
Abstract
Objective:
Viability of inpatient acupuncture is limited by current hospital reimbursement structuring. Research has primarily focused on length of stay (LOS) instead of cost of stay (COS). This study evaluated acupuncture as an option for inpatient pain control, determined if acupuncture influenced patient satisfaction during hospitalization, and examined any effects on LOS and COS.
Materials and Methods:
In a quasiexperimental pilot research study, acupuncture was offered free of charge for 3 months on a single floor of an urban medical center. Pre- and postintervention scores, number of treatments, and diagnosis related groups (DRGs) of patients receiving acupuncture were tracked and then compared to a nonintervention, DRGs-matched group with overlapping hospital-floor and admission dates. LOS, COS, and patient satisfaction scores during the months of intervention were compared to the months before and after the intervention.
Results:
Patients' pain significantly decreased each time they were treated. Consumer Assessment of Healthcare Providers and Systems scores increased to 85, 99, and 97 during the months of intervention and then returned to the lower, preacupuncture levels after acupuncture was no longer available. LOS was higher in the intervention group (+7.8 days), but acupuncture saved the hospital an anticipated $125,770 in the projected COS during that 3-month time alone.
Conclusions:
Acupuncture was a potent pain-relief alternative for hospitalized patients, providing more satisfaction. Acupuncture resulted in longer LOS, but the aggregate COS was 86% less than expected. Acupuncture may be a financially viable, clinically impactful adjunct to hospital care.
INTRODUCTION
As hospitals are faced with Joint Commission requirements to offer nonpharmacologic approaches to pain management, a growing body of evidence indicates that acupuncture is a reasonable treatment modality for many types of pain.1–7 However, if hospitals do not have grants or philanthropic funding, or cannot successfully bill to recover the costs of an acupuncturist's services, this potential solution is often restricted to those with the financial means to pay out-of-pocket. 8
This creates a no-win situation. Hospitals are limited in their options to fulfill the Joint Commission requirements and keep patients satisfied with their hospital stays. 9 Many insurance companies are missing the opportunity to provide their consumers with a low-cost, safe alternative to potentially life-threatening and addictive medications such as opioids and to expensive surgical interventions. Patients without financial means and/or one of the limited number of reimbursable diagnoses (such as low-back pain) often do not have access to a modality with a low risk–benefit ratio and a potent history of efficacy for treating pain. 10
Hospitals are commonly reimbursed for a stay with a single payment, as determined by a patient's diagnosis related group (DRG). 11 * Out of that DRG-determined reimbursement, hospitals must cover the costs of the patient's care: clinician costs, medications administered, meals, housekeeping, laboratory work, radiographic testing, etc.
As a consequence of this reimbursement structure, hospitals are often motivated to discharge a patient sooner, citing a desire to keep the cost of stay (COS) down by equivocating it to length of stay (LOS). To date, research examining the financial benefits of offering acupuncture in a hospital setting has only been evaluated in terms of LOS. Change in COS as an independent marker of financial viability of inpatient acupuncture treatment has not been evaluated in the published medical literature to date.12–17 While the phrase cost of stay is often cited in the title, abstract, or body of an article, the authors of the articles cited above (and many others not cited) are using LOS as a surrogate for COS. However, Taheri et al. have demonstrated that LOS has minimal impact on COS, thus potentially limiting current understanding of how acupuncture might affect actual COS, independent of LOS. 18
Additionally, hospital reimbursement is tied to patient satisfaction scores through a program administered by the Consumer Assessment of Healthcare Providers and Systems (CAHPS) of the Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services.19,20 Press Ganey Associates (South Bend, IN, USA), is a company that performs CAHPS surveys of patients following discharge to determine how satisfied they were with their stays. 21 The patients fill out a Likert scale (1–5, with 5 being best) and that is converted to a 1–100 scale when reported to a hospital (100 being best). The hospital's scores are then compared to a national cohort of similar hospitals and reported to the hospital of interest as a percentile. A score of 70, for example, means that the hospital is in the 70th percentile, when compared to a national cohort of similar hospitals. These scores are then used to impact percentage of reimbursement. To date, no identifiable studies have evaluated the impact of acupuncture on patient satisfaction as measured by CAHPS scores.
Finally, although many studies have examined acupuncture's efficacy for particular biomedical symptoms or diagnoses, to the current authors' knowledge, no work has been performed to evaluate acupuncture's effect on a variety of pain complaints of hospitalized patients.
This study was performed to investigate if acupuncture is an effective modality for treating pain of all types in a hospitalized patient population; to evaluate the capacity of inpatient acupuncture to influence patient satisfaction during hospitalization as measured by CAHPS scores; and to determine if, on a single hospital floor, COS and LOS tracked together for patients receiving acupuncture, compared to those that did not.
MATERIALS AND METHODS
A quasiexperimental research design was used at an urban, teaching hospital to evaluate 15–20 minutes of voluntary acupuncture performed at patients' bedsides by 2 licensed acupuncturists on patients hospitalized for any reason on a mixed medical, surgical, oncologic floor. The acupuncture team members (the current authors), both National Certification Commission for Acupuncture and Oriental Medicine–certified licensed acupuncturists (1 who was additionally boarded in medical acupuncture) with >9 years of experience at the time of the study, offered their services free of charge to patients and were not reimbursed by the hospital for their time. The acupuncturists received no financial support and paid for all supplies used, including their own needles, out-of-pocket.
The study was performed from June to the end of August because this was deemed to be an adequate time to demonstrate monetary effects and because the acupuncture team members were willing to donate up to 3 months of their time.
Patients were identified by nursing or physician staff as possible candidates for acupuncture and consented to receive care by a member of the acupuncture team. There were no participant eligibility criteria other than a desire to receive acupuncture and availability of the patient for treatment while the acupuncturists were working at the hospital. No harm or unintended consequences were noted for any patient participating in the study aside from minor bleeding at an occasional acupoint; the bleeding was stopped with minimal pressure.
If a patient consented to treatment, acupuncture was initiated on the patient at any time during the hospitalization, and acupuncture was continued until discharge or until the patient no longer wished to receive it (i.e., the patient's complaint resolved). All treatments were performed and all numeric pain rating scale (NPRS) data were collected at the patient's bedside in that patient's hospital room. Data on COS and LOS were acquired by the hospital administration and provided to the acupuncture team. Data on CAHPS results were acquired by the charge nurse on the relevant floor and provided to the acupuncture team.
Acupuncture points were not preselected but were instead chosen as a clinician would use them in typical practice: the points were selected according to traditional East Asian medicine principles and diagnostic techniques according to the patient's individual needs at the time of treatment. The needles were placed to a depth confirmed by the De Qi sensation and were retained for ∼15–20 minutes. DBCtm 0.16 x 30-mm needles (Lhasa OMS, Weymouth, MA, USA) were used for body points, and DBC hand needles used for auricular points. Techniques included only cutaneous or auricular needling; no-cupping, gua sha, moxibustion, or additional ancillary traditional East Asian medicine techniques were used.
Patients receiving acupuncture were tracked by number of treatments and categorized by DRGs. DRGs were used to compare groups of patients who received acupuncture with those that did not for LOS and COS. Both groups were hospitalized on the same hospital floor and during the same 3-month time. The hospital provided data on real and projected LOS and COS for all relevant patients following their discharges.
Pre- and postintervention scores of patient's primary complaints or concerns were obtained verbally by the acupuncture team using a 10-point NPRS and compared using paired Students t-tests. CAHPS scores for the hospital floor were analyzed using simple descriptive statistics, as were LOS and COS. Data analysis was performed, using Stata software (StataCorp, College Station, TX, USA). †
Ethics
At the time of the study, the hospital was interested in allowing the acupuncturists to perform acupuncture at the bedside as a quality-improvement experiment, not as a human-subjects research study. The outcomes measures were designed as cost–benefit analyses. The acupuncture itself was not considered experimental. The study was presented to the hospital's institutional review board committee and was approved as exempt because the research was conducted on the cost–benefit analysis of the program retrospectively after the program was concluded.
RESULTS
A total of 78 patients received at least 1 acupuncture treatment. Of those, 6 were missing data and 72 had accurate recorded pre- and postintervention scores for their chief complaints. The mean age of hospitalized patients treated with acupuncture was 58. Other demographic data were not obtained or recorded, as the acupuncturists were not given access to the hospital's electronic medical records.
All of the patients' primary complaints were pain. Prior to treatment, patients rated their pain levels on a 10-point NPRS scale. The mean score was 7.08 (standard deviation = 2.29; n = 72). After a single course of acupuncture treatment, patient pain levels decreased from 7.08 to 2.82 (t = 13.37; p < 0.001; n = 72). Of these 72 patients, 31 would receive additional treatments.
In patients who received only 1 acupuncture treatment during the hospitalization, their pain levels decreased significantly with acupuncture treatment from 7.07 to 2.90 on a 10-point NPRS scale (t = 10.64; p < 0.001, n = 41). See Figure 1.
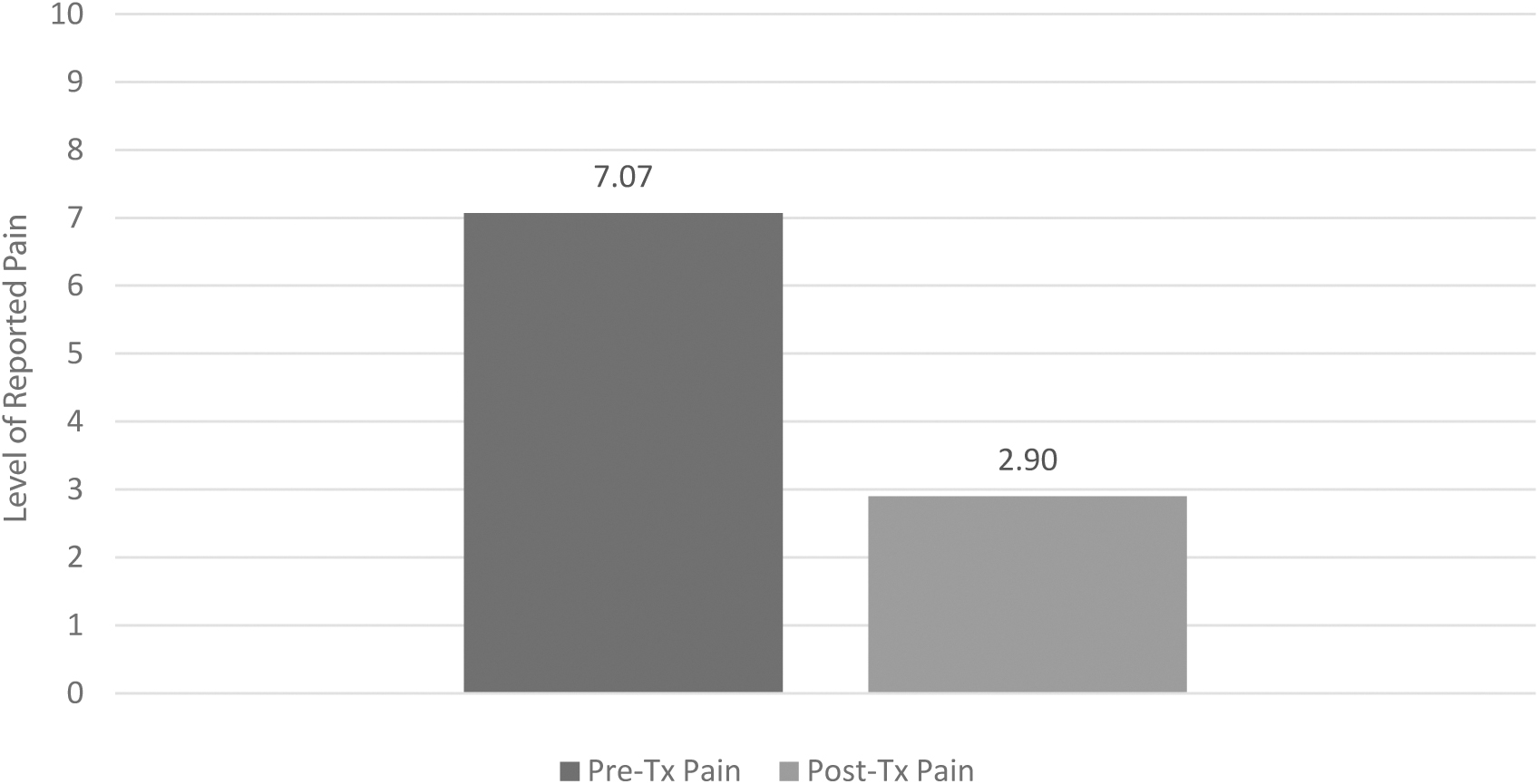
Change in pain scores before treatment (Pre-Tx) and after treatment (Post-Tx) for patients who received 1 acupuncture treatment only during the entire hospitalization (t = 10.64; p < 0.001; n = 41).
In patients who received 2 treatments (n = 31), pain levels decreased significantly from 7.13 to 2.71 (t = 7.98, p < 0.001, n = 31) on the first day of treatment and from 6.73 to 2.23 (p < 0.001, n = 26) on the second day of treatment. See Figure 2.
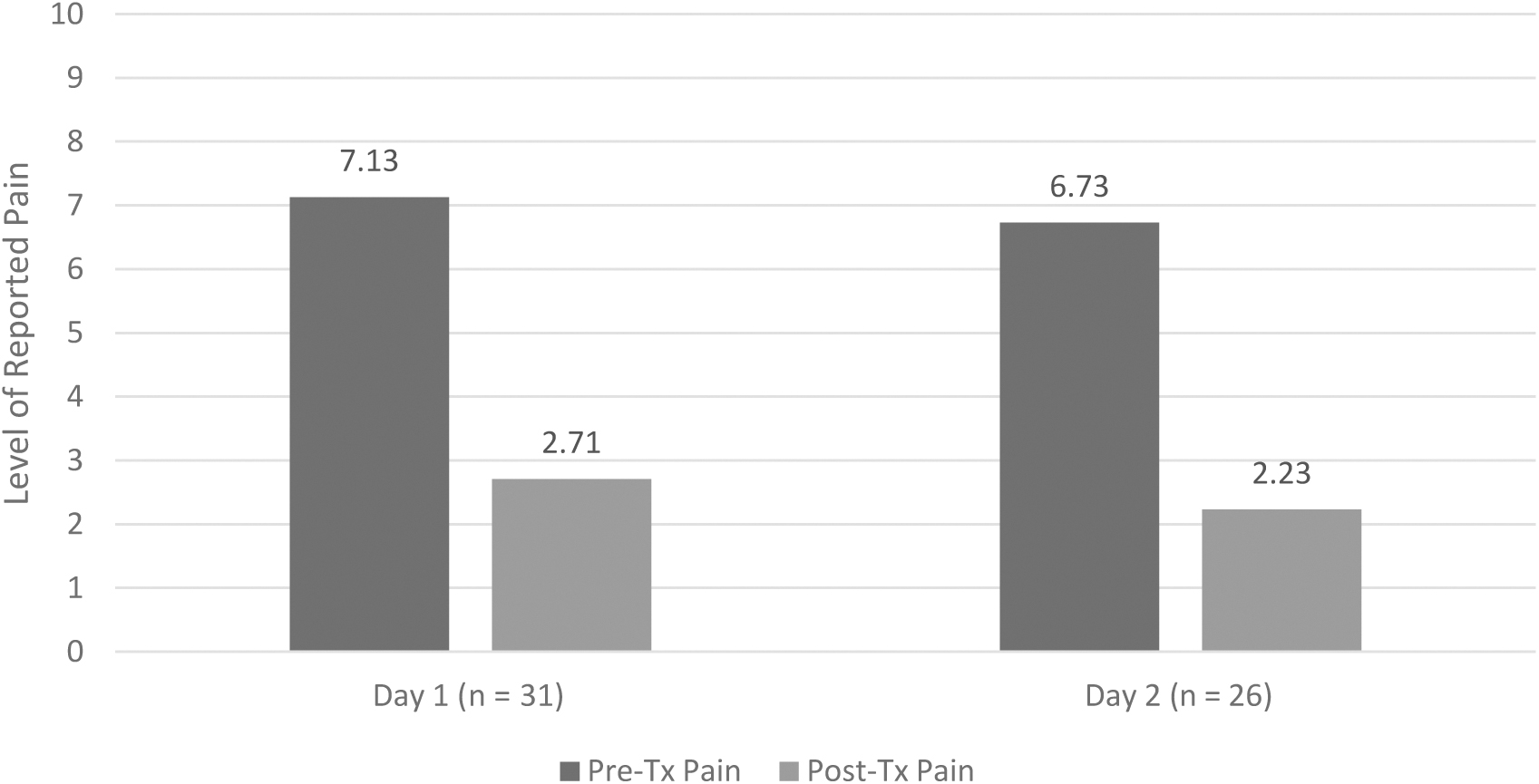
Change in pain scores before treatment (Pre-Tx) and after treatment (Post-Tx) for patients who received 2 acupuncture treatments during the hospitalization (day 1: p < 0.001; day 2: p < 0.001).
In patients who received more than 2 treatments, the change in chief complaints could not be analyzed due to the low numbers of patients receiving more than 2 treatments and due to missing pre- or postintervention scores for subsequent treatments for these patients.
Prior to acupuncture, CAHPS scores for the hospital floor were consistently in the high 50s and low 60s as reported by the charge nurse for the floor. The researchers were not permitted to view these preintervention scores themselves but had to rely on reporting of the charge nurse. CAHPS scores increased to 85, 99, and 97 during the 3 respective months of acupuncture intervention (scores released to—and validated by—the acupuncture team) and then returned to the much lower, preacupuncture intervention levels after the acupuncture service team was no longer available, as reported to the team by the charge nurse.
With data obtained from the hospital following patients' discharges, evaluations were performed of the COS and LOS between patients who received acupuncture and a comparison group who did not receive acupuncture but had matching DRGs and were hospitalized during the same months on the same hospital floor. Of the 72 acupuncture-treated patients, 25 were DRG-matched to patients who did not receive acupuncture but were in the hospital on the same floor during the same time. For these 25 patients, the aggregate LOS was longer by 7.8 days, but the aggregate COS was $125,770 (86%) ($125,700 less than expected). See Table 1.
Comparison of Length of Stay and Cost of Stay by Diagnosis Related Group for Patients Receiving Acupuncture and for Controls
Patients were categorized by DRG and compared between groups who received acu (treatment; n = 25) and those who did not (control; n = 203). DRGs with only 1 patient receiving acupuncture were excluded from the analysis. Average real and projected LOS in the treatment and control groups were compared as were real and projected COS. Average LOS was higher than projected (7.8 days) in the intervention group, but actual (real) COS was lower than projected by $125,770.
DRG(s), diagnosis related group(s); acu, acupuncture; LOS, length of stay; COS, cost of stay; COPD, chronic obstructive pulmonary disease; CC, complication or comorbidity; sm, small; lg, large; proc, procedure; MCC major complication or comorbidity; CDE, common duct exploration; LE, lower extremity; UTI, urinary-tract infection; nonmalig, nonmalignant; hrs, hours; MV, mechanical ventilation.
DISCUSSION
This study evaluated the effect of acupuncture on COS and LOS on a mixed hospital floor for 3 months. An attempt was made to mitigate confounders of changes in nursing staff, hospital staff, medical staff, or ancillary staff by using a single hospital floor over a set 3-month time duration and by comparing acupuncture recipients to those on the same floor, with the same providers during the same time, who did not receive acupuncture.
Change in patient satisfaction as measured by CAHPS scores correlated with the availability of an acupuncturist on the hospital floor. However, the acupuncture team was not provided with the actual dollar amount that this radical change in CAHPS scores generated.
Anecdotally, the charge nurse for the relevant floor relayed that there was more than 1 situation in which patients were threatening to sue or to transfer to another hospital until she offered acupuncture as an alternative to their underlying complaints (pain). Once offered, each patient and/or patient's family declined to take legal action or to transfer, and, instead, were treated successfully and satisfactorily with acupuncture. It is possible that because patients' experiences were improved and because there were alternative modalities offered to control complaints per the anecdotal comments noted above, patient satisfaction scores improved. There were no other administrative, nursing, or medical staff changes nor other known alternations in floor routines or initiatives for this time duration that might otherwise have accounted for such a dramatic shift in patient satisfaction.
While the days of acupuncture treatment were tracked, there was no attempt to correlate the day of hospitalization with the day that acupuncture treatment was initiated or with the anticipated date of discharge. Based on a retrospective review of patient records, it appears that the acupuncture team was consulted only after LOS began to rise. It is impossible to know this definitively, however, and that was the first limitation of this study.
A second limitation of the study was that the reasons for the extended LOS in the treatment cohort were not evaluated. However, it was observed that patients who responded well to standard care were not generally referred to the acupuncture team. The hospital staff tended to consult the acupuncture team when a patient's pain was not otherwise controlled with usual care, when a patient was dizzy or walking unsteadily, when insomnia was preventing recovery or becoming a problem for night staff, when the patient had some form of gastrointestinal distress, etc.
A third limitation was that, because all of the complaints discussed above can prevent discharge, it was likely that there was selection bias in the patients who received acupuncture over those that did not. Clinically, it is logical that the acupuncture team was consulted specifically because patients were not progressing as anticipated or recovering quickly from the medical or surgical indications for their hospitalizations. Because these patients were experiencing problems that would delay discharge, it is not surprising that patients in the acupuncture cohort had longer LOS in this nonrandomized study. It is precisely this situation that makes it more remarkable that the COS was so much lower than anticipated in the acupuncture group; due to these patients' extended LOS, they likely would have required more hospital resources without acupuncture intervention. A randomized trial would help evaluate this potential area of bias and some or all of the associated real or anticipated costs.
An area for further investigation would be whether acupuncture treatment would have a preventative effect on lowering COS and LOS when acupuncturists were consulted earlier during patients' hospitalization. These investigations would help address some of the issues identified by the Patient Centered Outcomes Research Institute–funded stakeholder conversation convened in 2021 regarding implementation of acupuncture into American health care. 22
The complexities of the subcategories of the DRG system made it challenging to match patients who had acupuncture precisely to those who did not during the same time and on the same floor. A fourth limitation of this study was that many more patients were treated during this time than was indicated by this study, but comparison was limited due to difficulty with creating appropriate cohorts as controls. Future investigations should include greater numbers of enrolled patients, longer study durations, and multiple locations throughout the hospitals—including more-complex levels of care, such as an intensive care unit—to determine if acupuncture intervention can decrease the direct COS (and not just the LOS as a surrogate for the COS).
This study demonstrated that acupuncture is an effective tool for mitigating pain, corroborating previously published studies. Due to limitations on the number of hours and months that the acupuncture team could donate to the project, the team was only able to be in the hospital for ∼4 hours in the morning, 5 days per week, for 3 months. It was therefore not possible to measure the length of time that acupuncture provided pain relief for the patients. Some preliminary data from an unpublished but related study suggests that the pretreatment chief complaint levels were significantly diminished on treatment day 2 (more than expected even in postsurgical patients) and again on day 3, but the limited number of subjects involved prevented statistical evaluation.
Additional limitations of this study included inclusion of a single hospital floor, inability to track all staff conclusively that may have had an effect on patient satisfaction (e.g., phlebotomy, admissions, janitorial staff, etc.), potential bias in the delay in patients responding to the CAHPS questionnaire for indeterminate times following discharges, inability to access the CAHPS data directly, and the lack of transparency regarding the degree to which CAHPS scores affected overall COS for the time of the study. 23
CONCLUSIONS
The current study demonstrates that patient pain was controlled due to 15–20 minutes of acupuncture performed at the bedside during inpatient hospitalization. During the same time that the acupuncture team was present in the hospital, patient satisfaction scores improved radically and then returned to their previous, much lower, levels after acupuncture was no longer available to hospitalized patients. Finally, the aggregate COS for patients who received acupuncture compared to those DRG-matched patients who did not receive acupuncture saved the hospital $125,770 over 3 months—a sum that could cover, at least in part, the salary of 1 full-time acupuncturist for an entire year. The results of this study support using acupuncture in the inpatient setting, improving clinical outcomes and patient satisfaction while reducing financial burden on the health care system.
Footnotes
ACKNOWLEDGMENTS
The authors wish to acknowledge the assistance and support of Collin Hitt, PhD, for his assistance with statistical analysis; of Abby Falbo, RN, for her assistance on the hospital floor; and of Paul Romito, Manager, Medical Staff Services without whose support this study would never have been possible.
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
No funding was provided for this project.