeutic method that is effective for accelerating healing and producing an anti-inflammatory effect by stimulating the involved tissues. Significant pain reduction has been demonstrated for a variety of musculoskeletal conditions. 12
CASE
A 51-year-old married woman, in menopause, reported that she could not bend the thumb of her right hand since 1 week prior to presenting, and that the condition was painful (6 on a numeric rating scale [NRS]). From her anamnesis, it was known that she had felt stiffness and pain in the joint of the thumb of her right hand for the last 2 months, and that, in the previous week, the intensity of her pain had been growing stronger every day, especially when she engaged in activities involving gripping, such as squeezing laundry, mopping, and writing; thus, this condition interfered with the patient's daily activities. She described the pain as stabbing and reported that it was reduced with drugs such as 500 mg of paracetamol. This pain also radiated from her thumb to the back of her hand. Sometimes, she had difficulty sleeping due to this pain.
She was given LLLT. This consisted of multilead laser acupuncture therapy with a laserneedle touch solution, (Original Laser Needle®, Germany), class 3R with an optical power of 40 mW per channel and a wavelength of 658 nm. The probe diameter was 1 mm and the power density was 4 W/cm2. The unilateral points treated were only on her right hand (LU-10 Yuji, LI-4 Hegu, PC-6 Neiguan, LI-11 Quchi, GB-21 Jianjing, and an Ashi point on the first finger of her metacarpophalangeal [MCP] joint). Two bilateral body points were treated at ST-36 Zusanli and LR-3 Taichong with a movement/ mesenchymal frequency (an 1168-Hz pulsed-wave Nogier-C laser) at 4 Joules per point for 7 minutes. This acupuncture protocol was performed 3 times per week for a total of 12 therapy sessions.
RESULTS
After undergoing 12 sessions of acupuncture therapy, this patient's range of motion (ROM) in her MCP-I flexion improved from 33o to 133o since her second treatment and lasted up to 8 weeks after the last treatment (Fig. 1). The patient's NRS pain scale score decreased from 6/10 to 0/10 after her eighth treatment and this improvement continued for the next 2 months (Fig. 2). Her QoL scores, as measured with the Short Form–36 (SF-36) and Quick-Disabilities of the Arm, Shoulder and Hand (Q-DASH) instruments (Figs. 3 and 4).

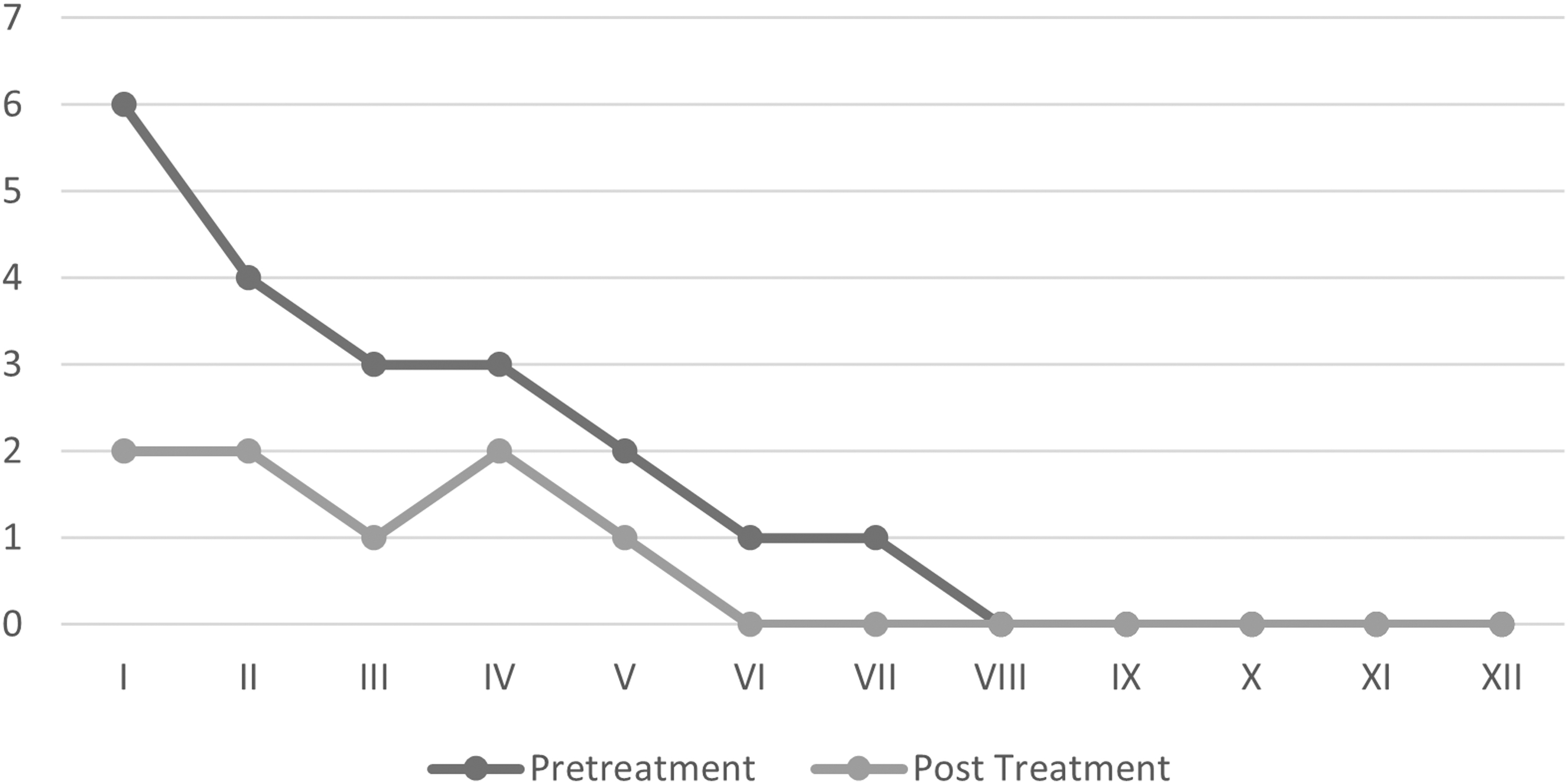
NRS scores pretreatment and post-treatment: 12 sessions of laser acupuncture therapy. NRS, numeric rating scale.
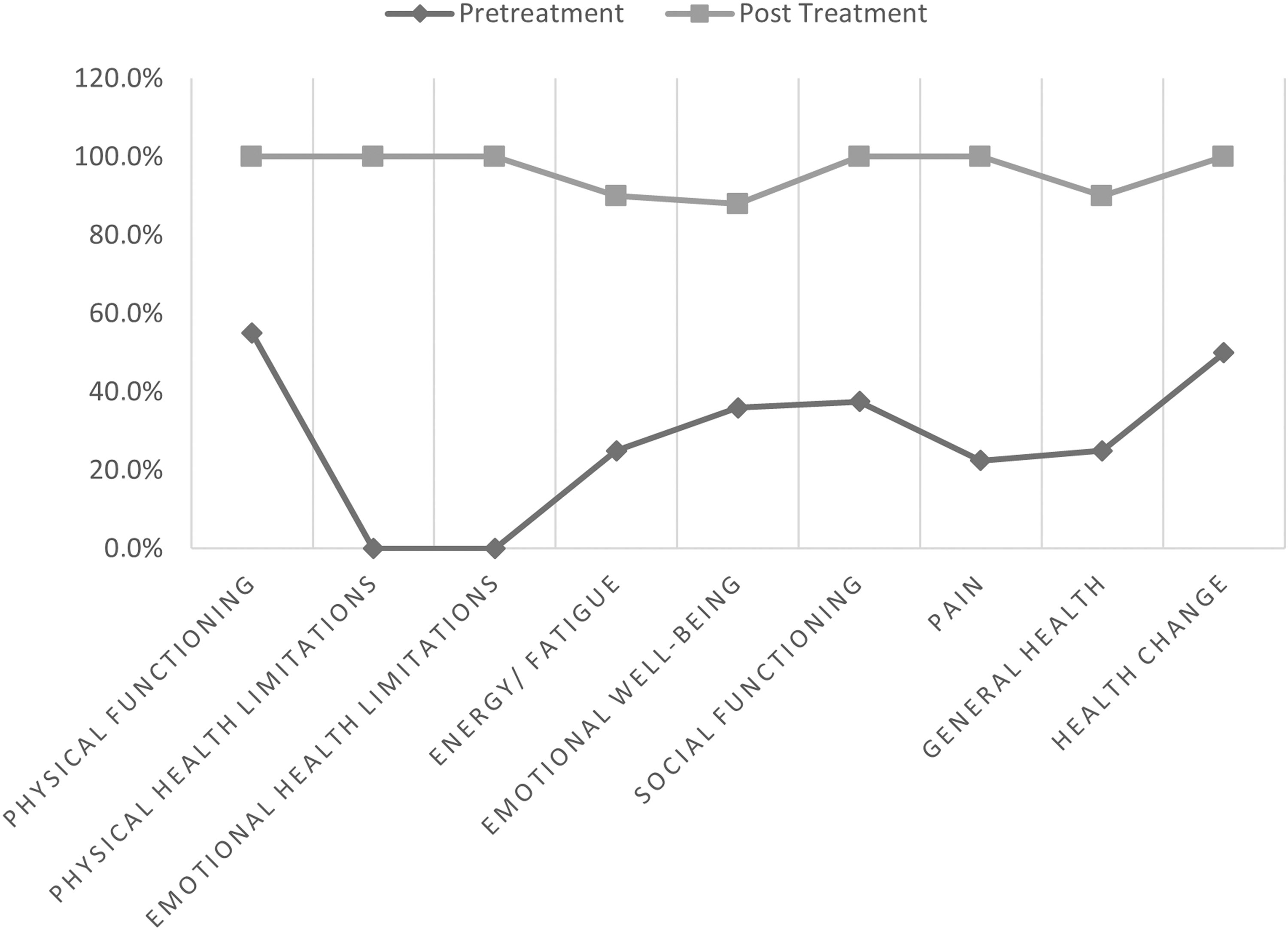
SF-36 Scores pretreatment and post-treatment: 12 sessions of laser acupuncture Therapy. SF-36, Short Form–36.

Skor Q-DASH pretreatment and post-treatment: 12 sessions of laser acupuncture therapy. Q-DASH, Quick-Disabilities of the Arm, Shoulder and Hand.
DISCUSSION
This case report described the role of laser acupuncture in overcoming pain due to trigger finger in a 51-year-old woman, who had pain in her right thumb and was unable to bend it for 1 week before going to the clinic. To establish the diagnosis of trigger finger in this patient, a comprehensive examination was carried out starting with the anamnesis, physical examination, and other supporting investigations, such as laboratory values, radiology, and ultrasonography. A differential diagnosis of osteoarthritis (OA) was ruled out by the radiologic examination, as there were no signs of OA, such as spurs or narrowing of the joint space. The swelling and stiffness in this patient's thumb, also did not indicate the symptoms of rheumatoid arthritis (RA) when further anamnesis did not reveal bilateral symmetrical pain or involvement of many joints. In addition, she did not have any systemic symptoms of RA. A diagnosis of de Quervain syndrome was ruled out by a physical examination with a negative Finklestein test.
Acupuncture therapy was given to this patient, using a multilead laser modality (Original Laser Needle,® made in Germany) with a Nogier-C pulsed wave at an 1168-Hz frequency, 40 mW optical power, and 4 Joules/point for ∼7 minutes. This dose is in accordance with Naeser's recommendation, which is 4 Joules for both muscle and joint pain. 13 The recommended treatment time (TT) described by Kreisel and Weber, 14 involved setting the laser needle a with resonance mode for 40-mW power and a 4-Joules dose, for a TT of 7 minutes on each point. The reason for using the C-wave laser was that it is for disorders related to the locomotor system (movement/mesenchymal frequency). 14
It is believed that, for body acupuncture, one must reach the nociceptive structures that lie 2–3 cm underneath the skin's surface. To achieve this depth, the wavelength must be between 605 nm and 850 nm, which can be reached by red and infrared lasers. 15
This patient received acupuncture therapy 3 times per week (1 series), for a total of 12 therapy sessions. This was in accordance with a study conducted by Aranyavalai et al. that produced improvement in patients' NRS scores and lasted up to 3 months. 12
The acupuncture therapy consisted of LLLT treatments on right hand unilateral points at LU-10, LI-4, PC-6, LI-11, GB-21 and an Ashi point (at MCP-1) as well as 2 body points bilaterally at ST-36 and LR-3. This was in accordance with Wu et al.'s research, which found that functional magnetic resonance imaging (fMRI) showed that acupuncture induced an activation of brain areas on puncturing the LR 3 point, which specifically regulates brain areas in the cingulate gyrus, thalamus, and posterior lobes of the cerebellum associated with sensation and analgesia. 16
Wei et al. also stated that stimulation of ST-36 will activate regions in the brain, including the prefrontal lobe and anterior cingulate cortex with respect to their functions as pain modulators; this was seen on fMRI images. 17 In addition, other points, such as LU-10, LI-4, PC-6, LI-11, and GB-21, were chosen because they fit the thumb dermatome, sixth cervical (C-6) level; this was in accordance with a study conducted by Ferreira et al. 18 These researchers wrote that there is a relationship between acupuncture points and their dermatomes, both in terms of mechanism of action, as well as in indications conforming with existing evidence-based studies. 18
In the current case, LLLT was used, which has been proven to increase the proliferation of fibroblast cells, keratinocytes, endothelial cells, and lymphocytes. The proliferative mechanism occurs due to mitochondrial photostimulation that causes activation of signaling pathways and upregulation of transcription factors, leading to an increase in growth factors. LLLT can also increase neovascularization, promote angiogenesis, and increase collagen synthesis to help heal acute and chronic wounds. LLLT, at the correct dose, will decrease the mitochondrial membrane potential in the dorsal root ganglion and the production of adenosine triphosphate, resulting in a nerve blockade. The effect of this nociceptor blockade is pain relief that occurs within a few minutes. The medium-term effect of using LLLT is reduction in local edema and inflammation within hours-to-days. While the long-term effects will occur within 1–2 weeks, these effects can last for months-to-years as a result of better tissue healing. 19
The current patient was also followed up for 8 weeks after her acupuncture therapy was completed and the results of the LLLT were still felt. Her pain reduction was assessed using the NRS, and her QoL was assessed using the SF-36 and Q-DASH scoring systems. After undergoing acupuncture, she had a very significant change in her pain and improvement in various aspects of her QoL.
All examination procedures, from the beginning of therapy to the end of the therapy, as well as the follow-up, were approved by the patient for this case presentation. She has been given informed consent.
CONCLUSIONS
Acupuncture has a curative role for handling trigger finger cases.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
No funding was received for work on this article.