
Abstract
Introduction:
Patients with chronic pain and high-level catastrophic thoughts often do not respond to acupuncture. This may be related to hypofunctioning of the dorsolateral prefrontal cortex and the descending pain inhibitory system. Therefore, we examined the relationship between the level of catastrophic thinking and the analgesic effect of electroacupuncture using the pain catastrophizing scale (PCS). We also evaluated the descending pain inhibitory system using conditioned pain modulation (CPM) and offset analgesia (OA). The relationship between catastrophic thinking and the descending pain inhibitory system was also examined.
Materials and Methods:
After testing the hospital anxiety and depression scale and the PCS in 14 healthy adults, the current pain threshold (CPT), CPM, and OA were measured, in order, before the intervention. Thereafter, electroacupuncture was applied to 3 limbs (the dominant hand and both lower extremities) at 4 Hz, and to the scalp at 100 Hz, for 30 minutes, and the CPT was measured again immediately after the intervention. The difference in the CPT before and after the intervention was taken as the analgesic effect.
Results:
The participants were divided into 2 groups, the H-PCS group (≥16 points) and the L-PCS group (≤15 points), according to the PCS score, and the analgesic effects of electroacupuncture were significantly different (P = 0.04). However, no relationship was found between the PCS score and the CPM (r = −0.02, P = 0.94) and OA effects (r = −0.19, P = 0.49).
Conclusion:
It was suggested that people with high-level catastrophic thinking may find it difficult to obtain the analgesic effects of electroacupuncture.
INTRODUCTION
Chronic pain is defined as pain that persists beyond the normal course of acute illness or a reasonable time for wound healing; 1 a study by the Centers for Disease Control and Prevention in the United States has reported a prevalence of 20.4% for chronic pain. 2 There are various factors that cause pain to become chronic, and recent functional magnetic resonance imaging (fMRI) studies have reported modulation 3 of brain regions associated with pain and the associated attenuation of endogenous analgesic mechanisms, such as the descending pain inhibitory system.4,5
Chronic pain management requires multidisciplinary treatment, including acupuncture and moxibustion therapy, which have been shown to be effective for various chronic pain disorders.6,7 Electroacupuncture is often used in acupuncture and moxibustion treatment for chronic pain, and is thought to suppress pain through endogenous analgesic mechanisms, such as the descending pain inhibitory system. 8 However, clinical acupuncture and moxibustion do not show therapeutic effects in some patients.
One of the reasons for this is catastrophic thinking. Catastrophic thinking is negative thoughts about pain, and it is said that excessive attention to pain, and the associated negative thoughts, makes the pain stronger or causes inactivity to avoid the pain, which exacerbates the pain. 9 Therefore, catastrophic thinking is thought to be an important factor in the chronicity of pain, causing pain to persist for long periods. 9 Catastrophic thinking is also associated with pain prediction (medial prefrontal cortex and cerebellum)10,11 and pain attention (dorsal anterior cingulate cortex and dorsolateral prefrontal cortex [DLPFC]). 11
The DLPFC is particularly involved in the descending pain inhibitory system, suggesting that catastrophic thinking affects the descending pain inhibitory system. 12 In refractory chronic pain, such as that in fibromyalgia, catastrophic thinking tends to be intense, and it has been suggested that the descending pain inhibitory system may be functioning abnormally due to hypofunction or a disorder in the brain network. 13 Therefore, in patients with chronic pain who do not respond to acupuncture and moxibustion treatment, the descending pain inhibitory system and other endogenous analgesic mechanisms may not be functioning properly and, as a result, therapeutic effects may not be observed.
However, in recent years, quantitative sensory tests (QSTs), such as conditioned pain modulation (CPM) 4 and offset analgesia (OA), 5 have been used as indices for quantitative evaluation of endogenous analgesic mechanisms, such as the descending pain inhibitory system. CPM is a diffuse noxious inhibitory control (DNIC) phenomenon in humans that suppresses pain by a noxious stimulus, 14 and OA is a phenomenon in which a slight decrease in a noxious heat stimulus significantly reduces pain sensation. 15 It has been reported that CPM and OA are attenuated in patients with chronic pain compared with healthy participants,16,17 suggesting that the function of the descending pain inhibitory system is impaired.
Therefore, in this study, we investigated the effect of catastrophic thinking on the analgesic effect of electroacupuncture, and also examined the relationship between catastrophic thinking, CPM, and OA.
MATERIALS AND METHODS
Participants
The participants were 14 adults (age 22.5 ± 2.0 years, 10 men and 4 women) who gave their informed consent. In addition, individuals who had experienced chronic pain for >3 months in the past were eligible for inclusion; those with heart, neurologic, or mental diseases, and those taking drugs that could affect the study results were excluded. The study was approved by the Meiji University of Integrative Medicine Human Research Ethics Review Committee (#2022-007).
Measurement/Evaluation
For psychological evaluation, anxiety and depression were evaluated using the Japanese Hospital Anxiety and Depression Scale (HADS). HADS consists of 7 questions each on depression and anxiety, and the evaluation was performed using a 4-step scale of 0 to 3 points. A score of 11 or higher for total score indicated a high degree of anxiety or depression. 18
In cognitive evaluation, catastrophic thinking (rumination, expansion, and helplessness) was evaluated using the Japanese version of the Pain Catastrophizing Scale (PCS). The PCS consists of 13 questions and is rated on a scale of 0–4 points. The total score is 52, with higher scores indicating stronger catastrophic thinking. 19
Quantitative Sensory Testing
CPM and OA were used to assess the descending pain inhibitory system. The intensity of pain when measuring CPM and OA was measured using a visual analogue scale (VAS), where the left end was “no pain” and the right end was “worst imaginable pain,” and the participants were asked to mark it on a 100 mm wide line, which was then evaluated.
CPM uses a thermometer (UDH-105; unique Medical, Japan) for the test stimulation (TS) to measure the outside of the nondominant upper arm. The probe area was 5 mm2. Heat stimulation was gradually increased, and the temperature at which the VAS reached 50 mm was measured. The temperature at this time was set as the heat pain threshold = TS. After that, TS was performed for 1 second on the lateral upper arm of the nondominant hand, and the intensity of pain was evaluated by VAS (VAS 1).
After an interval of 2 minutes, the participant was instructed to immerse his/her dominant hand in cold water (10°C) for 10 seconds (up to the wrist) as a conditioned stimulus simultaneously with the TS, and VAS was measured on the outer side of the nondominant upper arm immediately after releasing the hand (10 seconds) (VAS 2). The CPM effect was expressed as an arbitrary unit (AU), with reference to past studies, 20 and the value obtained by the following equation was referred to as the CPM effect: −{(VAS 2)/(VAS 1) − 1} × 100.
For OA, a thermal dolorimeter was used to fix the baseline at 33°C, followed by a thermal stimulus of 43°C for 5 seconds (T1), 44°C for 5 seconds (T2), and 43°C for 20 seconds (T3), for a total of 30 seconds. The temperature increase rate was 0.25°C/s. Pain intensity was evaluated by VAS every 5 seconds during the 30 seconds, from T1 to T3, and the difference between the maximum VAS (VASmax) and minimum VAS (VASmin) was defined as ΔOA. The OA effect was expressed as an AU, which was determined by the following formula with reference to past reports 5 : (ΔOA/VASmax) × 100.
Analgesic Effect of Electroacupuncture
The current pain threshold (CPT) was measured using Pain Vision PS-2100 (NIPRO, Japan) to measure the medial central part of the nondominant forearm. The participant was instructed to press the switch if he/she felt pain. The amount of current at this time was taken as CPT, and the average value of 2 sessions was taken as the representative value. Measurements were taken before and after the intervention, and the difference in CPT values before and after the intervention was taken as the analgesic effect of electroacupuncture.
Intervention
Using the Ohm Pulser LFP-4000A (manufactured by Zeniryoki, Japan), electroacupuncture was applied to 3 limbs, namely, the dominant hand and both lower extremities, and the scalp. Electroacupuncture was performed on the forearm of the dominant hand (LI10), between the base of the thumb and index finger of the dominant hand (LI4), and on both lower extremities (ST36, GB34) at a depth of 5–20 mm from the skin and a frequency of 4 Hz. Electroacupuncture was applied to the upper left and right sides of the forehead (ST8) at a depth of 10–20 mm from the skin and a frequency of 100 Hz.
The stimulation intensity was such that the participants could clearly feel the electrical stimulation on all 3 extremities and the scalp, and the stimulation time was 30 minutes. The acupuncture needles used were 40 mm/No. 2 and 50 mm/No. 2 stainless steel needles (Seirin, Japan) for the 3 extremities and the scalp, respectively.
Study Design
For all the participants, HADS and PCS were evaluated in advance, and as preliminary practice, the participants experienced all CPT, OA, and CPM measurements as in this experiment, and then participated in the experiment 1 to 2 days later. In this experiment, after measuring the participants' CPT, OA, and CPM, electroacupuncture was performed for 30 minutes in the supine position, and CPT was measured again immediately thereafter (Fig. 1). Based on previous reports, 21 the participants were divided into 2 groups, the H-PCS group (≥16) and the L-PCS group (≤15), according to the PCS score, and the analgesic, OA, and CPM effects of electroacupuncture were evaluated.

Study protocol. This figure shows the study protocol. This study was conducted in 2 stages: a training session and a test session. In the training session, after informed consent was obtained, hospital anxiety and depression scale and PCS evaluations were performed before measurement; CPT, OA, and CPM were measured in order as practice; and a test session was conducted in the same manner 1–2 days later. In the test sessions, CPT, OA, and CPM were measured before the intervention; and CPT was measured again immediately after the intervention. CPM, conditioned pain modulation; CPT, current pain threshold; OA, offset analgesia; PCS, pain catastrophizing scale.
Statistical Analysis
Numerical values are expressed as medians (first quartile to third quartile), and the difference in CPT before and after intervention was analyzed as the analgesic effect of electroacupuncture. Stat View Ver.5.0 (SAS Institute, Inc., Japan) was used for statistical processing, and the Mann–Whitney U test was used for comparison between groups. Spearman's rank correlation coefficient was used to evaluate the correlation between the psychocognitive evaluation and the analgesic effects of electroacupuncture, OA, and CPM. The significance level was <5%.
RESULTS
Participants Characteristics
Table 1 gives the characteristics of the participants before the intervention. The age of the 14 participants was 22.0 (21.3–23.0) years, the HADS score was 7.0 (4.5–10.3) points, and the PCS score was 15.0 (5.0–23.0) points. In the H-PCS group (n = 7), PCS was 23.0 (21.0–26.0) points and HADS was 7.0 (5.0–7.5) points. In the L-PCS group (n = 7), PCS was 4.0 (0.0–8.5) points and HADS was 7.0 (5.0–11.0) points. Before intervention, CPT (P = 0.18), CPM (P = 0.56), and OA (P = 0.72) were not significantly different between the 2 groups.
Participants' Characteristics Before the Intervention
Grouping by PCS score: H-PCS (≥16 points), L-PCS (≤15 points).
Obtained using Mann–Whitney U test.
AU, arbitrary unit; CPM, conditioned pain modulation; CPT, current pain threshold; HADS, hospital anxiety and depression scale; OA, offset analgesia; PCS, pain catastrophizing scale.
Relationship Between PCS and the Analgesic Effect of Electroacupuncture
There were no significant correlations between PCS and analgesic effects across the participants (r = −0.40, P = 0.15, Fig. 2A). However, the analgesic effect in the H-PCS group was −3.75 (−9.60 to −0.55) μA and that of the L-PCS group was 10.10 (3.93–13.43) μA, indicating a significant difference between the 2 groups (P = 0.04, Fig. 2B).
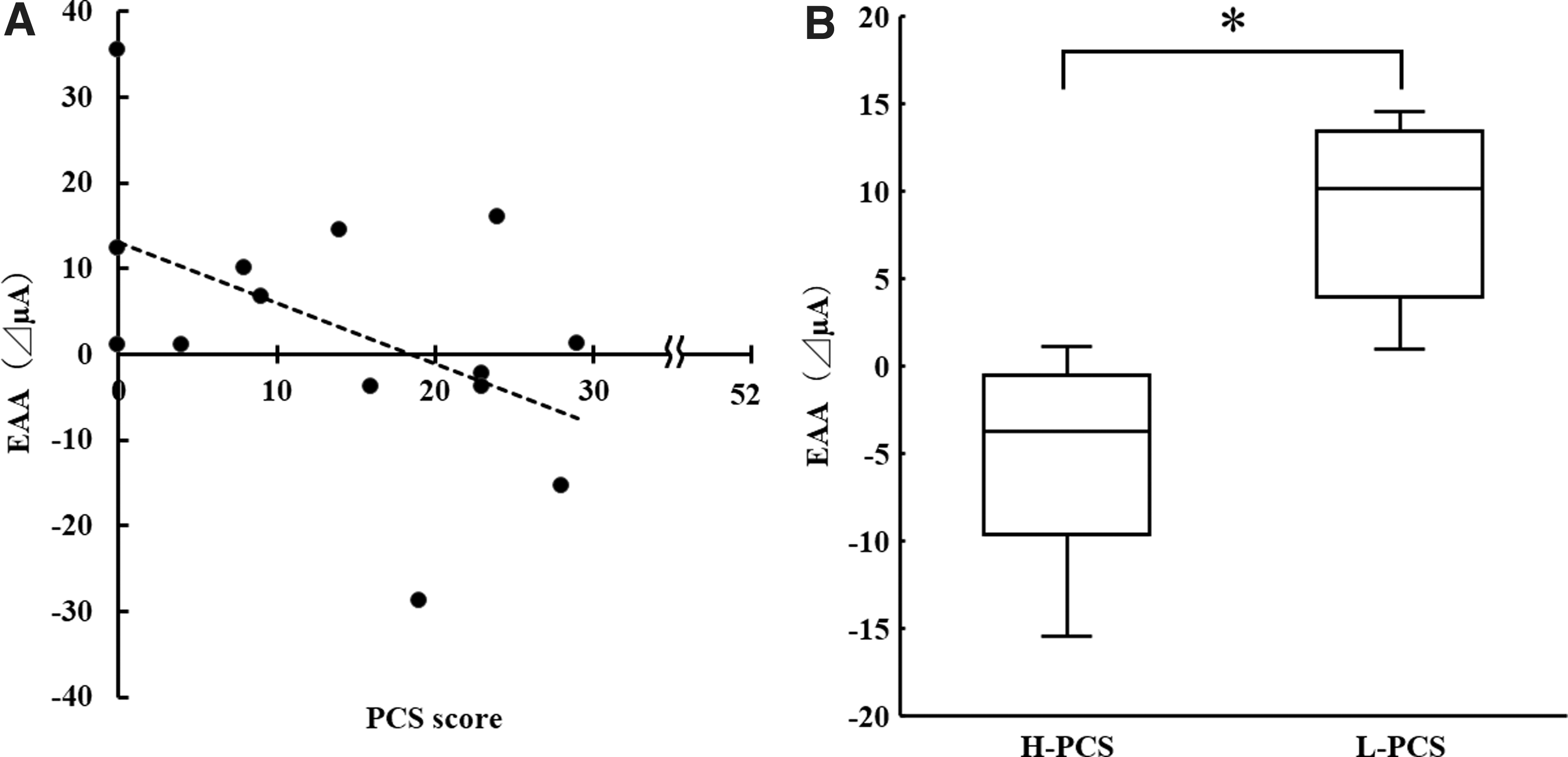
Relationship between PCS and the EAA effect.
Relationship Between PCS and QST
There was no significant correlation between PCS and OA across the participants (r = −0.19, P = 0.49, Fig. 3A). In addition, the OA of H-PCS group was 100.00 (90.84–100.00) AU, and the OA of L-PCS group was 100.00 (96.54–100.00) AU, with no significant difference between the 2 groups (P = 0.72, Fig. 3B).

Relationship between PCS and OA.
There was no significant correlation between PCS and CPM in all participants (r = −0.01, P = 0.97, Fig. 4A). The CPM of H-PCS group was 77.36 (67.54–92.50) AU and that of L-PCS group was 76.60 (55.77–84.27) AU, with no significant difference between the 2 groups (P = 0.56, Fig. 4B).

Relationship between PCS and the CPM effect.
DISCUSSION
Relationship Between the PCS and the Analgesic Effect of Electroacupuncture
Catastrophic thinking has been shown to be related to pain intensity, psychological distress, and pain persistence, and has been shown to be an important factor in chronic pain. 9 Catastrophic thinking can be evaluated by PCS, and it has been reported that even those without pain who have a high PCS score are more likely to develop low back pain in the future, and tend to develop chronic pain. 22 In refractory chronic pain, such as fibromyalgia, catastrophic thinking tends to be strong and difficult to treat.
Therefore, catastrophic thinking is one of the factors that must be considered in the treatment of chronic pain. 16 Furthermore, catastrophic thinking has been reported to be associated with various brain regions associated with pain perception10,11 and pain regulation.3,11,12,23 In particular, the DLPFC is involved in pain regulation, such as through the descending pain inhibitory system,12,23 suggesting that abnormalities in the functioning of the DLPFC may lead to dysfunction of the descending pain inhibitory system.
In contrast, in acupuncture treatment for chronic pain, electroacupuncture to the hands and feet is effective, and it is said that electroacupuncture has analgesic action by activating the descending pain inhibitory system through endogenous opioids and the serotonin–noradrenaline system. 8 As mentioned above, catastrophic thinking is involved in pain regulation, such as the descending pain inhibitory system, so a high level of catastrophic thinking makes it difficult for the descending pain inhibitory system to work. Therefore, in this study, the H-PCS group was considered to have experienced a lower analgesic effect than the L-PCS group did. These findings suggest that catastrophic thinking may affect the analgesic effect of electroacupuncture.
Relationship Between PCS and QST
QST is divided into 2 categories. Static-QST assesses somatic sensations such as tactile, vibration, and heat and cold sensations, as well as pain thresholds such as tenderness, heat, and cold pain. Dynamic-QST assesses the function of pain regulation in the central nervous system. 24 CPM is one of the Dynamic-QSTs, and Yarnitsky et al. proposed in 2010 that the DNIC phenomenon in humans be referred to as CPM. 14 Since CPM suppresses pain systemically, regardless of the stimulation site, it is thought to be a supraspinal analgesic mechanism 4 and is said to reflect the descending pain inhibitory system. 4
In recent years, OA has also attracted attention. 5 OA is a phenomenon in which even the slightest reduction in noxious thermal stimuli results in a significant reduction in pain sensation. 15 Recent fMRI studies have reported activity in brain regions associated with the descending pain inhibitory system during OA.5,17 Like CPM, OA is endogenous to the descending pain inhibitory system, and is used as an index reflecting the analgesic mechanism.5,17
CPM and OA have been shown to be associated with the brain regions involved in pain regulation, such as mesocentric gray matter (e.g., periaqueductal gray, DLPFC),5,25 and the brain regions involved in pain perception, such as the primary somatosensory region. 25 It has been reported that CPM and OA are attenuated in patients with chronic pain compared with healthy participants,16,17 suggesting that the function of the descending pain inhibitory system is impaired.4,5,17
In contrast, it has been suggested that the descending pain inhibitory system may be less active in patients with chronic pain and strong catastrophic thoughts. 26 It has also been reported that PCS, which evaluates catastrophic thinking, may be a predictor of chronic pain >3 months after surgery, 27 and there are several similar reports for QST.28,29 So PCS and QST are considered to be associated; however, no significant association was found in this study. A previous meta-analysis examining the relationship between PCS and CPM also reported that there was no association, 30 but suggested that the results may differ depending on the stimulus conditions for CPM.
However, no definite opinion has been obtained. In addition, it has been suggested that the results of OA may differ depending on the stimulus conditions. 31 Therefore, the possibility that the measurement conditions may have influenced this study cannot be ruled out, and further investigation of catastrophic thinking and QST is necessary.
Relationship Between the Analgesic Effect of Electroacupuncture and QST
Various methods of acupuncture analgesia are used at the peripheral,32,33 spinal cord, 34 and supraspinal cord levels,8,35 but analgesia by electroacupuncture to the hands and feet is thought to be primarily mediated through the descending pain inhibitory ssystem. 8 The descending pain inhibitory system is said to produce an analgesic effect through the action of neurologic factors, such as the serotonin–noradrenaline system, and humoral factors, such as endogenous opioids. 36
Chang et al. compared the analgesic effects of electroacupuncture at different frequencies and found that similar analgesic effects were obtained at all frequencies, but reported that an inhibitory effect by p-chlorophenylalanine, a serotonin synthetic inhibitor, was possible only at 100 Hz. 37 Furthermore, Cheng and Pomeranz have shown that the lower the frequency, the longer it takes for the onset of the analgesic effect. 38 Another study reported that the analgesic effect of low-frequency electroacupuncture lasted longer for 60 minutes rather than 15 minutes. 39
This study applied 30 minutes of low-frequency acupuncture stimulation, and the analgesic effect was measured 30 minutes or more after the stimulation, so the effect of analgesia through humoral factors was considered to be greater than that through neurologic factors.
In contrast, CPM, which is thought to reflect the descending pain inhibitory system, has been reported to be activated by serotonin–noradrenaline reuptake inhibitors (SNRIs), 40 suggesting the involvement of neurologic factors, such as monoamines. Also, recent fMRI studies have shown that OA activates brain regions involved in the descending pain inhibitory system, 5 suggesting that central mechanisms are involved, but OA is associated with SNRIs, 41 and since it has been reported to be unchanged by the opioid antagonist (Naloxone), 42 the detailed mechanism remains unknown.
However, the effect of neurologic factors may be greater than that of humoral factors such as opioids, which require a certain stimulation time to develop analgesic effects, because OA reduces pain sensations instantly with slight stimulation.
Based on this, it is possible that the descending pain inhibitory system activated by electroacupuncture and the descending pain inhibitory system reflected by CPM and OA partially reflect different factors. However, it is unclear whether neurologic and humoral factors in the descending pain inhibitory system act separately, and further investigation is required.
Limitations
Although CPM and OA, used in this study, are considered to be indicators that reflect the descending pain inhibitory system, there are no specific measurement conditions (type of stimulus, stimulus duration, etc.) for them, and the need for such an investigation has been mentioned.30,31 Therefore, the appropriate measurement conditions for CPM and OA used in this study, and the mechanism to be considered from the results, need to be examined further. Other study limitations may include the small number of participants and nonsex uniformity. Although significant differences in age were observed between the H-PCS and L-PCS groups in this study, they were slight and the effect was considered minimal. Moreover, CPM and OA have been suggested to attenuate in older adults. 25 Therefore, it is necessary to investigate a wide range of age groups.
In addition, since it is unclear how much the descending pain inhibitory system was affected by the degree of PCS in this study, detailed investigation of brain function by fMRI is also necessary. Furthermore, to verify the results of this study, it is necessary to investigate different stimulation frequencies, stimulation times, and evaluation timings.
CONCLUSIONS
The analgesic effect of electroacupuncture may differ, depending on the status of catastrophic thinking, and the analgesic mechanism activated by electroacupuncture may occur by a mechanism different from that of CPM and OA. However, since the number of participants in this study was small, the number of participants needs to be increased to further examine the findings in the future.
Footnotes
ACKNOWLEDGMENTS
We express our sincere gratitude to Shinsaku Ozeki, Ryosuke Shima, Megumi Nakamura, and Yuya Harano for their cooperation in the conduct of this study. We thank Editage for English language editing.
AUTHORs' CONTRIBUTIONS
The draft study protocol was prepared by S.H. and adopted with some modifications under the guidance of S.S. and K.I. Data collection was carried out mainly by S.H., and partly with the cooperation of M.O. Data analysis and statistical analysis were performed by S.H. under the guidance of K.I. The article was drafted by S.H., who then prepared the final article with reference to all coauthors' comments. In addition, the English text was proofread by Editage. All coauthors approved the final article for publication.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.