
Abstract
Objective:
Knee flexion exercise is a type of exercise therapy for improving knee-joint muscle strength. Among the knee extensors, the vastus medialis muscle is less active and prone to disuse atrophy. The effects of press needle acupuncture include vasodilation, which may affect blood flow in the vastus medialis. This study examined the effects of exercise stimulation + press needle stimulation on muscle blood flow.
Materials and Methods:
Conducted in Teikyo Heisei University, Tokyo, Japan, this randomized controlled trial involved 30 healthy adults in 3 groups (10 who did not receive stimulation, 10 who received exercise stimulation only, and 10 who received press needle stimulation + exercise stimulation). The stimulations were applied once per week, for 3 weeks. After resting for 10 minutes, the nonstimulated group rested for 2 additional minutes, and the other 2 groups performed knee flexion and extension exercises considered to be “very very hard on the Borg rating.” After this activity, the 2 stimulation groups rested for 10 minutes. Press needle stimulation was applied on the vastus medialis muscles of both thighs in the combination stimulation group.
Results:
The combination group had a smaller decrease in muscle tissue oxygen saturation and an increase in total hemoglobin, compared to the exercise only stimulation group.
Conclusions:
Press needle stimulation during exercise may dilate muscle blood vessels. Future studies should examine the effectiveness of this stimulation for age-specific and knee diseases.
INTRODUCTION
Human muscle fatigue is a reduction in the force-generating capacity of muscles induced by exercise. 1 Given that human performance and muscle fatigue are closely related, muscle recovery can be considered the recovery of force after exercise. 2 While skeletal-muscle blood flow is regulated by multiple mechanisms, such as the reflex function via the central nervous system, it has been reported that hyperemia due to sustained skeletal-muscle exercise is primarily due to metabolic vasodilation and increased vascular conductance via the skeletal-muscle pump. 3
Near-infrared spectroscopy (NIRS) devices have been used in sports medicine to measure oxygen (O2) status noninvasively in specific muscles and brain regions. Muscle-tissue O2 saturation (StO2), which can be measured by NIRS, reflects the balance between O2 supply and consumption in muscle tissues. 4 In addition, O2 dynamics in localized regions of skeletal muscle during exercise and recovery have also been revealed through the use of NIRS light.5,6 Therefore, NIRS is an optimal modality for evaluating changes in tissue oxygenation during exercise.
Knee flexion exercises comprise a type of exercise therapy that increases general knee-muscle strength. Among knee extensors, the vastus lateralis muscle has the largest muscle mass and extension force. In contrast, the vastus medialis muscle is less active and is the weakest and most-vulnerable muscle in the extensor mechanism. 7 As the vastus medialis is prone to disuse atrophy, recovery after injury is frequently challenging. Indeed, that muscle is most often in need of rehabilitation after knee fusion, injury, or surgery. 7
The effects of acupuncture stimulation trigger various physiologic responses via the autonomic nervous system (ANS), 8 including increases in skin temperature and skin and muscle blood flow.9,10
The press needle is a type of acupuncture needle. 11 Ordinary acupuncture needles are filiform and cannot be moved in the body if they remain inserted. Press needles, however, have a very short insertion depth and do not penetrate the muscle but remain in the skin. Therefore, the needle does not break and there is no risk of it entering the body. In addition, because the press needle is fixed with a seal, that needle can be affixed to the body while a person is exercising.
Using a press needle during exercise may reduce muscle fatigue and prevent vastus medialis muscle weakness. Nevertheless, no prior studies have evaluated the combined effects of press needles + exercise. If the decrease in StO2 during exercise can be suppressed, early recovery from muscle fatigue can be expected. This study evaluated the efficacy and safety of press needles + exercise stimulation on the vastus medialis muscle before, during, and after exercise in healthy adults.
MATERIALS AND METHODS
Participants
This study was conducted in accordance with the tenets of the Declaration of Helsinki. 12 The purpose, methods, and potential outcomes of the study were explained to all participants, after which written informed consent was obtained.
A total of 30 healthy adult men were randomly allocated to the following 3 groups: (1) control group (no exercise stimulus; n = 10; age, 22.1 ± 0.5 years; body mass index [BMI], 21.8 ± 1.92 kg/m2); (2) exercise-only stimulation group (exercise only; n = 10; age, 21.6 ± 0.7 years; BMI, 21.7 ± 3.33 kg/m2); and (3) combined press needle + exercise stimulation group (n = 10; age, 21.3 ± 0.6 years; BMI, 21.9 ± 2.68 kg/m2). The allocation method utilized dedicated randomization software. Exercises were performed by participants once per week for 3 weeks. A parallel-group, randomized trial was thus performed and started with examining the subjects' baseline muscle-blood flow.
Participants were required to refrain from eating or drinking anything other than water (e.g., alcohol, caffeine-containing beverages such as coffee and tea) 2 hours before the day of the experiment to avoid effects on the ANS. The room temperature was standardized at 24°C–27°C.
Intervention Method
Exercise Stimulation
The exercise stimulus was comprised of a knee-flexion/extension movement (180°/second). A metronome was used to guide each subject to flex and extend his knee once per second. Each participant was also instructed to perform the exercise with his arms crossed and held to his torso to avoid arm recoil. The knee-flexion angle was the participant's maximum flexion and extension position (Fig. 1). The exercise intensity was set to “very, very hard on the Borg scale” 13 of perceived exercise intensity. Participants in the control group were assessed seated during the 2-minute rest timeperiod.
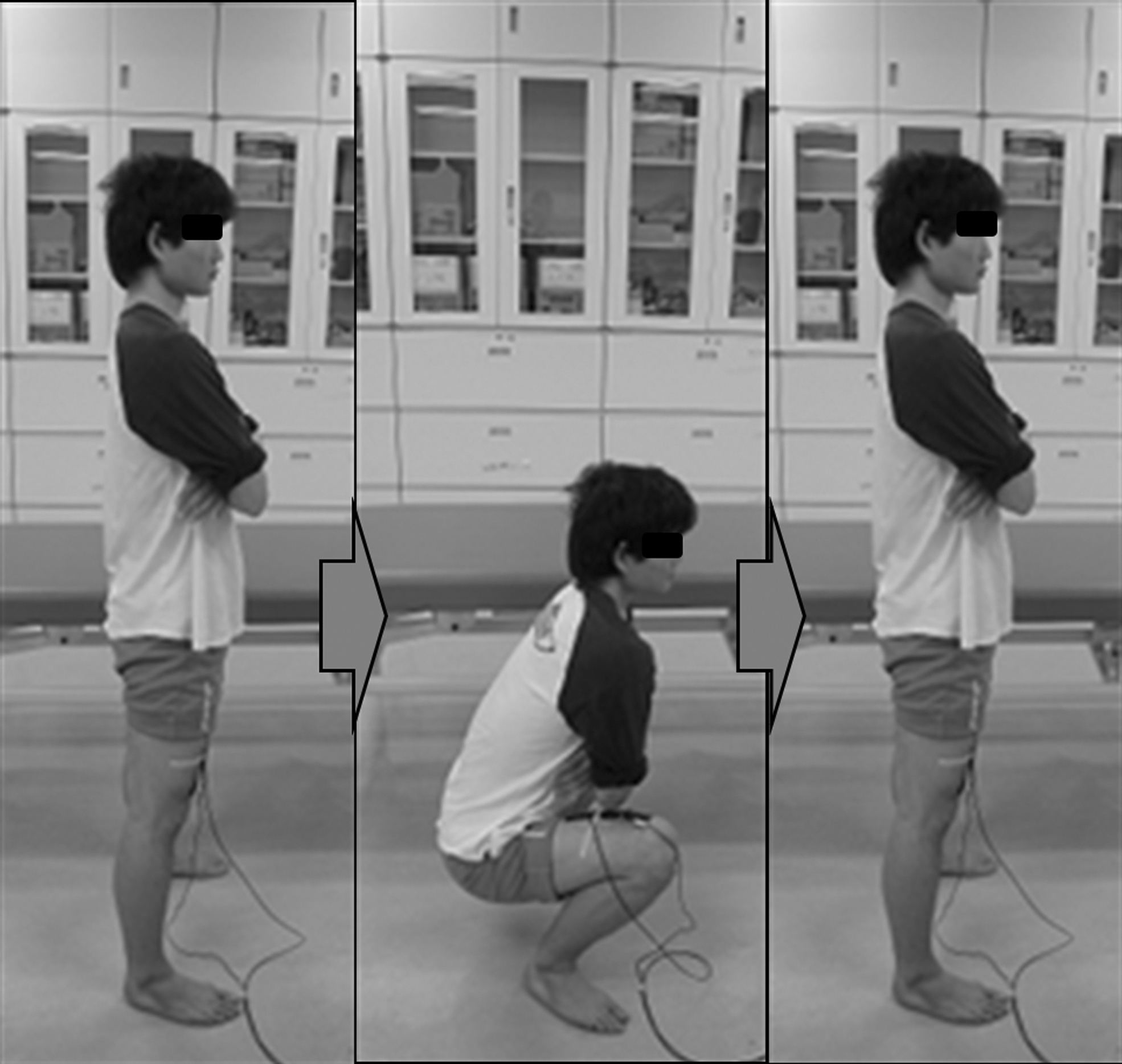
Knee-flexion/extension movement. A metronome was used to guide the subjects to perform the knee-flexion/extension exercise once per second. Participants were also instructed to perform the exercise with their arms crossed and fixed to their torsos to avoid arm recoil. The knee-flexion angle was the participant's maximum flexion/extension position.
Press Needle Stimulation
Two stainless-steel press needles (length, 1.2 mm; diameter, 0.20 mm; SEIRIN,® Shizuoka, Japan) were used and were fixed using a 10-mm-diameter circular tape. The press needles remained attached to the subjects in the combination stimulus group throughout the exercise part of experiment. For each subject the needle was applied to the most distended area of the vastus medialis muscle in the quadriceps muscle of both legs. SP-10 (Xuehai) was the acupoint used (Fig. 2). 14 The press needles were initially affixed and removed after the rest and exercise session and at the end of the rest period. New press needles were affixed each time the subjects exercised. Potential adverse events, such as pain and internal bleeding due to the press needle and itchy skin due to the attached tape, were monitored.

Press needle site. Press needling was applied to the most-distended area of the medial vastus medialis of the quadriceps muscle on both legs. Moreover, in terms of meridians, this was the SP-10 (Xuehai) acupoint. 1
NIRS
Muscle-blood flow measurements were obtained using a functional test oximeter (OMEGAWAVE Inc., Tokyo, Japan). StO2 (%) and total hemoglobin (Hb; an arbitrary unit) were assessed before, during, and after exercise stimulation. NIRS utilizes 3 wavelengths of near-infrared spectra from the main unit through a probe (light transmitter) applied to biologic tissue and receives the light with a detector (receiver); changes in tissue oxygenated blood volume, tissue deoxygenated blood, tissue total Hb, and StO2 are measured in absolute amounts via changes in the intensity of light received. The distance between the light transmitter and receiver is 1.5–3.0 cm. Thus, the NIRS measurement depth can be estimated to be 1.5–3.0 cm from the skin surface to the muscle tissue.
For each subject, the NIRS holder was placed near the origin of the vastus medialis muscle, where muscle contraction is small, even during exercise. The holder was secured with black vinyl tape to prevent light from entering through the gap and to prevent the quadriceps muscle from being inhibited during exercise. If the holder was detached during the measurement, the data from that measurement were deleted.
Protocol
Participants rested for 10 minutes in a sitting position. Next, they rested in a supine position (10 minutes). This was followed by the intervention stimulus for the 2 exercise groups (a “very, very hard” on a modified Borg rating” 13 exercise stimulus, while the control group had 2 minutes of seated rest). This modified Borg rating is modified according to the 15-point scale for rating perceived motion, 13 and is classified into 7 categories: very very light; very light; light; fairly hard; hard; very hard; and very very hard. For this study participants performed the “very very hard” exercise until they could no longer perform the knee flexion and extension exercise.
This intervention was performed once per week, 3 times over 3 weeks. NIRS was measured during the 10-minute preintervention supine rest timeperiod, intervention timeperiod, and 10-min postintervention supine rest timeperiod. Press needles were inserted before the supine rest. The press needles were removed after 10 minutes of rest after each exercise session; a new needle was inserted for the next session (Fig. 3).
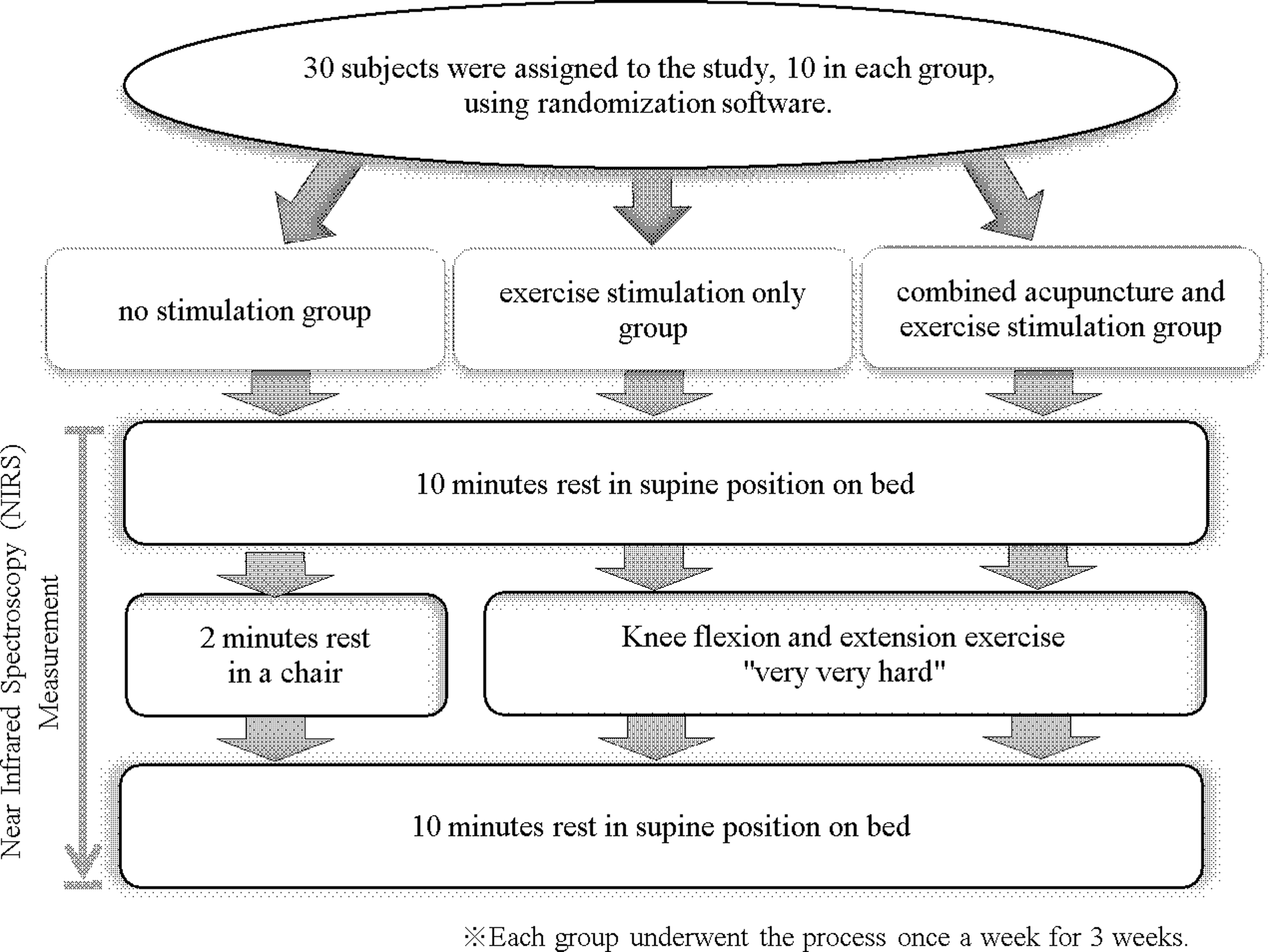
Protocol. Stimulation: The 30 participants were allocated randomly into 3 groups: (1) no stimulation (control); (2) exercise-only stimulation; and (3) combined press needle acupuncture + exercise stimulation. All participants rested in a supine position on a bed for 10 minutes, followed by either no stimulation or exercise stimulation (at a “very hard” intensity for the 2 remaining groups). After the exercise, the participants again rested in a supine position on the bed for 10 minutes. The exercise was performed once per week for 3 weeks. Near-infrared spectroscopy (NIRS) measurement: Measurement timepoints were before exercise (NIRS measured after 10 minutes of supine rest), during exercise (NIRS measured during exercise stimulus), and after exercise (NIRS measured after 10 minutes of supine rest).
Statistical Analysis
NIRS results were expressed as mean ± standard deviation (SD). The control group (no exercise stimulus), exercise stimulation group, combined press needle + exercise stimulation group, and each of the 3 measurement timeperiods (before, during, and after intervention) were set as independent variables. Each mean NIRS value was set as the dependent variable. A 2-way repeated measures analysis of variance was used for comparisons among and within the groups.
The exercise stimulation results were expressed as mean ± SD. The exercise stimulation group, combined press needle + exercise stimulation group, and each of the 3 measurement timeperiods were set as independent variables. The value of each mean was set as the dependent variable. A t-test analysis was used to compare the groups. The significance level was set at 5%. All statistical analyses were conducted with JMP®15 (SAS Institute Inc., Cary, NC, USA).
Ethical Approval
The research plan was approved by the Ethics Review Committee of Teikyo Heisei University, Tokyo, Japan (approval number: 24-050), and was conducted in accordance with the provisions of the Declaration of Helsinki. 12
RESULTS
NIRS measurements were obtained from all 10 participants in the control group during each of the 3 sessions. All 10 participants in the exercise stimulation group were assessed in the first session; however, only 9 participants were assessed in the second session and 8 participants were assessed in the third session. In the combined press needle + exercise stimulation group, 10 participants were evaluated in the first and second sessions, while 8 were evaluated in the third session. Although the 5 aforementioned missing participants continued to perform knee flexion during the exercise sessions, their data were deleted because of detachment of their NIRS holders (Table 1).
St2, Total Hb, and Average Number of Knee-Flexion/Extension Exercises Measured
StO2, muscle-tissue oxygen saturation; Hb, hemoglobin; yrs, years; SD, standard deviation; BMI, body mass index; NIRS, near-infrared spectroscopy; SE, standard error.
NIRS
StO2 Assessment
The exercise stimulation group had significantly lower StO2 during exercise, compared to that during the preintervention timeperiod (P < 0.0001) and postintervention timeperiod (p < 0.0001). The combined press needle + exercise stimulation group also had significantly lower StO2 during exercise, compared to that during the preintervention timeperiod (p < 0.0001) and postintervention timeperiod (P < 0.0001). The exercise stimulation group had significantly lower StO2 during exercise than the control group (P < 0.0001) and the combined press needle + exercise stimulation group (P = 0.0003). The combined press needle + exercise stimulation group had significantly lower StO2 during exercise, compared to the control group (P = 0.0019) See Figure 4.
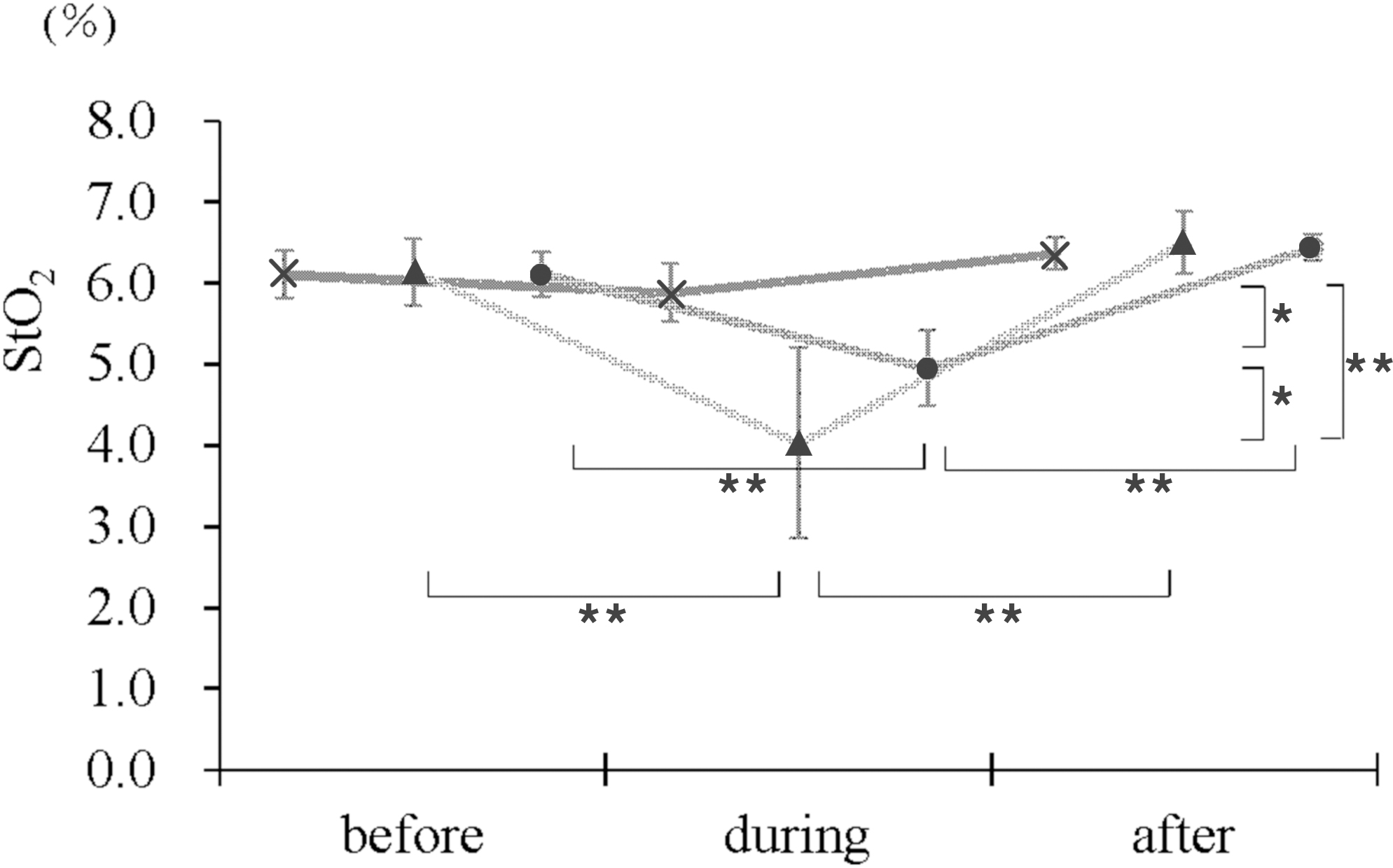
Changes in muscle-tissue oxygen saturation (StO2). StO2 changes are shown for the [ × ] control (no-stimulation) group, the [▴] exercise-only stimulation group, and the [●] combined press needle acupuncture + exercise-stimulation group. The change in StO2 among the groups is shown on the vertical axis. Changes in StO2 within each group before, during, and after exercise are shown on the horizontal axis. On the vertical axis, StO2 during exercise in the [▴] exercise stimulation group was significantly lower (P < 0.0001), compared to that in the [ × ] control group. StO2 during exercise in the [▴] exercise stimulation group was significantly lower (P < 0.0197), compared to that in the [●] combined acupuncture + exercise stimulation group. StO2 during exercise in the [●] combined press needle acupuncture + exercise stimulation group was significantly lower (P = 0.0177), compared to that in the [ × ] control group. On the horizontal axis, StO2 during exercise in the [▴] exercise stimulation group was significantly lower than that before (P < 0.0001) and after (P < 0.0001) exercise. StO2 during exercise in the [●] combined acupuncture and exercise stimulation group was significantly lower than that before (P = 0.0045) and after (P < 0.0001) exercise. Statistical analysis was performed by a 2-way analysis of variance with significance levels of ** P < 0.01 and * P < 0.05.
Total Hb
Total Hb was significantly greater during exercise in the exercise stimulation group than in the combined press needle + exercise stimulation group (P = 0.0032) See Figure 5.

Changes in the total hemoglobin (Hb). The changes in total Hb are shown for the [ × ] control (no stimulation) group, [▴] exercise stimulation group, and [●] combined press needle acupuncture + exercise stimulation group. On the vertical axis, the change in total Hb among the groups is shown. The change in total Hb within each group before, during, and after exercise is on the horizontal axis. On the vertical axis, total Hb during exercise in the [▴] exercise stimulation group was significantly higher (P < 0.0032), compared to total Hb during exercise in the [●] combined acupuncture + exercise stimulation group. Statistical analysis was performed by 2-way analysis of variance, and the significance level was set at * P < 0.05. SD, standard deviation; a.u., arbitrary unit.
Average Number of Knee Extension Exercises
The control, exercise stimulation, and combined press needle + exercise stimulation groups each had 10 participants, and each group underwent 3 sessions as parallel groups. No significant changes were noted in the average number of exercise sets from the first to third sessions among participants in the exercise stimulation and combined press needle + exercise stimulation groups (Fig. 6).
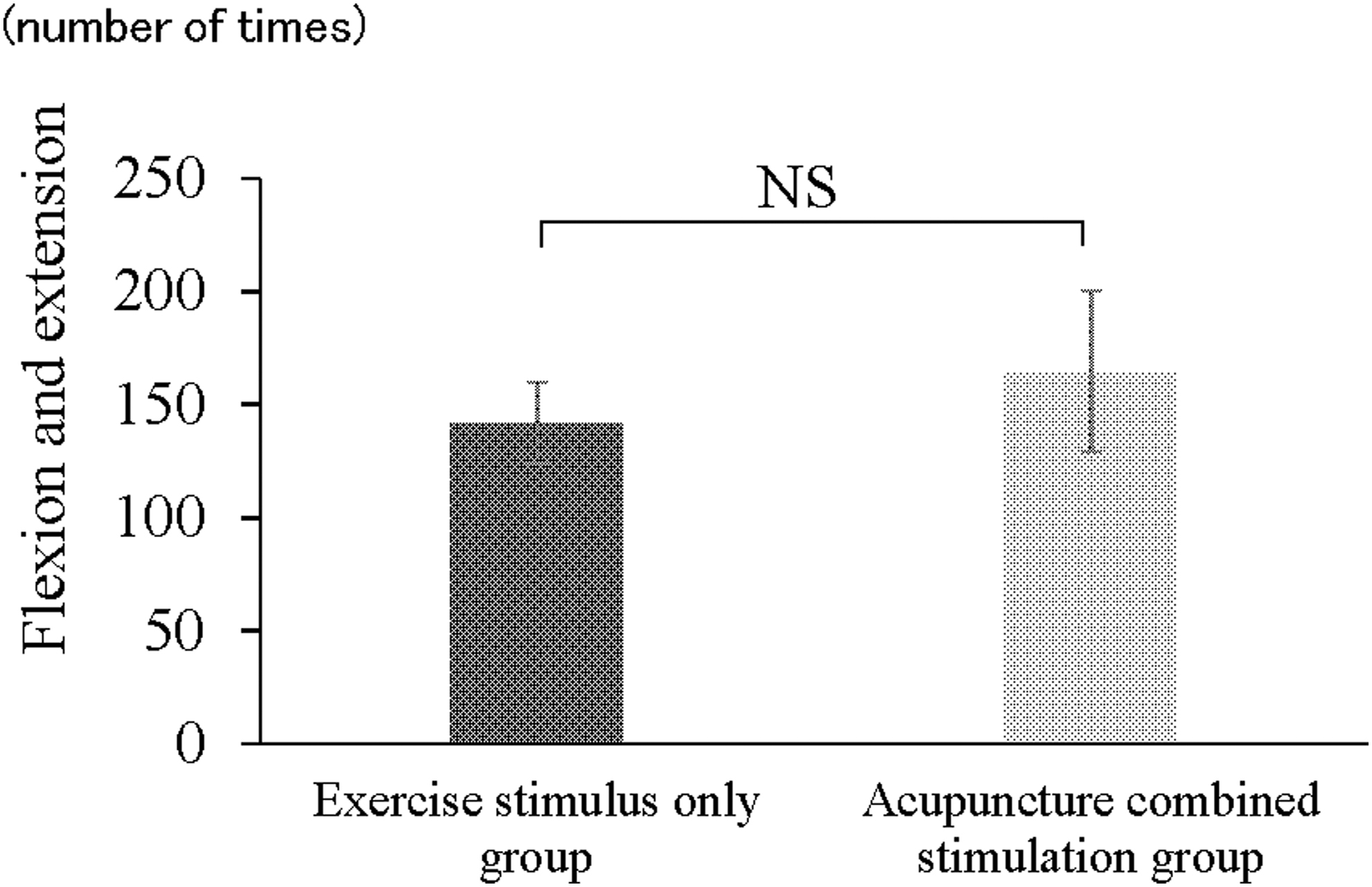
Comparison of the level of exercise stimulus between the groups. The average number of knee-flexion and extension movements (180°/set) across sessions 1–3 is shown for the exercise stimulation group and combined press needle acupuncture + exercise stimulation group. The vertical axis shows the average number of knee flexion/extension exercise sets. The horizontal axis shows the groups who performed exercises. There were no significant differences in the average number of times the exercise was performed. NS, not significant.
DISCUSSION
This study investigated the effects of exercise stimulation combined with press needle stimulation before, during, and after exercise. StO2 during exercise was significantly lower in the exercise stimulation group than in the combined press needle + exercise group. Total Hb during exercise was higher in the exercise stimulation group than in the combined press needle + exercise stimulation group. These findings indicate that exercise stimulation provided in conjunction with a press needle tends to reduce the decrease in StO2 during exercise.
In addition, although the ANS does not appear to be involved in skeletal-muscle vasodilation during exercise,15,16 skeletal-muscle blood flow has been reported to be primarily due to local vasodilatory responses that function as a feed-forward mechanism for exercise hyperemia. 17 Therefore, using a press needle + exercise stimulation in the present study may have contributed to this response. No adverse events, such as pain or internal bleeding (caused by the press needles) or itchy skin (caused by the tape) were noted during or after the experiment. Although previous studies have reported the local skin infections, 18 no skin infections occurred in the current study. Thus, the safety of the press needle + exercise stimulation was confirmed.
In terms of changes in the number of knee flexion exercises, it has been reported that intermediate-level trainees have a progressive increase in muscle strength (before and after the intervention) as the number of sets per week increases over the training course. 19 The knee flexion exercises in the present study were performed once per week because they were of a “very hard” intensity. Therefore, participants in the exercise stimulation group and combined press needle + exercise stimulation group were unlikely to be affected by changes in muscle strength over the study duration.
During skeletal-muscle exercise, regulation of blood flow and O2 supply results from integration of many stimuli, including the mechanical effects of contraction, local metabolism and endothelium-derived substances, which are vasoactive factors associated with red blood cells, and the sympathetic nervous system.
It has been reported that when limb O2 uptake increases during muscle activity, vascular resistance decreases rapidly, accompanied by a slight increase in O2 uptake thereafter. 20 Therefore, the lower StO2 and higher total Hb during exercise in the exercise stimulation group, compared to that in the combined press needle + exercise stimulation group may be attributed to vascular conductance. The combined press needle + exercise stimulation group had a decrease in StO2 during exercise but no increase in total Hb. This could be due to the dilatory response of the muscular vessels via the sympathetic nerve fibers. 21
Animal studies have shown that stimulation of group IV afferent fibers of the L2 spinal nerve in anesthetized cats produces action potentials in the ipsilateral L2 white traffic branch. 22 The press needle insertion depth in this study was 1.2 mm and was subcutaneous. This suggests that centrally mediated stimulation caused muscular vasodilation at the level of spinal-cord segments via the somatic autonomic reflex, with the cholinergic nerve in the sympathetic division serving as the centrifugal pathway. Therefore, there may have been increased vascular conductance in this group, compared to that in the exercise stimulation group.
Furthermore, it has been reported that a decrease in cutaneous blood flow due to sympathetic control at the onset of exercise is replaced by cutaneous vasodilation attributed to hypothalamic control as the body temperature rises, resulting in the opening of capillaries in skeletal muscle. 23 Increased cutaneous blood flow with press needle stimulation has been reported to involve calcitonin-related peptide (cGRP), 24 and increased skin blood flow has been shown to increase skin temperature. 25 Press needle stimulation may cause dilation of skin vessels via an axon reflex 26 to the skin, which facilitates the opening of skeletal muscle capillaries and vasodilation.
In terms of the kinetics of muscle deoxygenation during NIRS, it has been reported that, during transient exercise loading, the adaptation rate of local muscle perfusion is slower and more dependent on O2 extraction in older persons, compared to that in younger persons. 27 A decrease in rapid vasodilation with aging due to rapid muscle contraction has also been noted.28,29 While cutaneous vasodilation induced by human press needle stimulation is presumed to involve cGRP, nitric oxide (NO) production is also thought to be important. 30 Current evidence suggests that the production capacity of NO decreases with age, even in healthy people. 31
In the present study, the total Hb during exercise was greater in the exercise stimulation group than in the combined press needle + exercise stimulation group. The desaturation of Hb during exercise indicates that homeostatic regulation is insufficient to maintain constant capillary oxygenation. 6 Furthermore, the extreme progression of desaturation suggests an imbalance between O2 supply and demand. 6 Therefore, using the circular press needle method combined with exercise therapy may be effective for preventing and recovering from muscle fatigue.
Several limitations of the present study must be acknowledged. First, the participants were healthy adults who were not elderly or of an age-specific group. They also did not have any muscle weakness in their knees. Therefore, additional studies are required to evaluate the applicability of combined press needle + exercise for medically compromised patient groups. Second, while measurements were obtained once per week for 3 weeks, the number of exercise sets needs to be increased in future studies to assess simultaneous effects on muscle strength. Given that muscle recovery can be defined as the regaining of strength after exercise, 2 evaluating postexercise muscle strength is necessary. To validate the clinical applicability of combined press needle + exercise stimuli, the effects of continuous and repetitive stimulation, as well as the effects of loading, need to be assessed.
CONCLUSIONS
In this study, the combination of press needles + exercise stimuli prevented a decrease in StO2 and an increase in total Hb versus exercise stimuli alone. The desaturation of Hb during exercise is an imbalance between O2 supply and demand. Therefore, combined press needle + exercise therapy could be effective for preventing and recovering from muscle fatigue. However, this study was conducted on healthy participants. Therefore, further studies investigating the mechanisms of this phenomenon are needed to assess its effectiveness in different age groups and older adults, as well as for patients with knee-muscle weakness.
Footnotes
ACKNOWLEDGMENTS
The authors thank Fumio Karakida, Yoshinobu Mineta, and the participants for their cooperation in this study.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This research received no specific grants from any funding agencies in the public, commercial, or not-for-profit sectors.