
Abstract
The dynamic pulse reaction (Nogier reflex), Reflex-Auriculo-Cardiac (RAC), or vascular autonomic signal is a physiologic phenomenon that is not fully accepted and widely understood in contemporary medical practice. In order to provide appropriate scientific evidence for better understanding, qualitative and—above all—quantitative research in this area is necessary. In this short report, 2 recordings of dynamic pulse reactions based on an analysis performed on a modified smartphone are demonstrated during laser acupuncture experiments using stimulation at ear acupuncture points.
INTRODUCTION
The importance and targeted application of the dynamic pulse reaction—or the Nogier reflex or the Reflex-Auriculo-Cardiac (RAC) or the vascular autonomic signal—are, so far, almost unknown in conventional medicine. 1 The RAC can be felt with the fingertip by a trained medical person while different stimuli are applied to the patient at the same time.
A multinational research project among renowned research institutions in Taiwan and the Research Center for Traditional Chinese Medicine (TCM) at the Medical University of Graz, Austria, started before the COVID-19 pandemic. For the first time, scientific attempts were made to quantify changes in the dynamic pulse response by using highly technical methods. The results, recorded for the first time with a modified smartphone, should serve as an important source of inspiration and basic research for possible further applied research by other scientific teams.1,2
FROM NOGIER'S OBSERVATIONS TO LASER-CONTROLLED ACUPUNCTURE
The dynamic pulse phenomenon or reaction was first described by Paul Nogier, MD, in the 1970s.3–5 He was of the opinion that most body cells react to stimuli from the autonomic nervous system (ANS). Dr. Nogier was therefore looking for a method to show the body's reaction to acupuncture-induced measures. He discovered that mechanical pressure on specific points at the ear elicited a cardiovascular response. He called this reaction the reflexe auriculo cardiaque (Reflex-Auriculo-Cardiac); later it was also abbreviated to RAC or termed the dynamic pulse reaction (to distinguish it from Chinese static-pulse diagnosis).1,5 In research by Bahr et al. for practical application in auricular medicine, the RAC signal served as both a diagnostic and a therapeutic tool. 6 Use of the RAC signal enabled the development of interference-field acupuncture7,8 as well as the therapeutic so-called “controlled acupuncture,” in which the acupuncture needle is positioned dynamically under pulse control and is not based on cun and other units of measurement as in the classical Chinese tradition. 6
Litscher et al. 9 wrote an original article in Integrative Medicine International in 2014. Together, the Austrian, the German and Chinese researchers focused on a new method in auricular medicine for investigating the Nogier reflex. A new high-resolution imaging method for recording pulsatile surface changes made it possible, for the first time, to quantify the RAC reproducibly without statistical analysis. This method combines an innovative microscope system, video analysis software, and special image-processing software (from the Beijing University of Science and Technology). Even small, pulse-dependent changes in the skin surface became clearly visible. 8
From Moser et al., 10 also from the Medical University of Graz, in Austria, proof was published in 2017 that the RAC follows physiologic laws quite well. The study built on an earlier series of tests based on heart-rate variability (HRV) measurements and analysis, and demonstrated various reproducible changes in physiological parameters. A total of 7 parameters and various external noninvasive stimuli were recorded under a defined setup and test course. The researchers hypothesized that the RAC is a manifestation of a cardiac response in the ANS, which then initiates a pulse wave. They concluded that using a subtle stimuli close to the perceptual limit should enable repeatable testing of immediate and sympathetic responses.8,10
Technology and application presented recently1,2 focusses now on a modified smartphone-based registration of pulse activity and can be applied to both static and dynamic pulse reactions.1,2 The system was implemented on the Android platform. A user interface was integrated on the phone that enabled the user to start or stop the sensor data collection and view the obtained signal in real time. The measured data were first stored in the phone and then transmitted to the cloud server at the end of each measurement session.1,2
The hardware architecture of this innovative system is divided into 3 parts: (1) the sensors; (2) the smartphone per se; and (3) the cloud server section. The sensors first register photoplethysmography signals from the patient and transfer them to the smartphone via the on-the-go cable. The mobile unit then transmits the data wirelessly (as already mentioned) to the cloud server. It is anticipated that the RAC can be predicted by using artificial neural networks.1,2,11
RESULTS
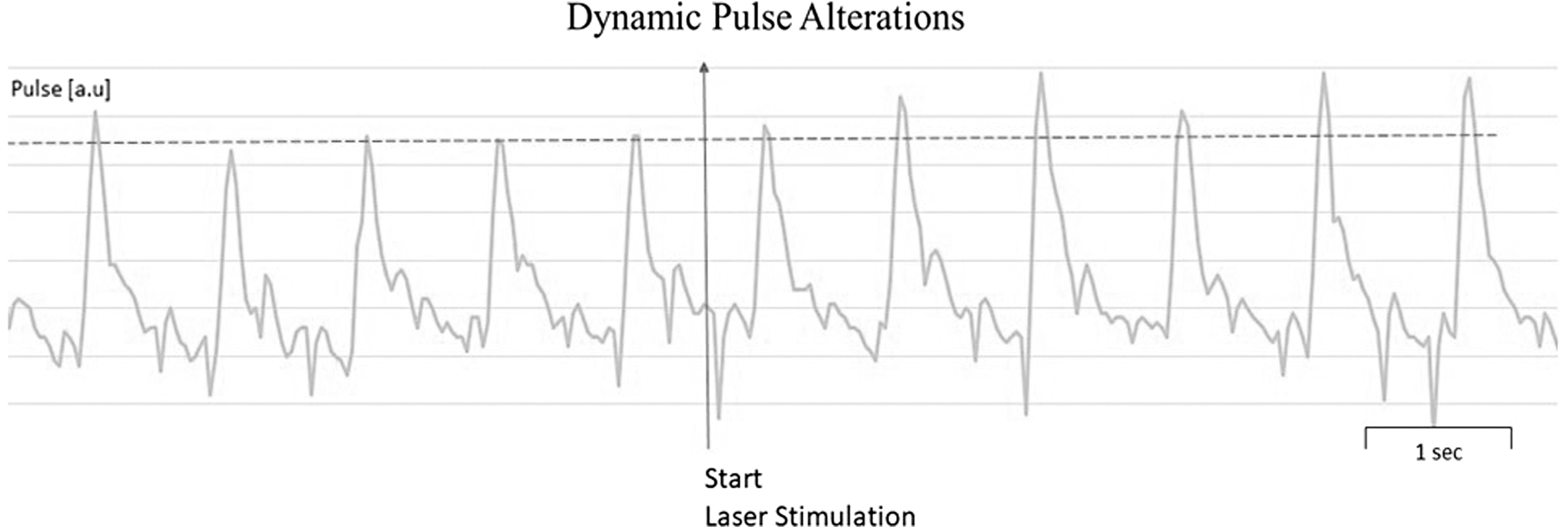
Figure 1 shows the dynamic pulse response immediately after being triggered by laser stimulation at the Shen Men ear point (810 nm, 150 mW, 30 seconds) in a 26-year-old female with a sleep disorder. In this case mainly, the changes in amplitude in the pulse signal from the radial artery can be seen clearly. Data were recorded via an adapted smartphone. 2

Dynamic pulse response triggered by laser stimulation at the Shen Men ear point in a 26-year-old female patient immediately before and immediately after the onset of laser acupuncture stimulation with near-infrared light on the ear.
In Figure 2 the dynamic pulse response triggered by laser stimulation at the Stomach ear acupoint (810 nm, 150 mW, 30 seconds) is shown in a 53-year-old male with functional dyspepsia. Again, the changes in amplitude in the pulse signal from the radial artery can be seen clearly.
Dynamic pulse response (Reflex-Auriculo-Cardiac) triggered by laser stimulation at the Stomach ear point in a 53-year-old male.
The investigations, which included only noninvasive measurement methods, were approved by the local ethics committee of the Changhua Christian Hospital, in Taiwan. Both patients showed clinical reductions of their symptoms. However, we could not make an exact determination if any of the demonstrated RAC changes had any clinically significance.
LIMITATIONS
The present short report has some methodological deficiencies. Only 2 examples are shown, which were not verified by control measurements. In addition, the data resulted from 2 patients with 2 different clinical conditions. Nevertheless, due to the new technical procedure involved, it seems justified to release this publication for interested persons in the scientific community and to show where the methodological development in this exciting field of research can go.
DISCUSSION
RAC research is indeed entering a new phase in which modern information technology and artificial intelligence (AI) will play a major role. In the future, the RAC could be quantified and documented by using adapted smartphones with integrated sensors and AI analysis methods (neural networks; Fig. 3).1,2,8

Reflex-Auriculo-Cardiac analysis using an adapted smartphone.
Of course, average heart rate, HRV, modulation of amplitude, and Fourier-wave transforms might all be obtained from the data. This type of array may ultimately relate to diagnosis and treatment. In addition, the dynamic pulse response might offer another avenue for investigating point specificity.
AI will help clinicians make better medical decisions by registering, storing, and analyzing RAC data. That is the theory. In practice, however, it is often difficult to convert the changes in heart rate data into usable information. The requirements of the physicians are too different; the influencing factors are too diverse.
CONCLUSIONS
This is the reason why we are already taking the opposite step again today and the human factor is playing a greater role again. From the our point of view, the greatest difficulty lies in including human perception in the RAC analysis process. The solution to these questions can only be that AI and information technology processes in RAC research cannot—and should not—be a substitute for the human factor but, rather be the basis for its data-supported decision-making.1,2,7,8,11
Footnotes
ACKNOWLEDGMENTS
The authors of this short report would like to thank all members of the Initiative for Medicine without Side Effects (a non-profit association) and, of course, especially its president, Frank R. Bahr, MD, for the support provided to the Medical University of Graz before the COVID-19 pandemic.
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
No funding was obtained for work on this article.